
Abstract
Family interventions have produced benefits on clinical and family outcomes in long standing psychosis. However, little is known about the efficacy of such interventions in the early stages of psychosis. This article reviews published research over the last two decades on family intervention in first-episode psychosis. Electronic databases, such as PubMed, PsycINFO, and ScienceDirect, have been systematically searched. In addition, an exhaustive Internet search was also carried out using Google and Google Scholar to identify the potential studies that evaluated family interventions in first-episode psychosis. We have identified seven reports of five randomized controlled trials (RCTs) and five non-randomized and uncontrolled studies of family intervention. Our review on 12 reports of family intervention studies has shown mixed effects on outcomes in first-episode psychosis. Most of the reports showed no added benefits or very short-term benefits on primary clinical or family outcome variables. There is a dearth of family intervention studies in first-episode psychosis. More RCTs are needed to reach reliable conclusions.
Background
The role of families in treatment of psychiatric patients has become increasingly important, mainly due to two reasons. First, some factors in family members’ behavior and attitude to patients such as criticality, hostility, and over-involvement, known as expressed emotion (EE), significantly predict relapse in individuals with prolonged psychosis (Barrowclough & Hooley, 2003; Pharoah, Mari, Rathbone, & Wong, 2010; Roseliza-Murni, Oei, Fatimah, & Asmawati, 2014) and first-episode psychosis (King & Dixon, 1999). Second, literature shows that providing care to a person with severe mental illness can adversely affect the mental health and well-being of family caregivers (Hayes, Hawthorne, Farhall, O’Hanlon, & Harvey, 2015; Hernandez & Barrio, 2015). Family members of individuals experiencing their first episode of psychosis have a higher risk of distress compared with family members of individuals with a prolonged course of illness (Martens & Addington, 2001; Sadath, Muralidhar, Varambally, Jose, & Gangadhar, 2014). Furthermore, the stress experienced by caregivers during the first episode can sometimes hamper recovery and even lead to a relapse (Tennakoon et al., 2000). Hence, there is a growing understanding among mental health professionals about the need to help the family caregivers along with the patients. Consequently, family interventions are now strongly recommended in many standard clinical practice guidelines for the treatment of schizophrenia (Kreyenbuhl, Buchanan, Dickerson, & Dixon, 2010) and early psychosis (International Early Psychosis Association Writing Group, 2005).
Over the last two or three decades, there has been an increased trend in identifying and treating psychosis, especially schizophrenia, in the early course of illness (Lieberman & Fenton, 2000). It is based on the rationale that significant clinical and psychosocial dysfunction in psychosis occurs in the first 5 years after the onset of illness (Reed, 2008), and many of such deteriorations are irreversible in later stages. Longer untreated psychosis is associated with greater risk of declining performance at school or work, social isolation, depression, suicide, drug or alcohol abuse, and aggressive behaviors (Onwumere, Bebbington, & Kuipers, 2011). Thus, early intervention is critical to achieve better clinical and functional outcome (“International Clinical Practice Guidelines for Early Psychosis,” 2005) and prevents long-term disability associated with psychosis (Reed, 2008). However, medication alone is not enough to prevent long-term disability or guarantee functional recovery from psychosis (Killackey, 2009).
The evidence for the effectiveness of family interventions in psychosis with prolonged course is well established through systematic reviews and meta-analysis of outcome studies. Such reviews report that family interventions reduce the risk of relapse and hospital readmissions (Pharoah, Mari, Rathbone, & Wong, 2006; Pharoah et al., 2010; Pitschel-Walz, Leucht, Bauml, Kissling, & Engel, 2001) improve compliance with medication, enhance general social functioning, decrease in levels of EE within the family (Pharoah et al., 2006) and improvements in knowledge and coping (Okpokoro, Adams, & Sampson, 2014) have been documented. However, most of the previous research has been conducted in caregiver populations associated with a more prolonged exposure to schizophrenia, and the effects of family interventions in the early stages are largely unknown (Askey, Gamble, & Gray, 2007). To date, there are a limited number of studies that have examined the use of family intervention with first-episode psychosis. Situating within this knowledge gap, the current article aimed at reviewing the published research on family intervention in first-episode psychosis. This review is different from the other systematic reviews in this area with respect to the focus and the number of reports reviewed.
Current Review Versus Previous Reviews of Family Intervention in FEP.

Note. FEP = first episode psychosis, RCT = randomized controlled trial.
The following is the key question addressed by this review:
What is the evidence of family interventions improving clinical and family outcome in first-episode psychosis?
