
Abstract
Age-related declines in postural control and physical fitness are strong risk factors for falls in older adults. Balance efficacy has been utilized to identify poor postural control, reduced physical function, and fall risk. However, it is not clear as to whether balance efficacy is truly a better predictor of functional fitness outcomes or postural control. Distinguishing these associations is an important step in the future derivation of physiotherapeutic programming to remediate acute and chronic decline. Therefore, the purpose of this cross-sectional study was to partition which measures are more associated with balance efficacy, fitness, or postural control. One hundred eleven community-dwelling older adults participated and were asked to complete the Balance Efficacy Scale (BES), a functional fitness measure (the Senior Fitness Test [SFT]), and a measure of postural control (the Sensory Organization Test [SOT]).We found that the SFT was more significantly associated with balance efficacy (R2 = .37) than the SOT (R2 = .08) in older adults. Overall, aerobic endurance, functional mobility in the SFT, and the vestibular score on the SOT were significantly associated with balance efficacy.
We concluded that clinicians utilizing the BES as a preliminary screen should recommend physiotherapy follow-up activities that build endurance (walking), lower extremity functional mobility (sit-to-stand), and vestibular function (head movement while walking). Understanding the links between a preliminary screening tool and the physiological needs of the patient will allow for targeted activities to be prescribed.
Introduction
Falls are one of the biggest problems for adults above 65 years of age, causing accidental death and secondary serious injuries (Bishop, Patterson, Romero, & Light, 2010). Thirty percent of community-dwelling older adults (65+) and 50% of older adults above 80 years old fall annually (Bishop et al., 2010). The negative outcomes associated with falls include psychological and physical limitations, which further exacerbate fear of falling. These compounding negative consequences can lead to social isolation, depression, and decreased quality of life (Bishop et al., 2010; Portegijs et al., 2012).
Balance efficacy is defined as a person’s perceived self-confidence (i.e., self-efficacy) regarding the ability to avoid falls while performing an identified activity (Bishop et al., 2010; Legters, Whitney, Porter, & Buczek, 2005). Thirty-five percent of community-dwelling seniors report activity avoidance due to low-balance efficacy (Fletcher, Guthrie, Berg, & Hirdes, 2010). Low-balance efficacy related to falls has been found to be a sensitive predictor of falls (Carpenter, Adkin, Brawley, & Frank, 2006). Researchers have been exploring the relationship between balance efficacy and other risk factors to better understand falls in older adults (Arnold & Faulkner, 2009; Bishop et al., 2010; Brown, Polych, & Doan, 2006; Liu-Ambrose et al., 2006; Myers et al., 1996).
Postural control and physical fitness play important roles in determining older adults’ fall risk (Liu-Ambrose et al., 2006; Woollacott & Shumway-Cook, 2002). A decline in postural control, which can result from a decline of a sensory system (e.g., diminished visual, vestibular, or somatosensory function) and/or diminished functional fitness (e.g., decreased muscle strength and size, mobility, and flexibility) due to aging, has been documented to be strong predictors of falling in older adults (Hess & Woollacott, 2005; Konopack et al., 2008). The Senior Fitness Test (SFT) is a valid and reliable measure of fitness in older adults (Rikli & Jones, 2013). It includes measurements of strength (i.e., chair stand, arm curl), flexibility (i.e., chair sit-and-reach, shoulder stretch), endurance (i.e., 6-min walk, 2-min step test), and functional mobility (i.e., 8-foot up-and-go). Moreover, the Sensory Organization Test (SOT) has been regarded as an important measurement tool used to examine and understand postural control through the integration of visual, somatosensory, and vestibular components (Jacobson, Newman, & Kartush, 1993).
Previous studies have found that balance efficacy is related to functional fitness (Klima, Newton, Keshner, & Davey, 2012; Woollacott & Shumway-Cook, 2002) and postural control (Arnold & Faulkner, 2009). For example, Klima et al. (2012) found that balance efficacy is significantly correlated with balance ability and functional mobility in community-dwelling older men. Other researchers have found aerobic endurance is strongly related to balance efficacy in older adults (Julius, Brach, Wert, & VanSwearingen, 2012). Moreover, it has been found that balance efficacy is an independent predictor of balance performance in challenging sensory conditions (Arnold & Faulkner, 2009; Liu-Ambrose et al., 2006). However, according to Lane et al. (2014), balance performance scores from the SOT did not show significant differences between high fear of falling and low fear of falling groups in older adults who were diagnosed with vascular intermittent claudication.
