
Abstract
The irrefutable consequence of Scottish excessive alcohol consumption has prompted implementation and proposal of alcohol policy measures. The purpose of this study is to explore with heavy drinkers their awareness of and identify potential implications of policy introducing alcohol minimum unit pricing (MUP). Face-to-face semi-structured interviews were conducted with drinkers with alcohol-related harm (n = 20; 15 males, five females; aged 34 to 67 years old) in Scotland’s two largest cities (drinkers were participants within a larger quantitative study, through attendance for treatment for alcohol-related harms at National Health Service [NHS] centers). Median weekly consumption among participants was 130.7 units (range: 28-256.3 U.K. units). Views regarding the impact of increased alcohol prices, through MUP, were mixed. While some drinkers indicated potential reduction in intake, thus possibly reducing alcohol harms in the long term, the expected, or even desired, from a public health perspective, effects on consumption and associated harms might not be fully realized in this group. To mitigate possible unintended short-term detrimental effects of MUP on the most vulnerable, careful planning and appropriate resourcing may be required prior to implementation.
Introduction
The personal, social, and economic cost of alcohol consumption in Scotland has been estimated to be approximately £7.5 billion per year (Johnson, Ludbrook, & Jaffray, 2012), and while rates of associated health problems and mortality overall have been reducing in the past 10 years, they continue to surpass those of the rest of the United Kingdom (Beeston et al., 2013). In 2014, 18% more alcohol was sold per adult in Scotland compared with England and Wales (Robinson, Beeston, McCartney, & Craig, 2015).
Scottish governmental responses have included a range of legislative measures through the “Changing Scotland’s Relationship with Alcohol: A Framework for Action” (Scottish Government, 2009), which adopts a whole-population approach. In an attempt to mitigate the effects of low cost and easily accessible alcohol, acknowledged by the Health First evidence-based alcohol strategy (University of Stirling, Alcohol Health Alliance, British Liver Trust, 2013) to be two key drivers facilitating excessive alcohol consumption, the Alcohol etc. (Scotland) Act 2010 was implemented in October 2011 (Scottish Parliament, 2010). This legislation banned quantity discounts plus other alcohol promotions in off-sales premises (outlets licensed to sell alcohol for consumption off the premises). A subsequent reduction in off-trade wine sales was reported, but with little evidence of impact on sales of other drink types (Robinson et al., 2013). However, Nakamura et al. (2013) found that banning alcohol multi-buy promotions (primarily for beer, cider, and wine) in Scotland did not reduce alcohol purchasing in the short term, and suggested that wider regulation of price promotion and price would be required.
The Alcohol (Minimum Pricing; Scotland) Act 2012 (Scottish Parliament, 2012) will set a minimum price at which a unit of alcohol may be sold (1 U.K. unit equals 8gm/10ml ethanol), currently favored at 50 pence (£0.5: U.S.$0.8) per U.K. unit (50ppu). However, the legality of this Act in terms of international trade agreements was challenged by the trade bodies representing alcohol producers, and it was referred to the European Court of Justice (ECJ). The ECJ ruled that the Act was in breach of European Union (EU) free-trade laws, but returned the case to Scotland civil courts for a final ruling. At the time of writing, this process is ongoing, and the outcome, and therefore any implementation date for the Act, remain uncertain. An account of the Act’s development and the policy context can be found in Katikireddi, Hilton, Bonell, and Bond (2014) and Katikireddi, Bond, and Hilton (2014).
Evidence in support of increasing the price of alcohol to reduce alcohol-related morbidity and mortality derived from systematic reviews emerging from the United Kingdom, Australia, the United States, and Europe is persuasive (e.g., Booth et al., 2008; Elder et al., 2010; Jackson et al., 2010; Wagenaar, Tobler, & Komro, 2010). Scottish Minimum Unit Pricing (MUP) legislation was also critically informed by a model proposed by Sheffield University (Meng, Purshouse, Brennan, & Meier, 2010; Purshouse, Meng, Rafia, Brennan, & Meier, 2009). The Sheffield alcohol policy model version 2 was adapted to a Scottish context by incorporating Scotland-specific data on levels of alcohol consumption, the prices paid by population sub-groups for different categories of alcohol, and the preferences for off-licensed trade versus on-licensed trade purchasing (Purshouse et al., 2009).
Updated versions of the model (Meng, Hill-McManus, Brennan, & Meier, 2010, 2012) adjusting for the imposition of a 50ppu minimum price combined with a discount ban, predict figures for extra spending per annum for moderate, hazardous, and harmful drinkers at £11, £65, and £148, respectively, which equates to an additional spend per week of £0.22, £1.25, and £2.83. The model defines moderate drinkers as men/women who consume no more than 21/14 U.K. units per week, hazardous drinkers as consuming between 21/14 and 50/35 units per week, and harmful drinkers as consuming more than 50/35 units per week, respectively.