Eligibility Criteria
Articles published in English language during the last two decades were considered for the review. Studies were included if they were family intervention study reports that evaluated either clinical outcomes or family outcomes or both after family intervention in first-episode psychosis. There is no uniform definition for first-episode psychosis in scientific literature (Breitborde, Srihari, & Woods, 2009). It has been defined in terms of patients’ first treatment contact (Craig et al., 2004); duration of antipsychotic medication use (Breitborde et al., 2009); and duration of psychosis (Castro-Fornieles et al., 2007). As each definition as its own strength and weaknesses (Breitborde et al., 2009), we included all studies that fulfill any one or all the above definition for first-episode psychosis.
Multi-element intervention studies in FEP were excluded as the current review aims at understanding the evidence of a single intervention (family intervention). To clarify, family interventions were given in many early intervention trials along with patient-oriented pharmacological and non-pharmacological interventions such as social skill training, cognitive–behavioral therapy (CBT) and crisis intervention (Bertelsen et al., 2008; Craig et al., 2004; Grawe, Falloon, Widen, & Skogvoll, 2006; Jeppesen et al., 2005; Kuipers, Holloway, Rabe-Hesketh, & Tennakoon, 2004; Petersen et al., 2005; Tempier, Balbuena, Garety, & Craig, 2012). Such study reports were not included because it was difficult to isolate the efficacy of any single intervention (family intervention) effectiveness. Family-oriented non-interventional study reports were excluded as they were not meeting the review aim.
Search Strategy
Studies were identified by searching electronic databases and scanning reference list of retrieved articles and systematic reviews. This search was applied to PubMed, PsycINFO, and ScienceDirect, with each database being searched from 1994 to 2014. An exhaustive Internet search was also carried out using Google and Google Scholar. The last search was run on July 31, 2014. The following search terms with a combination of two or more were used to identify potential studies: family intervention, family therapy, family work, family psycho education, first-episode psychosis, first-episode schizophrenia, early psychosis, and recent onset psychosis. The first author (A.S.) performed initial literature searches and screening of the articles from the electronic databases and Internet sources.
Data Extraction
Our review is a qualitative systematic review, and the data extracted from the selected studies were summarized but not statistically combined. The first author (A.S.) and the fourth author (J.P.J.) independently extracted data from the included studies. Disagreements were resolved by discussion between the two review authors. Variables extracted included the authors of the study, publication year, aim of the study, participants, setting, primary outcome measures, nature and type of intervention, number of sessions and period of intervention, comparison group details for RCTs, assessment timeline, dropout, and results. Furthermore, information necessary for evaluating methodological quality was extracted from the included RCTs (Figure 1).

PRISMA flow diagram (Moher, Liberati, Tetzlaff, & Altman, 2009).
Quality Assessment
There is no uniform standardized method to assess the quality of studies in systematic reviews (van Tulder, Furlan, Bombardier, & Bouter, 2003). We used a checklist recommended by van den Berg, Schoones, and Vliet Vlieland (2007), which was based on the guidelines for systematic reviews as set by the editorial board of the Cochrane Collaboration Back Review Group (van Tulder et al., 2003). This checklist consisted of 13 items that had been developed for their systematic review on Internet-based physical activity interventions. However, we have removed two items, “description of compliance with intervention” and “timing of assessment comparable” as they were not perceived relevant to family intervention studies. Methodological quality was rated independently by the first author, checked and verified by the fourth author. Each item was rated “yes,” “no,” or “unclear.” A total score was calculated by summing up all the “yes” items. Studies were rated as having good methodological quality if they score 8 or more in a total score of 11.
Results
Methodological Quality of the Family Intervention RCT’s
The results of the methodological quality assessment are described in Table 1. This assessment included five RCTs (Gleeson et al., 2009; Leavey et al., 2004; Linszen et al., 1996; McCann et al., 2013; Zhang, Wang, Li, & Phillips, 1994) for this quality assessment and excluded two reports (Lenior, Dingemans, Linszen, de Haan, & Schene, 2001; Lenior, Dingemans, Schene, Hart, & Linszen, 2002) as those were the follow-up assessments of one RCT.
Assessment of Methodological Quality in Randomized Control Trials.