In addition, increased anxiety levels toward postural control showed a decrease of the center of pressure sway variability in combination with an increase in sway frequency (Brown et al., 2006). Furthermore, Bishop et al. (2010) argued that balance efficacy scores are not related to lower leg muscle strength (i.e., quadriceps, dorsi flexors, hip abductors) or functional mobility.
These previous efforts to study the relationship between balance efficacy and postural control, and balance efficacy and physical fitness have provided mixed findings (Arnold & Faulkner, 2009; Bishop et al., 2010; Brown et al., 2006; Liu-Ambrose et al., 2006; Myers et al., 1996). In addition, studies investigating which is more related to balance efficacy, postural control or functional fitness, are lacking. Therefore, the purpose of this study was to partition which measure is more associated with balance efficacy, fitness, or postural control. We hypothesized the following:
Method
Participants
One hundred eleven community-dwelling older adults (female = 71, male = 40) between 61 and 91 years old (75.1 ± 6.1) participated in the present study. G Power (Faul, Erdfelder, Buchner, & Lang, 2009) was used to calculate the sample size required for multiple regression analyses. If up to six variables were modeled at an effect size = 0.35 (large) at an alpha level of .05 and power of 0.80, a minimum of 68 participants are required. The participants were recruited from senior centers in the surrounding community via group presentations about falls and fall risk given by the senior author. Interested individuals contacted the researchers after these presentations. All participants submitted physician approval forms for their eligibility to participate in the present study and provided written informed consent. Participants were excluded if they had a previous history of peripheral or vestibular abnormalities, a history of two or more falls in the previous 6 months, or if they were not able to walk without assistance. This study was approved by the Institutional Review Board at the University of Texas at Arlington.
Assessments
All participants completed a self-report measure of balance efficacy (Balance Efficacy Scale [BES]) as well as measures of fitness (SFT) and postural control (SOT) during a single visit to the lab. The order of the measures was random, and each of the measures is described in more detail in the following.
The BES is a self-report measurement of balance efficacy examining how individuals feel about performing daily activities with or without support (e.g., handrail). Individuals report how confident they are in performing 18 items on the test (e.g., getting out of bed, walking on uneven ground, standing on one leg, reaching for an object, etc.), from 0% (not confident at all) to 100% (absolutely confident). Average scores below 50% represent low-balance efficacy (O’Sullivan, Schmitz, & Fulk, 2007).
The SFT is a well-validated (r = .77-.83) and reliable (R = .81-.96) functional fitness test, which identifies functional performance across four domains (i.e., muscular strength, flexibility, functional mobility, and aerobic endurance) in older adults (Konopack et al., 2008). It consists of eight measures of functional fitness: chair stands, arm curls, shoulder stretch, chair sit and reach, 8-foot up-and-go, 2-min step test, 6-min walk, and grip strength (Rikli & Jones, 2013). A description of each SFT variables is shown in Table 1.
Description of Variables in SFT.