In British Columbia, Canada, where alcohol minimum pricing (not minimum unit price) has been introduced, significant health benefits have been observed, including a 32% reduction in wholly alcohol attributable deaths following a 10% increase in average minimum price for all alcoholic drinks (Zhao et al., 2013). An important assertion is that, despite popular opinion, even the heaviest drinkers reduced their consumption when minimum alcohol prices increased (Zhao et al., 2013).
The Scottish Government believes that MUP is the most effective of a range of policy options to tackle price, and help reduce alcohol consumption and related harm (Scottish Government, n.d.). MUP would set a floor price for one unit of alcohol, below which it could not be sold. For example, one 440 ml can of 5% cider contains 2.2 units, therefore, the minimum price for which it could be legally sold would be £1.10, so there would be no financial benefit in buying in bulk (as is currently the case). Certainly, current Scottish sales data (Robinson et al., 2015) would predict the greatest impact on the price of spirits (particularly vodka) and strong white cider. Those defined as moderate drinkers would be marginally affected as they consume a small amount of alcohol. Alcohol purchasing in licensed premises (e.g., pubs, restaurants) is likely to be unaffected by MUP as prices already greatly exceed the minimum proposed.
The developers of the Sheffield model acknowledge that as it is based on general population data, it cannot predict the impact on heavy drinkers. Byrnes, Shakeshaft, Petrie, and Doran (2013), using Australian survey data, reported that when faced with price increases, “high intensity” drinkers continued to binge by reducing their alcohol consumption between episodes of binging. The reduced drinking in itself may afford some health benefits, but the episodic binging represents a harmful drinking pattern. As the price of individual, cheap drinks will increase, a likely effect of MUP may be surmised from the findings of the following studies. Recent work from New Zealand (Casswell, Huckle, Wall, & Yeh, 2014) revealed that heavy drinkers paid more for alcohol overall than the general population because they consumed more, but they paid less for individual drinks as they bought disproportionate quantities of cheap, typically strong, alcohol. They tended to buy their alcohol from off-trade sources. Similar conclusions were reached in two separate studies involving drinkers harmed by their alcohol consumption in Scotland (Black, Gill, & Chick, 2011; Black et al., 2014), where participants tended to purchase cheap alcohol, with around 95% of purchases being from off-sale outlets (i.e., supermarkets and corner shops, etc.).
A common criticism of increasing the price of alcohol is that, if people with alcohol dependence can no longer afford their drink of choice, they will need to find a substitute, whether that be cheaper alcohol, counterfeit or illicit alcohol, or other substances. Alternatively, they might resort to theft. On balance, the evidence suggests that increases in alcohol pricing tend to be associated with reductions in crime (Home Office, 2011), but there is currently insufficient evidence to determine the impact of alcohol prices and purchase of other licit and illicit substances (Hunt, Rabinovich, & Baumberg, 2010).
Thus, it appears that further data relating to the drinking patterns of the heaviest drinkers in society would be valuable and informative. These drinkers rarely take part in routine population surveys documenting consumption (Livingston & Callinan, 2015), and factors, other than price, that restrict or facilitate their consumption are poorly described. As suggested by Chalmers (2014), the Sheffield alcohol policy model would ideally be built on a dataset including people’s alcohol purchases, consumption, location of purchase, and price.
Our participants comprised both dependent drinkers, and those whose health was at least harmed in some way by their drinking, as they were all recruited in hospital or clinic settings for treatment relating to their alcohol consumption. To our knowledge, this is the first report exploring the current, and self-predictions of future, purchasing behavior of a group of heavy (as we refer to them throughout the article) drinkers explicitly in relation to proposed alcohol policy.
Aims and Objectives
In light of the recent policy measures proposed by the Scottish Government, this study interviewed heavy drinkers to elicit their views regarding the cost of alcohol in Scotland, explore their awareness of increases in alcohol price, and opinions regarding implications of MUP should it be implemented, at a personal and wider level.
Method
The findings reported here are in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) 32-item checklist (Tong, Sainsbury, & Craig, 2007). This study sits within a 2-year prospective study of 639 patients attending alcohol treatment services as outpatients or admitted as hospital inpatients with an alcohol-related problem (which has resulted in physiological and/or psychosocial harm), who were interviewed about their drinking and purchasing habits approximately every 6 months over a period of 24 to 30 months.