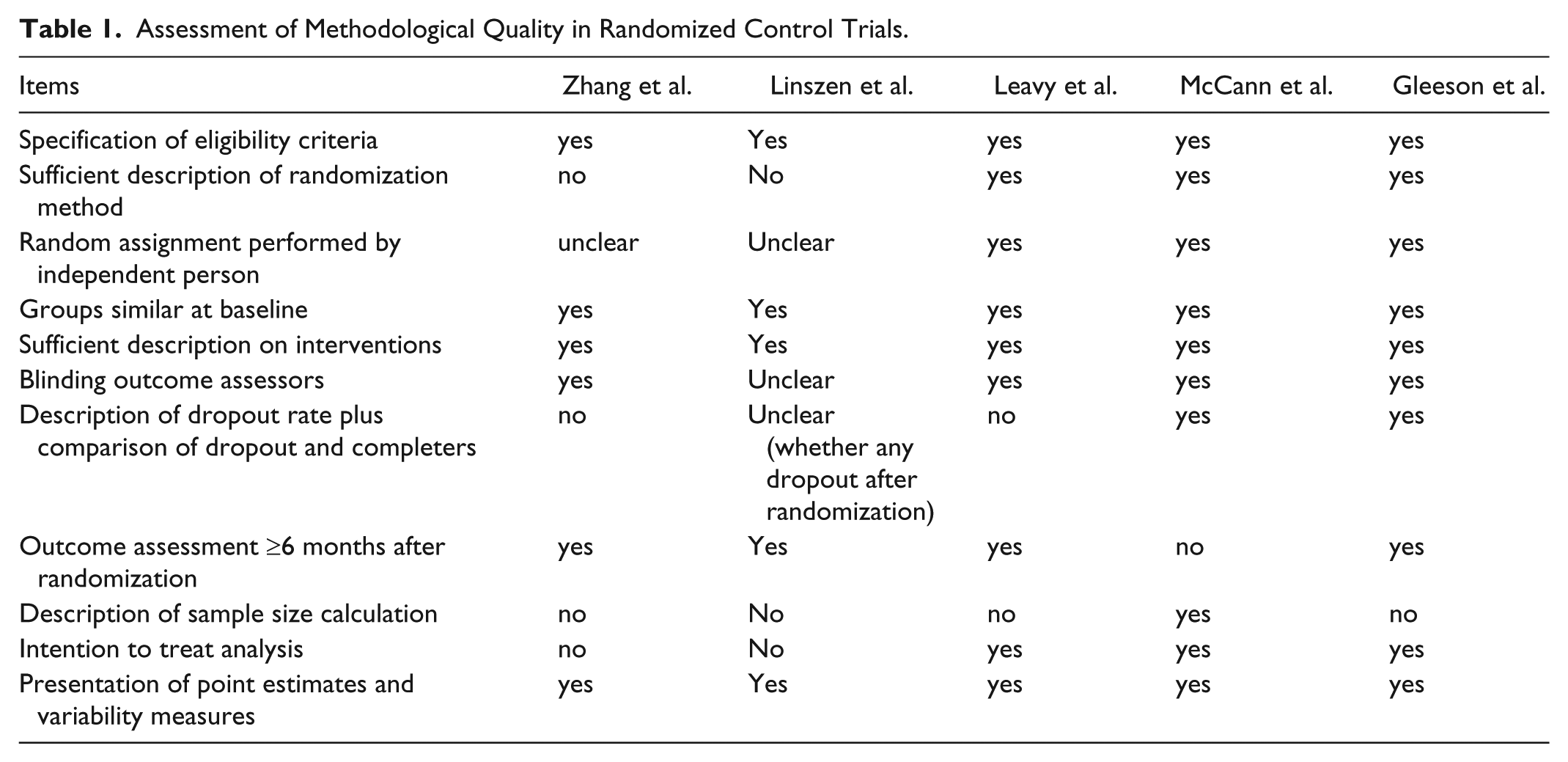
Of the 5 studies included, 3 (Gleeson et al., 2009; Leavey et al., 2004; McCann et al., 2013) were scored 9 or above and rated as having good methodological quality, whereas 3 studies (Linszen et al., 1996; Zhang et al., 1994) scored 6 and 5, and therefore, these studies could not fulfill the current study’s criteria for having good methodological quality.
Study Characteristics
As per the selection criteria, a total of 12 reports from 10 studies were selected and reviewed. The designs of these studies included five RCTs (see Table 2). The two reports of Lenior et al. (Lenior et al., 2001; Lenior et al., 2002) were follow-up studies of Linszen et al. (1996). There were five non randomized and uncontrolled designs which included three ‘pretest-posttest ‘studies, one longitudinal cohort study, and one had a posttest-only design (see Table 3).