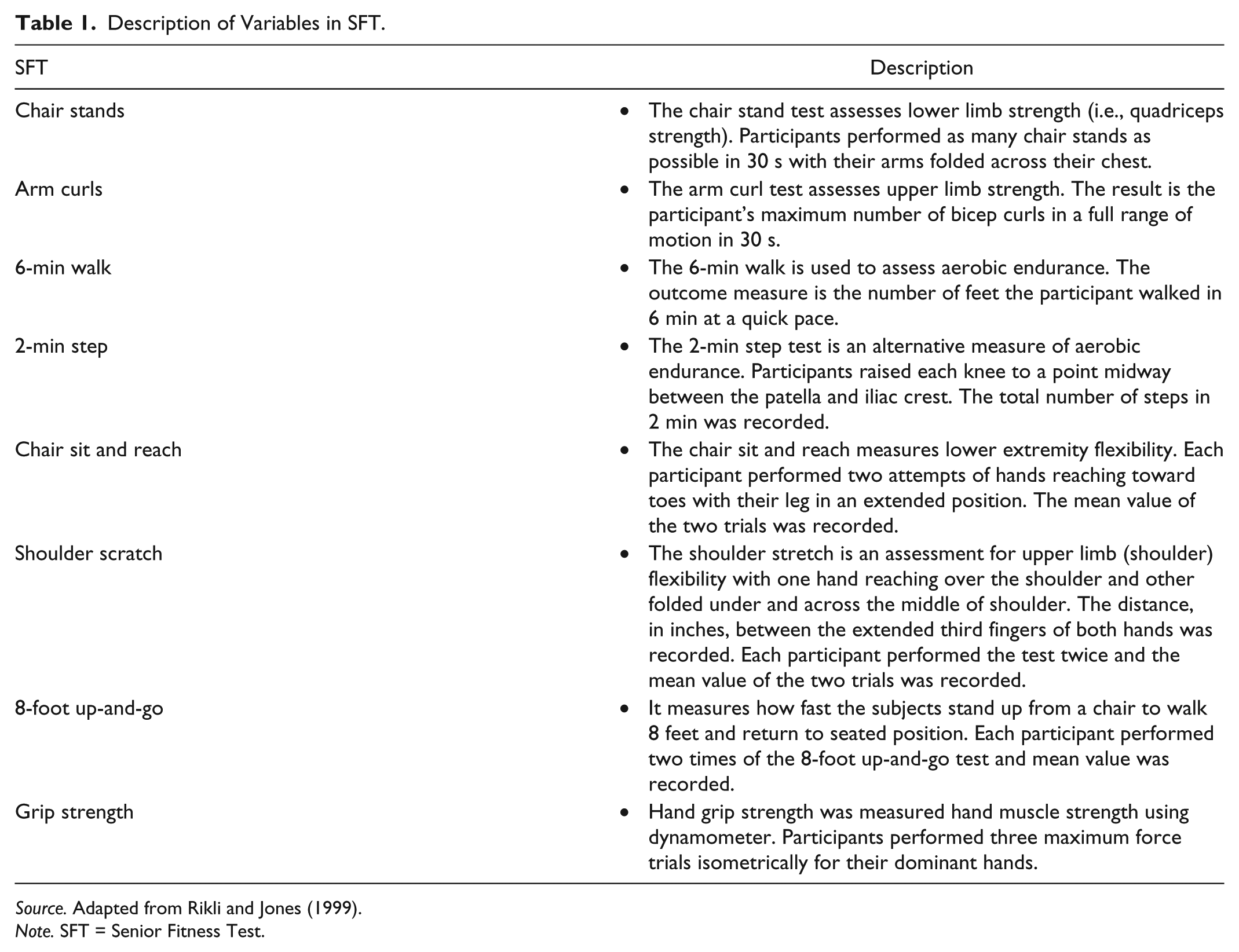
Source. Adapted from Rikli and Jones (1999).
Note. SFT = Senior Fitness Test.
The SOT of the NeuroCom® Equitest (NeuroCom International, Clackamas, Oregon) was used to assess postural control. To accomplish this, inaccurate information was delivered to the eyes, feet, and joints through sway referencing of the visual surround and support surface (Jacobson et al., 1993). The equilibrium score quantifies the Center of Gravity (COG) sway in real time (i.e., 20 s) of six conditions: (a) eyes open, surround, and platform stable; (b) eyes closed, surround, and platform stable; (c) eyes open, sway-referenced surround; (d) eyes open, sway-referenced platform; (e) eyes closed, sway-referenced platform; (f) eyes open, sway-referenced surround, and platform (Jacobson et al., 1993). Small COG anterior–posterior sway indicates 100% of equilibrium score, and sway that exceeds limit of stability and loss of balance indicates an equilibrium score of 0% (Jacobson et al., 1993). The somatosensory ratio, visual ratio, and vestibular ratio in the sensory organization analysis quantifies the ability to use input from the somatosensory, visual, and vestibular systems to maintain balance (Jacobson et al., 1993). The six conditions (Figure 1) were used to calculate sensory analysis ratios for visual, proprioceptive, and vestibular systems input (Jacobson et al., 1993). The somatosensory domain score was calculated that equilibrium test in Condition 2 score was divided by Condition 1, visual domain score was calculated that the score of Condition 4 was divided by Condition 1, and the vestibular domain score was calculated that Condition 5 score was divided by Condition 1 score. Participants stood still on the platform while wearing a safety harness for each 20-s trial (three trials per condition). Average values of the three trials for the six conditions were used for the calculation for the three components of SOT scores.