Participants were asked at their third quantitative interview (T3), (between October 2013 and March 2014, around 18 months after recruitment), whether they would be willing to take part in an additional semi-structured face-to-face interview (see the appendix) to explore their experiences and views about recent alcohol policy and the governmental proposal to legislate a “minimum unit price” for alcohol. The interview was scheduled for a date as soon after the T3 interview as mutually convenient, mostly between 1 and 4 weeks. From those who indicated willingness, 20 participants were recruited, 10 from each of the two Scottish cities in the study (Glasgow and Edinburgh). Participants were purposively selected on the basis that they had been drinking at hazardous or harmful levels at T3, and that the average price they were paying at that time was less than 50ppu. Care was taken to ensure that they were approximately representative of the total sample by gender, social deprivation quintile, and age (see Table 1). Participants were contacted by telephone, and interview dates and times arranged. If participants failed to keep their appointment, they were contacted to confirm whether or not they were still willing to take part, if not, the interviewer then selected another potential participant from those meeting the inclusion criteria, until the target quota of 10 participants from each city was achieved.
Participant Demographics and Consumption Details at Baseline and at Time-Point Preceding Qualitative Interviews.
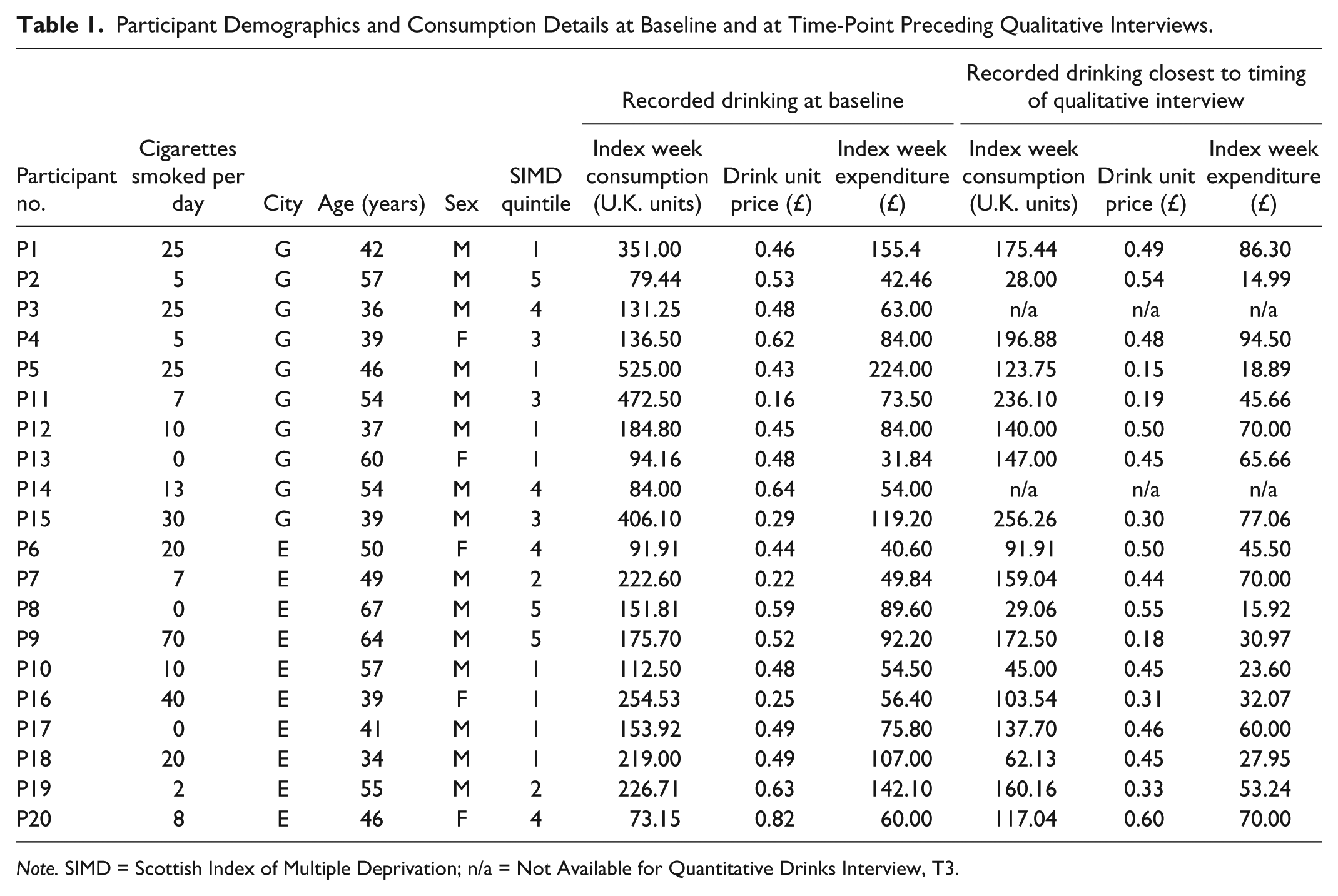
Note. SIMD = Scottish Index of Multiple Deprivation; n/a = Not Available for Quantitative Drinks Interview, T3.
