
Abstract
Previous studies have shown that gender may moderate the relationship between religiousness and mental health in most countries, but few studies have been conducted in Norway and Denmark. This study examined gender differences in religious experiences and church attendance as predictors of existential well-being among 295 women and 233 men from the general Norwegian population. Analyses showed that the structural equation models for women and men did not differ significantly on the global level. The models for women and men, however, showed different patterns. Among men, church attendance and negative religious experiences predicted existential well-being; among women, positive and negative religious experiences were related to existential well-being, but church attendance was not. The present findings suggest that men may benefit more from active religiousness, whereas women may benefit more from affective religiousness. Comparing these results with research in other cultural contexts, we find that different operationalizations of church attendance yield the same types of patterns across cultural contexts. Consequently, the benefits of religiousness may be similar for women and men irrespective of cultural context.
The relationship between religiousness and mental health is generally found to be stronger for women compared with men (C. G. Ellison & Fan, 2008; Hintikka, 2001; Krause, Ellison, & Marcum, 2002; Lewis, Shevlin, Francis, & Quigley, 2011; Maselko & Kubzansky, 2006; McCullough & Laurenceau, 2005; McFarland, 2010). Nevertheless, studies from Norway and Denmark indicate a different pattern where religiousness and mental health, including social support, are more strongly associated for men than for women (Hvidtjørn, Hjelmborg, Skytthe, Christensen, & Hvidt, 2014; Kvande, Reidunsdatter, Løhre, Nielsen, & Espnes, 2015; Sørensen, Dahl, et al., 2012; Sørensen, Danbolt, Holmen, Koenig, & Lien, 2012). This is despite results from both international and Scandinavian studies where women tend to be more religious than men (see Francis, 1997, for a review; Hintikka, 2001; Hvidtjørn et al., 2014; Sørensen, Lien, Holmen, & Danbolt, 2012).
Several important factors distinguish Norway, Denmark, and with the rest of Scandinavia from Europe and the United States, where most studies on religiousness and health have been conducted. First, the majority of people in both Norway and Denmark are secular, and few are highly religious. For instance, in 2008, only about 13% to 15% of Norwegian and Danish people reported having strong beliefs in God, whereas 61% of the U.S. population report such beliefs (National Opinion Research Center [NORC]/University of Chicago, 2012). Second, church attendance rates in Norway and Denmark are among the lowest in the world. Data from the European Social Survey Round 6 Data (2012) indicate that about 5% of Norwegians and 4% of the Danish people attend church weekly or more often. This is different from the United States where about 43% of the population attend church 3 or more times per month (Gallup, 2010). Finally, Norway is considered one of the most gender-equal countries in the world in terms of women’s participation in the public sphere outside the home (Bekhouch, Hausmann, Tyson, & Zahidi, 2013; Lopez-Claros & Zahidi, 2005). This may influence the development of gender roles in society including women and men’s involvement in religion, and it may affect religion’s associations with health and well-being. Thus, it appears that religion may function differently for men and women, depending on social context, as well as the particular domains of religiousness and mental health that are being examined.
The present study explores gender differences in two domains of religiousness—church attendance and religious experiences—and measures their associations with existential well-being (EWB) in a Norwegian context. Gender differences in the relationship between religiousness and mental health could be linked to how women and men cope with adversities, including mental health problems, but they may also be linked to gender differences in active versus affective domains of religiousness. We also explore different operationalizations of concepts such as church attendance, which may also account for the divergent findings across contexts.
Gaining knowledge of potential gender differences related to the functional aspects of religion would not only be helpful in a clinical perspective but may also be important for further theoretical developments regarding religiousness and gender. Although religious experience has been defined and operationalized in many different ways, Beit-Hallahmi and Argyle (1997) argue that religious experiences may still have a common core characterized by a wholeness of all things, timelessness, sense of reality, and blessedness. In addition to a common core, religious experiences also have different varieties, which are not commonly agreed on by scholars. Two dimensions of religious experiences are emphasized by Beit-Hallahmi and Argyle; the distinction between the immanent and the transcendent, and the social and individual. The immanent versus the transcendent refers to a unity of all things within oneself versus a connection with a transcendent being outside the universe. The social versus individual dimension reflects the importance of social setting, inasmuch that religious experiences may occur in social settings or in solitude. According to Beit-Hallahmi and Argyle, religious experience is therefore a multidimensional phenomenon, which covers several types of experiences from feelings of peace and unity with all things and being close to a spiritual force, but which also includes intense sensations such as out-of-the-body experiences, having contact with the dead, and telepathy.