Six conditions of Sensory Organization Test (SOT): (a) eyes open, surround, and platform stable; (b) eyes closed, surround, and platform stable; (c) eyes open, sway-referenced surround; (d) eyes open, sway-referenced platform; (e) eyes closed, sway-referenced platform; (f) eyes open, sway-referenced surround, and platform.
Outcome Variables
The balance efficacy score was used as the dependent outcome and SFT (i.e., chair stands, arm curls, shoulder stretch, chair sit and reach, 8-foot up-and-go, 2-min step test, 6-min walk, grip strength) and SOT (i.e., equilibrium score in somatosensory, visual, and vestibular domains) were used for independent variables.
Statistical Analysis
A multiple regression analyses were used to determine the association between the BES and functional fitness test, and BES and SOT. The linear equation included the following dependent variables: BES and independent variable: functional fitness test (SFT) and SOT Pearson coefficient correlation was also used for each variable of the SFT and SOT with the BES. All analyses were performed with SPSS 22 (IBM, Chicago, Illinois). Alpha was set to .05 for all analyses.
Results
Of the 111 older adults, a total of three participants were not able to finish the 6-min walk or 2-min step test due to fatigue. The assumptions of linearity, independence of errors (SFT = 2.24, SOT = 2.14) by the Durbin–Watson statistic, homoscedasticity, multicollinearity, and normality of residuals were not violated. A retrospective power analysis was performed using G*Power, which estimated the effect size to be 0.35. Statistical power was estimated at d = 0.99, when calculating for α = .05, N = 111, and 11 predictors. Eleven variables, eight in SFT and three in SOT, were used to explore the association with balance efficacy score. Means, standard deviations, and correlation coefficients of BES, SFT, and SOT are summarized in Table 2.