Of the 28 participants contacted, three failed to respond, two declined to participate, and three did not attend the arranged interview. Of the 20 interviewed, five were not drinking at the time of the qualitative interview, but reported harmful drinking at some stage in the 6 month period prior to, or at, T3; mean age was 48.3 years, five were female. Reported median weekly consumption (past 7 days, or typical drinking week) was 130.7 units at T3 (range 28-256.26 units), and all social quintiles were represented, broadly mirroring the distribution in the larger study.
Prior to the interview, participants received by mail details of the interview topics, assurance of anonymity and confidentiality, and their right to discontinue the interview at any point, with no detrimental consequences. It was emphasized that the questions were designed to obtain their views and opinions, and that there were no right or wrong answers. Interviews took place in a health service site. Consent for being interviewed and for audio recording was taken at interview. During each interview, the interviewer gave a brief explanation of the Alcohol Minimum Pricing Act, followed by an example, using white cider, and their preferred drink (if that was different), to demonstrate how the existing price would be affected by an MUP of 50ppu.
Interviews were arranged and conducted by the researchers who had administered the earlier quantitative interviews (H.B., C.R.), to capitalize on the degree of trust already established. Interviews were recorded using an encrypted digital recorder, and were between 20 and 50 min in length. An additional member of the research team (F.O’M.) was also in attendance (once the participant had given permission) to observe the interview and make notes, subsequently transcribe the recordings, and analyze the data. Interviews were conducted between October 2013 and March 2014, between 1 and 6 weeks after T3 interview. Handwritten fieldwork notes were kept during the data collection and analysis process. Upon completion of the interview, participants were given a £10 voucher for a high street pharmacy-led health and beauty store, and reimbursed for any travel expenses.
Data Analysis
The interviews were transcribed verbatim by the first author, and during this process, initial thoughts and ideas were noted down, as an essential part of the analytic process (Riessman, 1993). Thematic analysis was conducted, as described by Braun and Clarke (2006). All the transcripts were read multiple times, to identify categories of relevance to the research aims; emerging themes and commonalities were noted. These categories were then grouped according to consistency in topic, as well as in relation to the research aims, and themes were thereby constructed, representing recurring topics. Verification of coding was confirmed by a second research team member, and all authors had iterative discussions regarding the construction of themes and their interpretation. The constant comparative method was used to help identify reasons for patterns and contradictions in the data.
Ethical approval was provided by National Health Service (NHS) Lothian Research Ethics Committee and was reviewed by the respective Caldicott Guardians.
Results
When asked about proposed alcohol policy, specifically MUP, participants gave wide ranging responses, sometimes relating it to their own personal experiences, and at other times projecting, referring to other drinkers, known or unknown to them, or the general public.
Contextually, public houses and bars played a minimal role in participants’ lives, with only one or two reporting drinking in pubs, and then only occasionally, or when friends took them out. Pubs were generally considered to be far too expensive for alcoholic and non-alcoholic drinks alike, the latter reducing any incentive to supplement or replace alcoholic beverages, and actually encouraging individuals to drink at home. Other comments indicated that pubs were where social drinking took place, which was no longer possible for these individuals; that they were not safe places because people could become violent and aggressive; and that drinking soft drinks in a pub made you feel silly as pubs were for drinking alcohol.
Drinkers’ Anticipated Personal Strategies to Cope With an Increase in Drink Prices Through MUP Implementation
When asked what would happen if the price of their preferred drinks were to increase, various tactical ways to manage were proffered. One participant reported she would switch from lager to spirits, as they were higher strength and she would get more units for her money, and could make her drink last longer by adding mixers. Alternatively switching to cheaper alcohol, such as white cider or supermarket own brand, was mentioned, “. . . it’s only when I’m down to my last pennies, and what can I buy for this, and my option is, I can get cheap cider for it” (P4, female), and “I would probably change what I was drinking . . . cider, or something cheap and nasty . . . [brand of white cider]” (P18, male); or reducing consumption, in some cases dramatically, “Phhhh . . . there’s no way I could address it . . . I would actually just need to cut right back or stop” (P5, male) and “. . . I would really struggle to actually maintain the drinking level . . . I would have to dramatically reduce my alcohol intake . . . well, I’d have to try” (P15, male).