Family Intervention Randomized Controlled Trials.

Note. BPRS= brief psychiatric rating scale, EE = expressed emotion, TAU= treatment as usual.
Family Intervention Non-Randomized and Uncontrolled Studies.

Note. EE = expressed emotion.
In 5 RCTs, a total of 465 participants were included (range from 76 to 124), whereas the total sample size of 2 pretest–posttest designs were 78 (sample size were 24, 31, and 23). The 1 longitudinal cohort study had 185, and the posttest-only design had 65 participants.
Overview of Family Interventions
The interventions of the randomized trials were family psychoeducation mostly with the components of education, support, communication and problem-solving techniques (Leavey et al., 2004; Linszen et al., 1996; Zhang et al., 1994), problem-solving bibliotherapy (McCann et al., 2013), and relapse prevention therapy with psychoeducational therapy, CBT, and family therapy components (Gleeson et al., 2009). In the majority of the family intervention trials, both families and patients participated in intervention programs (Gleeson et al., 2009; Leavey et al., 2004; Linszen et al., 1996; Zhang et al., 1994).
The number of intervention sessions varied across studies. In the study by Zhang et al. (1994), the intervention was provided for 18 months and families received a minimum of 1 session every 3 months. Linszen et al. (1996) used an 18-session treatment protocol for 12 months, sessions were provided bi-weekly during the first 5 months and monthly during the remaining 7 months. Leavey et al. (2004) used brief intervention package and provided over seven sessions and each session lasting an hour. McCann et al. (2013) used problem-solving bibliotherapy intervention, and caregivers worked independently through the module over 5 weeks. In this intervention, the caregivers were instructed not to finish more than one module per week. Finally, the study of Gleeson et al. (2009) used relapse prevention therapy for 7 months, and sessions were provided fortnightly (see Table 4).
Family Intervention of Randomized Controlled Trials.

Note. EE = expressed emotion; CBT = cognitive–behavioral therapy.
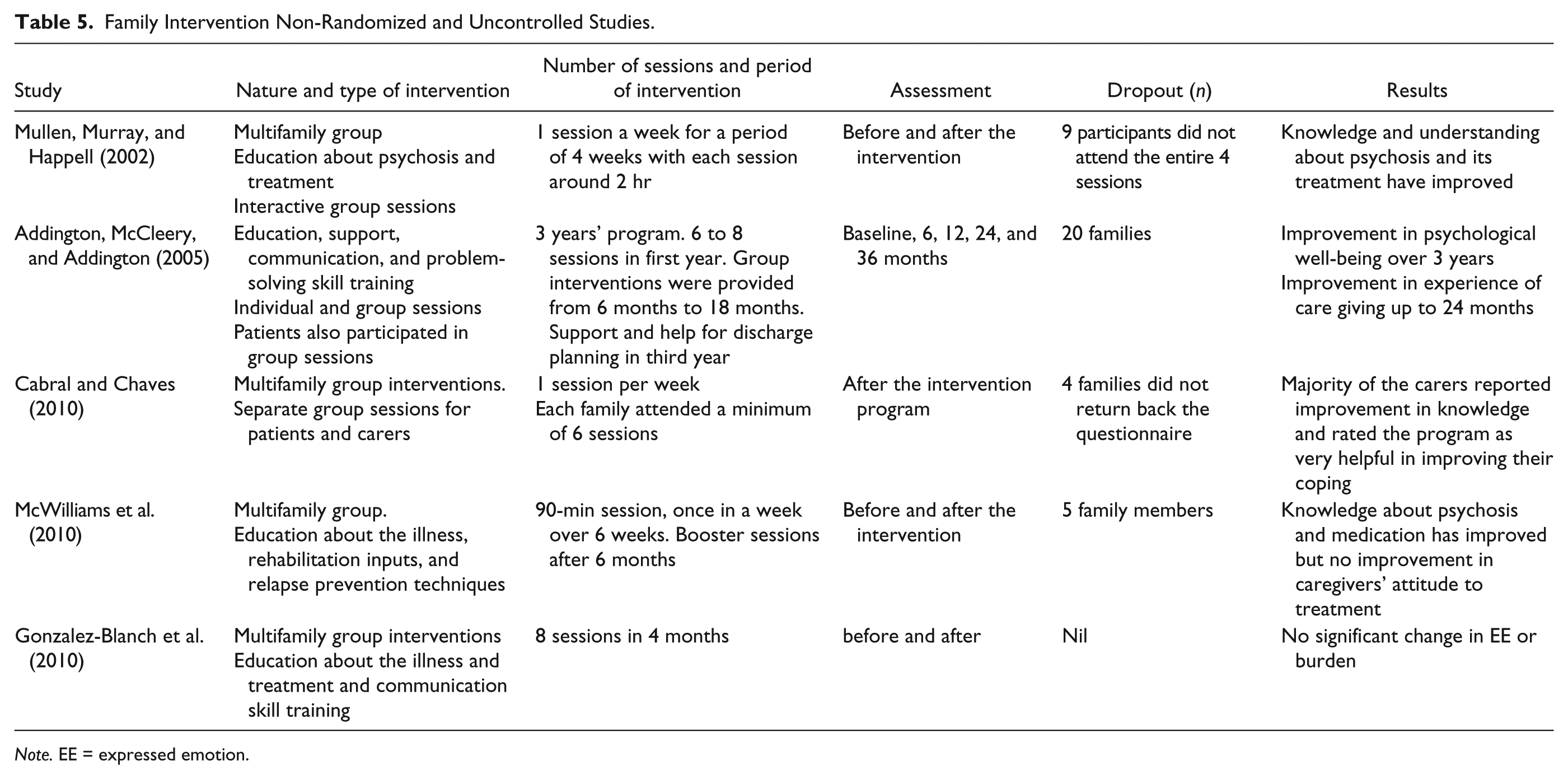
Among the non-randomized uncontrolled trials, a longitudinal cohort used 3 years of long-term family intervention (Addington, McCleery, & Addington, 2005). In this study, on average, families received seven sessions during the first year, two to four sessions in the second year, and two to three sessions in the third year. The intervention sessions in other non-randomized and uncontrolled studies were very brief and time-limited with a minimum of 1 session in a week for a period of 4 weeks (Mullen, Murray, & Happell, 2002) and 6 weeks (Cabral & Chaves, 2010) to a maximum of eight sessions in 4 months (Gonzalez-Blanch et al., 2010; see Table 5).
Family Intervention Non-Randomized and Uncontrolled Studies.
Note. EE = expressed emotion.
Clinical or Family Outcome