Mean (SD) and Correlation Coefficient of Variables.
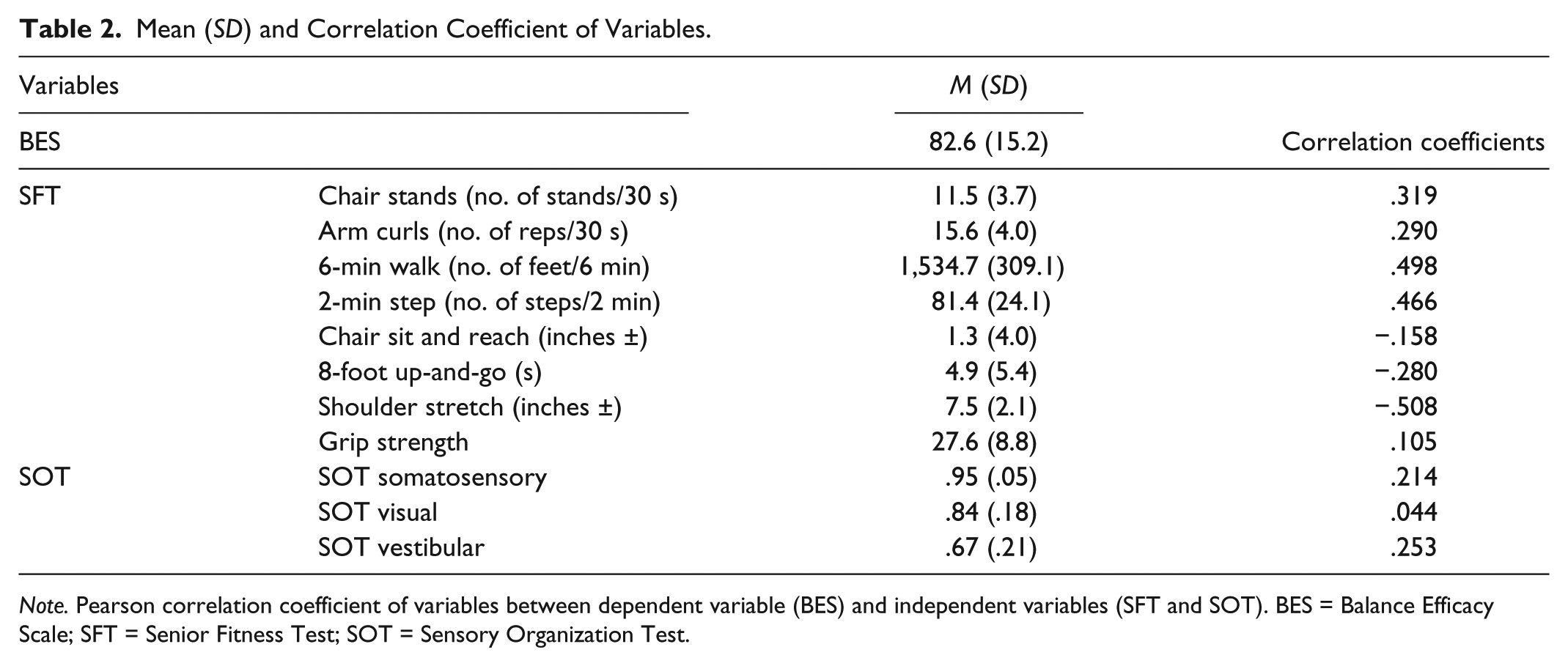
Note. Pearson correlation coefficient of variables between dependent variable (BES) and independent variables (SFT and SOT). BES = Balance Efficacy Scale; SFT = Senior Fitness Test; SOT = Sensory Organization Test.
We found that the SFT was significantly associated with the BES, R = .61, R2 = .37, F(8, 102) = 7.58, p < .001, 95% confidence intervals (CI) = [41.42, 89.12] (see Table 3, for specific variables). Moreover, the composite SOT was significantly associated with BES, R = .28, R2 = .08, F(3, 107) = 3.08, p = .031, 95% CI = [−24.64, 90.67].
ANOVA of the Multiple Regression Analysis With Predictors of Balance Efficacy From the SFT and the SOT.

Note. Dependent variable: Balance Efficacy Scale [BES]; SFT = Senior Fitness Test; SOT = Sensory Organization Test.
p < .05.
Regression coefficients and standard errors can be found in Table 4. Based on standard β coefficients (Table 4), aerobic endurance (i.e., 2-min step [β = .228, p = .023] and 6-min walk [β = .246, p = .014]) scores in the SFT showed the strongest association with the BES. The functional mobility assessment (i.e., 8-foot up-and-go [β = −.214, p = .045]) in the SFT was also significantly associated with balance efficacy. In addition, the vestibular score from the SOT (β = .213, p = .040) showed the highest association with BES. All other variables were not significantly associated with balance efficacy. The results indicate that aerobic endurance and functional mobility and vestibular function are associated with the balance efficacy screen.
Multiple Regression Analysis Predicting Balance Efficacy From the SFT Variables and the SOT Variables.