Some would be prepared to cut back on drink, to keep food intake constant, “I have to buy all the food, I haven’t got any choice, it’s the drinking that has to be cut back on” (P9, male), whereas others would cut back on food, “I’d still be able to buy it [alcohol], I’d just do without food” (P16, female), or not pay bills, borrow money, and get into debt or increase debt to maintain alcohol consumption, “I’d probably borrow money off my family members, especially my oldest daughter . . . that would be my only way round about it” (P13, female), and “. . . I would just do without heating and I’d have to rely on my family more . . . or friends” (P17, male).
Other tactics included shopping elsewhere and seeking out offers. One candidly stated he did not know how he would procure his alcohol, but “I think it will be drastic, what I would go to, to get what I need” (P1, male).
Those respondents who were either not drinking at the time of interview, or had cut down, spoke of “others,” saying perhaps “they” might resort to stealing alcohol, or switch drink type,
. . . if they’re that advanced . . . they’ll go and get something else. I don’t know what I think about it, but I don’t think it would stop. People will just go onto something cheaper and nastier, if they really wanted. (P3, male)
Unsurprisingly, the three participants who stated that they were not short of money were less concerned about any potential impact of MUP, “. . . it would be a while before I did that [change brands], because I’ve got enough money to pay for it” (P2, male);
. . . we have a bottle of wine amongst 3, every day . . . Pinot noir, it’s good quality wine. So we’re not buying the £2 or £3 bottle of wine. Money is not the issue with us. (P8, male);
and “that doesn’t bother me at all, the price of alcohol. I was buying it anyway. Eh, I don’t look at price” (P14, male).
Some participants perceived adverse health consequences of stopping or suddenly reducing alcohol intake in response to increased prices, in particular, a fear of seizures by those who had themselves experienced them, as tolerance/dependence can vary widely, making seizure prediction difficult, “. . . [it] could harm people, especially if you’re a right alcoholic, it could destroy them, it could kill them—just totally cutting down” (P16, female).
One participant, who had already reduced her alcohol consumption by approximately two thirds owing to financial constraints following a bereavement, said she would have to try to cut down further if prices continued to rise, but this caused her concern:
If it was to go up quite suddenly, I think my intake would be reduced again, because of the cost . . . which really worries me, because at the moment, I’m comfortable in my own wee zone, because I’ve turned into a recluse, kind of, since my [bereavements] . . . it’s going to send me into a state of depression I think, because I’m out of my comfort zone. (P6, female)
A number of participants stated that if MUP were introduced, they would just have to stop drinking, but could not expand on how they might do that, other than one who said she would seek medical treatment, “I would just get myself in somewhere, like here [detox centre] . . . there would be no way around it for me, I would just have to ride it out, or get help” (P4, female).
Awareness of MUP and Perceptions of Its Potential Wider Impact
All participants had been informed about the proposed introduction of an MUP at first, and subsequent, interviews. Some were aware that the legislation was currently being challenged, however, several claimed ignorance or did not know any details. Many expressed resistance to MUP, both from a personal perspective, as well as on behalf of others. One view was that people already paid enough tax, and claims that drinkers and smokers were “clogging up the health service” should be counteracted by saying that the government gained a lot in tax from them, and that MUP ultimately would hurt people “at the bottom.” Another said,
I don’t believe MUP will work . . . to me, it’s one step away from prohibition. Alcohol is still going to be available, and it’s just going to be a lot more expensive, and all that will happen is that people that can afford it anyway, they’ll pay it . . . whether or not they’ve got an alcohol problem, and people that can’t afford it, and who do have an alcohol problem . . . it’s going to lead to a burgeoning of a black market, which already exists with vodka, and whisky. (P5, male)
A participant said that while he agreed with MUP in principle, because he was drinking heavily again, he would not welcome it in practice,
My opinion is, if they [drink prices] can put someone like me into this state, and they can achieve it so easily, then it’s a disgrace . . . I would agree with that [MUP], unfortunately at the moment I wouldn’t. (P1, male)
Another felt that “. . . if it’s [MUP] going to help people and alcoholics, good, but if it’s not going to make any difference, I don’t see why they don’t just leave it alone” (P7, male).