Of the six reports that examined the efficacy of family intervention on clinical outcomes, only three reports showed significant benefits. One report (Zhang et al., 1994) showed benefits on hospital readmission, hospital-free period, clinical status, and overall functioning of the patients, over 18 months follow-ups. A 5-year follow-up assessment of Linszen et al.’s (1996) study by Lenior et al. (2001) reported some benefits on duration of stay in hospital for patients. The other report (Gleeson et al., 2013) showed short-term benefits (12 months) in relapse rate and long-term benefits (30 months) in medication adherence.
Four reports examined the caregiver/family-related outcomes, of which only 1 report (McCann et al., 2013) showed benefits on EE (6 weeks), care giving experience, and caregivers’ psychological distress (16 week). However, the follow-up assessment of this trial was just 16 weeks; therefore, it is difficult to comment on the longer benefits.
Outcomes of Non-Randomized and Uncontrolled Studies
A longitudinal cohort study by Addington et al. (2005) assessed the effectiveness of individualized family intervention integrated within a comprehensive treatment program for first-episode psychosis. The results showed improved psychological well-being and care giving experiences in follow-up at 36 months. Most of the single group pretest and posttest studies and one posttest-only study reported favorable outcomes. These studies evaluated the usefulness of a multifamily group psychoeducation in improving family members’ knowledge and understanding about psychosis and related management strategies. The result showed improvement in the family members’ knowledge (Cabral & Chaves, 2010), understanding, and management of psychosis from pretest to posttest (McWilliams et al., 2010; Mullen et al., 2002). An exception to the above trend, the pretest and posttest study of Gonzalez-Blanch et al. (2010) evaluated the effect of eight sessions of multifamily group psychoeducation on carers’ burden and EE. However, this study could not demonstrate any benefits of the intervention on caregivers’ burden or EE.
Discussion
Although many systematic reviews have reported positive outcomes of family interventions for caregivers and patients with prolonged psychosis (Pharoah et al., 2006, 2010; Pitschel-Walz et al., 2001), the present review of RCTs on family interventions in first-episode psychosis shows mixed results. The majority of family intervention RCT reports showed that the intervention had no added benefit on any of the primary clinical or family outcome variables (Leavey et al., 2004; Lenior et al., 2001; Lenior et al., 2002; Linszen et al., 1996) or showed only short-term benefits on either clinical or family outcomes (Gleeson et al., 2013; McCann et al., 2013), and most such benefits were not sustained at follow-ups, the periods ranging from 4 months (McCann et al., 2013) to 5 years (Lenior et al., 2001; Lenior et al., 2002).