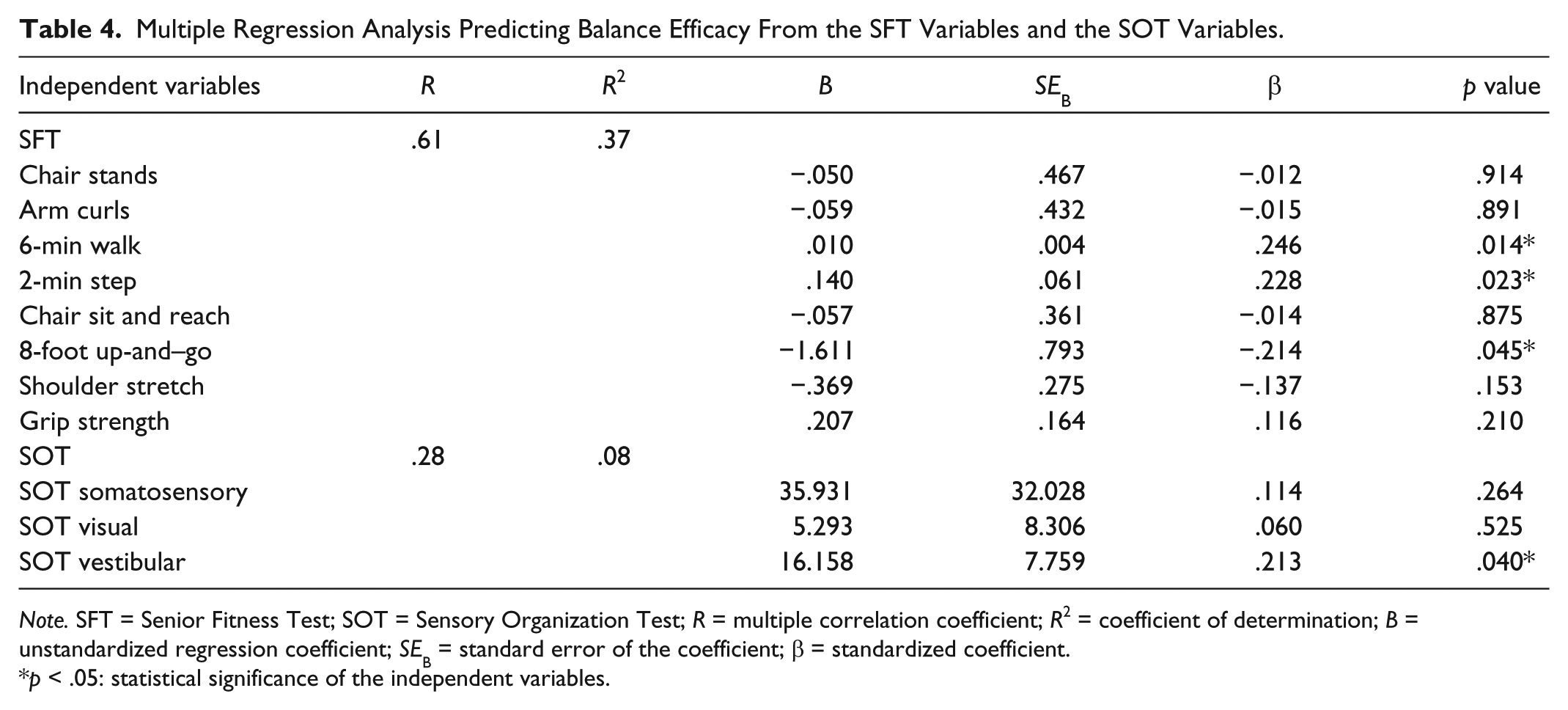
Note. SFT = Senior Fitness Test; SOT = Sensory Organization Test; R = multiple correlation coefficient; R2 = coefficient of determination; B = unstandardized regression coefficient; SEB = standard error of the coefficient; β = standardized coefficient.
p < .05: statistical significance of the independent variables.
Discussion
The purposes of this study were to explore which, postural control or physical fitness, is more associated with balance efficacy, and which measurement is the most associated with balance efficacy in community-dwelling older adults. The present study did not support our first hypothesis showing that physical fitness, as measured by the SFT, is more associated with balance efficacy than postural control, as measured by the SOT. However, the results were in accord with our second hypothesis that aerobic endurance in SFT and SOT score of vestibular system would be significantly associated with balance efficacy.