With regard to white cider specifically, there was a suggestion that MUP could be beneficial:
. . . I reckon if they kept 50 pence a unit, I think that would be better, because a lot of people would stop drinking [brand of white] cider, because I think that’s a big, big problem . . . But £4 for 22 units—that’s how much a bottle of [brand] is . . . so if they put it at 50 pence a unit, I think that would work out better. (P12, male)
It was also suggested that some people might even be persuaded to change from white cider to a “nicer drink” or “trade up” when they compared the prices post-MUP. One respondent calculated that his current 3-liter bottle of white cider would virtually triple in price at 50ppu, which he would no longer be able to afford,
A bottle of [brand of white cider] is going to be almost £10, that’s 3 liters. Currently I could get that or, the cheapest is £3.79, I think, so you’re looking at almost tripling the price. And there’s just no way I could afford that. (P5, male)
A participant who was currently not drinking thought that the effect of MUP on cheap ciders would “probably be a good thing” but went on to say that, in his opinion,
if somebody wants to drink, they’ll drink. They won’t be happy about the extra price, but if they’re an alcoholic or whatever, they will find a way to pay the money . . . (P7, male)
One participant, for whom money was not an issue, was positive regarding the proposition of MUP and felt that 50ppu was too cheap, “I would think it should be 60 to 65 pence. That’s my view” (P8, male). Another, similarly without financial problems, thought MUP would serve as a wakeup call, and that any disincentive would be positive,
I suppose it would make me realize just how much money I was wasting on it, when I could use the money for other things. It would be a big [sigh] reason to drink less, or stop drinking. It might not be enough to completely stop me, but it would be a very big consideration. (P2, male)
Several respondents indicated that they did not feel they would be personally affected, as they were already paying more than 50ppu. A retailer’s point of view was provided by a participant whose employment had involved the sale of alcohol. He was receptive to the prospect of MUP, as a means of removing the financial advantage perceived to be currently enjoyed by bulk-buying supermarkets:
. . . if I was still in business, I would have loved minimum pricing to come in, if I was selling alcohol . . . levelled the playing field. They couldn’t sell stuff cheaper than a certain amount, and I could probably sell for that price as well. (P14, male)
One participant suggested that MUP could reduce drinking by younger people, who tend to drink the cheapest drinks, particularly white cider and vodka, and that a dramatic price rise might make them think about spending their money on other items or activities:
. . . it is relatively cheap to go and get blasted for the weekend, you know, but for somebody to go to the cinema, it’s a tenner . . . or to go swimming, they’d have the bus fare there, the bus fare back, that’s £1.40 . . . plus the price of £3.50 to get into the swimming pool, that’s a fiver. You know, get somebody else to give us a pound, that’s two big bottles of cider! Way hay! . . . it’s too accessible, you know, and everything else is too expensive. (P20, female)
However, she did not think that MUP would influence those who were addicted, as “they’ll obtain alcohol wherever and however” (P20), which included driving to England to obtain cheaper alcohol, buying illicit alcohol, and home brewing. Others similarly predicted the likely failure of MUP,
I don’t think there’s anything else the politicians can do. If they introduce minimum pricing, then, they’ll just, they’ll still drink the alcohol, em, or they’ll be . . . pooling their money to get the stronger stuff, if that’s what they want . . . they’ll still get the alcohol . . . regardless of the price. (P14, male)
None of our participants indicated that they would resort to drinking illicit alcohol, following the proposed introduction of MUP; indeed, some stated they were very fearful of the damage such drink could potentially inflict and would not touch it, “It might not be ethanol, it might be methanol that’s in it, and you wake up blind or something. I just wouldn’t touch that” (P5, male). Only one participant mentioned potentially switching from alcohol to drugs, saying he would “just buy a bit of dope!” (P3, male).
Discussion
MUP is a whole-population intervention, and the participants in our study are members of a small but noteworthy section of the population, many of whom would be disproportionately affected by an increase in alcohol prices, such as through MUP, owing to the large volume and cheaper type of alcohol they purchased. Our findings show a range of views and awareness regarding MUP, and a varied perception of its hypothesized impact consistent with the demographic spread across Scottish Index of Multiple Deprivation (SIMD) quintiles, age, and levels of consumption. Participants who were already abstaining, and those who were considering abstention or reducing their consumption to “safe” levels, were more receptive to MUP than those who were not. Two participants reported that they would have to reduce their alcohol purchasing and consumption if MUP were introduced, owing to financial constraints, thus supporting the purpose of MUP.
Several respondents struggled to understand the concept of MUP; they still talked of trading down, using white cider as a fall back, or making more of an effort to track down special offers (which would no longer exist). They had not understood that they would be paying a minimum of 50 pence for each unit of alcohol (8g ethanol) contained in a drink, with no option to benefit financially from, for example, bulk buying or purchasing an alternative beverage type. Our quantitative data show that the mean unit price paid for beer was slightly above 50ppu (Gill et al., 2015), but, we propose, high alcohol consumption levels of beer drinkers are supported through the availability of cheaper drinks such as cider (Black et al., 2014).
It is important that discussion of the potential impact of MUP does not disregard the addictive nature of alcohol and its impact on purchasing. Many participants were generally not able to plan ahead, let alone take account of legislation that might not be implemented for years, if at all. To them, MUP was a vague and obscure concept, their attitude was that they would deal with any issues if, and when, it was in place. This absence of personal anticipatory preparation for MUP implementation could have implications for health services, such as increased emergency hospital admissions and demands on detox services.