Some of the plausible explanations for such mixed results are discussed here. In some trials (Gleeson et al., 2013; McCann et al., 2013), the family members were recruited from established early intervention services whereas family intervention was compared with specialist first-episode psychosis care. It was observed that these special clinics followed structured intervention programs including family interventions. Hence, the possibility of an unintentional exposure of similar intervention in control group cannot be ruled out completely. A similar problem was observed with another trial also (Linszen et al., 1996).
Although we could not find any major impact of the number of sessions on study outcomes, the favorable outcome reported in many studies were not sustained for a long period after the interventions ended (Gleeson et al., 2013; McCann et al., 2013). It was also observed that a few trials (Leavey et al., 2004; McCann et al., 2013) had very brief interventions, which were far below the treatment recommendation developed by the Schizophrenia Patient Outcome Research Team, who suggested that the family psychosocial interventions be offered for a minimum period of 6 to 9 months (Kreyenbuhl et al., 2010). Furthermore, many family intervention studies that reported favorable outcome in long standing psychosis used the interventions ranging from 9 months to 2 years (Barrowclough et al., 2001; Carra, Montomoli, Clerici, & Cazzullo, 2007; Dyck, Hendryx, Short, Voss, & McFarlane, 2002).
It was observed that the outcome variables across studies reviewed here were varied. Consistently, family interventions (mostly with prolonged psychosis) reported to have benefits on relapse rate, medication compliance, reduced hospital admission, and improvement in family atmosphere (Pharoah et al., 2010). Although some of these outcomes had already been evaluated in a few of the family intervention FEP studies, there is a need to measure those outcomes in more studies to establish evidences. We also compared the differences in intervention techniques used in prolonged psychosis and first-episode psychosis. Although we could not identify any major differences in intervention, some of the interventions used in prolonged psychosis such as motivational interviewing, crisis-oriented family intervention, and relaxation training were not well utilized in FEP.
Furthermore, the interventions used in studies were not based on the identified needs of the family members. A few trials (Leavey et al., 2004; Linszen et al., 1996) used established family intervention packages for prolonged schizophrenia, and it is unclear as to whether the needs of the families in the early period of psychosis are similar to that in prolonged psychosis. It should also be noted that we have not excluded any RCTs based on the methodological quality assessment. One trial (Linszen et al., 1996), which scored less as compared with other trials, had two follow-up reports (Lenior et al., 2001; Lenior et al., 2002), and all three reports had shown no significant benefits. Furthermore, the majority of the family intervention trials that did not describe their sample size calculation had fewer participants. Hence, we are unsure whether these studies had enough statistical power to detect intervention effect.
The majority of the non-randomized and uncontrolled studies primarily evaluated families’ knowledge and understanding about the illness and its management. These studies have reported benefits of improved knowledge and understanding (Cabral & Chaves, 2010; McWilliams et al., 2010; Mullen et al., 2002). However, whether the enhanced knowledge translates into benefits such as reduction of distress, improved coping, or relapse prevention is not clear.
Recommendations
Future studies may need to address the aforesaid issues and limitations. First, the family intervention needs to be provided at least 6 to 9 months to sustain significant clinical or family-related outcome benefits. Second, there should be some additional or unique intervention components for the family intervention group, which is not provided as the part of standard care or treatment as usual. To clarify, most of the family intervention trials that we have reviewed here received psychoeducation with the components of education, support, and communication skill training. As we have discussed elsewhere, there may be chances that the comparison group also would have received similar intervention as part of comprehensive early intervention services. Third, the studies need to explore the specific needs of caregivers and the family intervention to be provided according to their identified needs. Finally, qualitative feedback can be collected from the family caregivers after family intervention. This would help us to understand and modify our intervention strategies based on what components of interventions were helpful/not helpful and what area they feel improved or not improved.
Conclusion
It is evident that there is dearth of studies on family interventions in first-episode psychosis as only 12 relevant papers was found to have been completed on the topic over the last two decades. In the absence of well-substantiated evidence base, it is difficult to take empirically informed decisions in clinical practice. Furthermore, there is also little available material on specific needs of patients and caregivers in first-episode psychosis. Therefore, it is vital to develop and validate a need-based family intervention framework to guide clinical practice in first-episode psychosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.