The present study showed that scores on the SFT are more associated with balance efficacy than postural control in older adults. The results are similar to previous findings that fear of falling is independently associated with activity level, which is related to physical fitness (Bruce, Devine, & Prince, 2002). Moreover, Portegijs et al. (2012) and Weerdesteyn, de Niet, Van Duijnhoven, Cho, and Geurts (2008) reported an interaction between balance efficacy, physical fitness, and balance. Previous falls lead to low-balance confidence (i.e., fear of falling). The low-balance confidence leads to self-imposed restriction in activity, which reduces fitness. The decreased physical function also causes future falls due to balance deterioration, functional decline, anxiety, and decreases in social contacts (Fletcher et al., 2010); however, the time it takes for this to occur is likely variable based on the participants’ initial level of fitness. Similar to the previous studies, the present study supports the finding that physical fitness in elderly adults may be a stronger indicator of balance efficacy than postural control. In addition, the higher association between balance efficacy and physical fitness than postural control advances the understanding about the interacting relationship between the three factors (Portegijs et al., 2012). Rather than sensory strategy using visual, somatosensory, and vestibular system in balance control, the present study determined that physical fitness is more associated with balance efficacy.
The present study found that aerobic endurance and functional mobility are significantly associated with balance efficacy. It also compliments the findings of Julius et al. (2012) who examined the relationship between fear of falling and perceived walking effort in older adults with mobility limitations. They found that the rating of perceived walking effort is strongly related to balance. Cakit, Saracoglu, Genc, Erdem, and Inan (2007) also found in their randomized controlled study that improvements in cardiorespiratory function after 8 weeks of a speed-dependent treadmill exercise program were related to a significant decrease in fear of falling compared with a control group. Furthermore, 12 months of Tai Chi exercise training improved balance efficacy in frail older adults by improving cardiorespiratory function and self-esteem more so than participants in an educational class about fall prevention (Sattin, Easley, Wolf, Chen, & Kutner, 2005). In addition, the result of the association between balance efficacy and SOT score in the vestibular domain is supported by a study by Meli, Zimatore, Badaracco, De Angelis, and Tufarelli (2007). The authors found a strong relationship between vestibular function and anxiety by comparing the vestibular rehabilitation effect between a training and control group in patients with chronic vestibular deficits. Balance efficacy and anxiety level were significantly improved after a 10-week rehabilitation period.
Consequently, the results of the present study indicate that clinicians can use balance efficacy when screening for physical function (e.g., endurance, functional mobility) and the ability of older adults to successfully use their vestibular system to maintain their balance. Measuring physical fitness and postural control along with balance efficacy may be essential to fully understanding the contributing mechanism for an individual patient. For example, older adults with above average postural control who, counter intuitively, have low-balance efficacy may become more confident once they are shown their high postural control score and, consequently, lead a more active life, thus resulting in maintenance of or even improvements in postural control. However, without objective information about their balance, their low-balance efficacy might cause them to avoid physical activity. This could lead to detrimental declines in physical fitness, thus increasing the risk of falls. Therefore, measuring functional fitness after the balance test may aid clinicians in understanding the reason for low-balance efficacy and help them to decide appropriate interventions for an individual patient.
Nonetheless, this study is not without limitations. First, a history of falls increases fear of falling, but it has not been reported. However, the population in the present study consists of community-dwelling older adults, and based on their overall mean for 6-min walk and SOT score, they exceed population norms (Lord & Menz, 2002; Wolfson, Whipple, Derby, Amerman, & Nashner, 1994) for community-dwelling older adults. Second, it is possible that individual questions on the BES may have been rated differently in the present study; however, the present study only used the aggregate scores. In future studies, it would be of interest to divide groups between fallers and nonfallers based on their past real-life fall history and explore the relationship. Furthermore, the present study used an easy to implement battery of assessments to assess physical fitness in an older adult population. While this is a valid and reliable method, the battery relies heavily on human tester, which can lead to increased measurement error. Furthermore, this battery uses courser scales (e.g., 1 step) than some other measurement tools (e.g., Biodex balance system). Future research will benefit from the use of finer grained measurement tools. Finally, the results presented here are correlational, making us only able to hypothesize as to the causal nature of the relationship. The next step will be to conduct randomized control trials to further elucidate the cause of this relationship.
Conclusion
Based on the results of this study, functional fitness, as measured by the SFT, is more associated with balance efficacy than postural control, as measured by the SOT, in older adults. The present study suggests that consideration of balance efficacy is essential for clinicians while assessing functional fitness (e.g., aerobic endurance and functional mobility) and the ability to use the vestibular system to maintain balance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.