Reducing alcohol harm is a complex problem, requiring complex solutions. From their global systematic review and narrative synthesis of 42 studies that focused on alcohol policy interventions, Diepeveen, Ling, Suhrcke, Roland, and Marteau (2013) concluded that public acceptability of government interventions to change behavior is greatest for the least intrusive interventions, which are often the least effective, and for interventions targeting the behavior of others, rather than the respondents themselves. They recommend further research to assess how the presentation of the problem and the benefits of the intervention might increase acceptability for those interventions that are more effective but less acceptable. Results from recent Scottish and English research (Alcohol Policy Interventions in Scotland and England [APISE] study) showed that harmful and hazardous drinkers were less likely to support alcohol policies than moderate drinkers, but that the majority of respondents believed that the government has a responsibility and should be doing more to tackle harms caused by alcohol. Opinion on how they should be doing this, and who they should be targeting, however, was not clear (Li, 2014).
Lonsdale, Hardcastle, and Hagger (2012) reported skepticism regarding effectiveness of MUP as a means to reduce alcohol consumption from a sample of 218 members of different community groups in England, of whom 10 were hazardous drinkers, but none was a dependent drinker. In our study, many participants did not feel that any proposed alcohol policy was going to help them, but that the introduction of, for example, MUP, might reduce the likelihood of younger people developing the same drinking patterns and harms that they had.
Instead of perpetuating the perception that alcohol misuse is largely an individual problem best avoided and managed through education, counseling, and medical treatment, Groves (2010), among others, has suggested that for the United Kingdom, the health and societal costs of alcohol misuse are best prevented through legislation on pricing and marketing. In this vein, portraying alcohol policy as a broad, multi-sectoral, public health issue that requires a whole-population approach has been crucial to policy development in Scotland (Katikireddi, Bond, & Hilton, 2014). However, certain individuals and/or groups of people, such as those with alcohol-related harm interviewed in this study, may be affected more than others, perhaps by some unintended consequences. If MUP were introduced, the population effect (Meng, Hill-McManus, Brennan, & Meier, 2012) might be delayed. The lower-risk drinkers in Scotland could either over time reduce their consumption, decide to pay a bit more to maintain it, or even stockpile some cheaper pre-MUP alcohol. However, for the people we interviewed, who have a high frequency of purchasing and high expenditure owing to the high volumes purchased, the impact of MUP would be immediate, particularly so for white cider and cheap vodka drinkers.
Certainly, evidence shows that increasing the price of alcohol reduces harms of various types, and indicates that dependent drinkers are no exception to the rule that alcohol consumers respond to changes in alcohol prices (Babor et al., 2010). While a reduction in hospital admissions over time would be one anticipated effect of MUP, in the shorter term, the impact may be an increase and, if imposed during the winter months, an exacerbation of the general season-associated increase due to respiratory conditions and influenza (Scottish Government, 2015). The timing of its introduction should be carefully considered, in addition to the potential impact on quality of life, as many of our participants mentioned the competing financial demands of purchasing alcohol, buying food, and paying household bills.
Consequential changes in demands on treatment facilities also merit consideration. A recent survey of specialist alcohol treatment services in Scotland identified ongoing issues relating to service gaps, service planning, staffing, demand, and missed appointments (cited in Beeston et al., 2014, p. 16). Stockwell, Williams, and Pauly (2012) found that in British Columbia, when heavy drinkers were asked what they did if money was short, many said they applied for treatment. Sudden alcohol withdrawal is dangerous for dependent drinkers, in the most serious cases causing seizures. At the last estimate for Scotland, only one in four alcohol dependent drinkers was accessing alcohol services (Beeston et al., 2014), and Wallhed-Finn, Bakshi, and Andreasson (2014) reported that a minority of those with alcohol dependence seek and undergo treatment. All participants in our study have received treatment relating to their drinking at least once (their recruitment site), but there are likely many more (whose numbers we do not know) who have not engaged with services, or received support. If MUP is introduced, trading down to cheaper alcohol will no longer be an option, impacting on those already using services, but also potentially on an unknown number of people with alcohol dependence who are not.
Any unintended increases in the numbers contacting health and/or social care would likely be short term, following the implementation of an MUP, and could well be counterbalanced by falls in service use over a longer time period, due to reduced consumption within a much larger section of the population. Within the heavy drinking population, arguably there might be a greater demand for treatment services (e.g., detox, counseling, etc.) but a subsequent fall in emergency admissions due to accidents, bleeds, or myocardial infarction, for example, because of medically significant reductions in consumption.
MUP is not a tax and any increased revenue from an increased unit in price is proposed to be returned to the retailer, who will also be at liberty to increase the price of any drink, not just those that are currently sold under the 50ppu (Sheffield Alcohol Research Group, n.d.). One potential measure would be to annex part of the retailers’ anticipated profits and ring-fence for treatment services, in the form of a hypothecated tax, which would likely prove to be highly controversial (see, for example, Keable-Elliott, 2014).
One criticism of MUP is the potential for an increase in sales of illicit alcohol (Hilton, Wood, Patterson, & Katikireddi, 2014; Katikireddi, Bond, & Hilton, 2014). Several participants referred to its availability, while many stated they would actively avoid illicit alcohol due to safety concerns. Whether they would reconsider this view when finances are extremely stretched—with a choice between more expensive (legal) drinks and much cheaper (illegal) alcohol of unknown provenance and potential safety hazards—is not known.
Strengths and Limitations
Our study has a number of strengths. To our knowledge, this is the first published study that explores the perceptions and behaviors of heavy drinkers with regard to alcohol policy in Scotland, both extant and proposed, and provides insight into how members of a certain minority group felt they might be impacted by a population-level policy. Opinions and attitudes do not, of course, necessarily predict behavior, and are likely colored by current drinking status. Data were collected at an interesting time in the policy debate and complement existing research, which has, thus far, primarily focused on stakeholders’ perspectives, such as those in the public and voluntary sector, as well as industry representatives (Carrell, 2014; Katikireddi, Bond, & Hilton, 2014; Katikireddi, Hilton, et al., 2014; Meng, Hill-McManus, Brennan, & Meier, 2012; Scottish Government, 2012).
A key limitation was the attrition rate of the study, which meant that at time of interview, the number of potential recruits available to sample had reduced from 639 to 165. In addition, as more than 100 of the attritions were attributed to death, we may not have been able to recruit those who were drinking the most (although we have presented their consumption figures at baseline, see Table 1). Certainly, evidence shows that increasing the price of alcohol reduces harms of various types, and indicates that dependent drinkers are no exception to the rule that alcohol consumers respond to changes in alcohol prices (Babor et al., 2010). While a reduction in hospital admissions over time would be one anticipated effect of MUP, in the shorter term, the impact may be an increase, and, if imposed during the winter months, an exacerbation of the general season-associated increase due to respiratory conditions and influenza (Scottish Government, 2015). The timing of its introduction should be carefully considered. Some participants were not drinking at the time of the interview, and so they were describing actions in the past, or hypothesizing with regard to how they might purchase alcohol, now, or in the future, so we have no way of knowing whether or how their purchasing habits would be affected. However, on average, from our data, each participant would be required to increase expenditure by 21% to obtain the equivalent number of units should MUP at 50ppu be introduced. Put another way, the potential reduction in unit consumption induced by MUP if participants did, or could, not increase their expenditure, would be 24% (total sample), but for the sub-group drinking exclusively white cider, their consumption would need to drop by 66% (Gill et al., 2015).
Conclusion
Our findings provide important and relevant insights into the views and drinking practices of the heaviest consumers of alcohol. MUP has the potential to reduce alcohol-related harms on multiple levels, impacting on drinkers across the spectrum. The unique pattern of drinking described by this group underscores the need for a more accurate modeling, such as with the Sheffield model, of the potential ramifications of MUP. There are challenges associated with securing relevant informing data, and population surveys have significant shortcomings in this regard. MUP is likely to impact positively on a large proportion of drinkers, including some heavy drinkers, but it may have some short-term implications for a small group of dependent drinkers, some of whom may be unable to cut down on their alcohol consumption, and others who would need to suddenly cut down drastically. Both of these scenarios may have unintended detrimental consequences, which should be planned for and resourced appropriately. From our small study, we suggest that preventive and anticipatory approaches, targeted at those whose consumption causes them harm, could go a long way to making life better for all those who suffer from alcohol-related harm. In addition, further qualitative investigation regarding barriers and facilitators to reducing alcohol consumption among heavy drinkers, in response to increased alcohol prices, would be welcome.
Footnotes
Appendix
Acknowledgements
The authors would like to thank the interviewees for participating in this research, and the clinicians who facilitated the study. They would also like to thank Lucie Michalova and Robert Rush for their assistance and support, and the study steering group.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.C. reports personal fees from H. Lundbeck A/S and from Drinkaware during the conduct of the study.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was supported financially by the Chief Scientist Office, Scotland (CZH/4/645); Alcohol Research UK (R2011/01); National Health Service (NHS) Health Scotland; NHS Lothian Foundation Trust; and in kind by the Scottish Mental Health Research Network.