Although recognizing religious experiences to be a multidimensional phenomenon, some researchers have emphasized one dimension rather than many. Here, the focus is more on a subjective experience of the transcendent, which Glock and Stark (1965) have categorized as differing in intensity ranging over four levels: “a confirming experience, a responsive experience, the ecstatic experience and the revelational experience.” The latter two are the least common and contain more powerful perceptions and sensations with an increasingly intimate closeness to the divine in a perceived two-way interaction (Glock & Stark, 1965). However, a confirming experience and a responsive experience reflect a person’s everyday feelings and sensations in association with the transcendent. Such everyday experiences have also been described by King (1967) as “personal religious experiences” and how one’s personal life may be influenced by the transcendent (God). This includes a sense of God’s presence, being in close communion with God, and being heard and cared for. Such religious experiences are associated with well-being and other positive mental health outcomes. For instance, in a French study on participants aged 65 years and older, researchers found a positive correlation between religious experiences and self-rated health and life satisfaction (Bailly & Roussiau, 2010). Another U.S. study showed that spiritual/religious experiences were a strong predictor of happiness, life excitement, satisfaction with self, and optimism (C. G. Ellison & Fan, 2008).
In its position as one of the most studied domains of religiousness, church attendance is repeatedly associated with mental health. For instance, a U.S. study found that church attendance was positively associated with well-being and negatively associated with distress (C. G. Ellison, Boardman, Williams, & Jackson, 2001). Furthermore, a Dutch study found higher levels of church attendance to be negatively related to depressive symptoms (Braam et al., 2004). This study controlled for a range of confounding variables that may influence the outcome, such as age, gender, education, marital status, chronic disease, self-esteem, and emotional support. Others have also found church attendance to be positively associated with optimism, self-esteem, and well-being and negatively related to death anxiety, mortality, and depression (Baetz, Bowen, Jones, & Koru-Sengul, 2006; L. B. Koenig & Vaillant, 2009; McFarland, 2010; Strawbridge, Shema, Cohen, & Kaplan, 2001).
Women are often found to experience greater benefits from religion compared with men. A study from Northern Ireland found the level of church attendance to associate with well-being for both genders, but the relationship was stronger for women (Lewis et al., 2011). As Lewis et al. (2011) also accounted for denominational differences, church attendance had a stronger association to well-being for Catholic women and men compared with Protestants. Furthermore, a study conducted on the Finnish general population found a significant relationship between religious attendance and less mental health disorders among women but not among men (Hintikka, 2001). Religious experiences may also be a greater benefit for women. Findings from the U.S. General Social Survey in 1998 (but not for 2004) revealed that having daily spiritual experiences was related to greater levels of happiness and self-satisfaction for women but not for men (C. G. Ellison & Fan, 2008). Moreover, a prospective study found that women who were highly religious (equal to high levels of organizational and private religiousness combined) in early life reported a higher mean level of self-rated health throughout life compared with less religious women, a difference not evident for men (McCullough & Laurenceau, 2005). Finally, weekly religious attendance and spiritual experiences predicted well-being for women but weekly religious attendance was more strongly related to well-being for men (Maselko & Kubzansky, 2006).
In general, it may be maintained that women experience more mental health benefits from several domains of religiousness compared with men—however, the empirical findings are somewhat ambiguous. For instance, in a prospective study on U.S. adults aged 66 to 95 years, high levels of religious involvement decreased symptoms of depression and increased levels of optimism and self-esteem for men, but not for women (McFarland, 2010). Furthermore, a second prospective study found church-based social support to be positively associated with self-rated health for men but not for women (Krause et al., 2002). Such long-term benefits for men were evident despite higher levels of emotional support among women.
Although research is sparse on relationships between religiousness and health in Norway, a couple of studies support gender differences. A cross-sectional population study found younger religious men (18-39 years) to report significantly higher levels of tangible and emotional support compared with younger non-religious men (Kvande, Reidunsdatter, et al., 2015). Younger religious women, however, experienced less tangible support and the same level of emotional support compared with younger non-religious women. Furthermore, a large population study found church/prayer house attendance to moderate the positive relationship between death of a close relative and depression (Sørensen, Danbolt, et al., 2012). The influence of church attendance on depression differed for men and women. Among men, lower depression rates were associated with more frequent religious attendance, whereas among women, lower depression rates were associated with less frequent religious attendance.
Although there are several approaches to explaining gender differences in religion (e.g., structural location theories, socialization theories), the differential mental health benefits from religiousness for women and men are rarely addressed. Personality theories posit that general psychological or physiological differences in the personalities of women and men cause women to be more attracted to religion compared with men. Also, higher levels of general risk taking associated with less religiousness are observed for men, with the opposite pattern for women. These differences are linked to physiological distinctions across gender, which may lead to differences in their relationship to religion (Cornwall, 2009; de Vaus & McAllister, 1987; Francis, 1997; Miller & Hoffmann, 1995; Stark, 2002; Sullins, 2006). The use of religion as a stress buffer for poor mental health is evident within theories on personality. Thus, as women more so than men struggle with internalizing such mental health disorders as anxiety and depression (Rosenfield & Mouzon, 2013), women may use religion to protect themselves from threats to their mental health. Also, as women tend to engage in more emotion-focused coping and turn to their social networks more often than men do (Rosenfield & Mouzon, 2013), both church attendance and religious experiences might influence women’s well-being more than men’s. Nevertheless, one Danish study found that although women were generally more religious, religious men within the most religious subsample were more inclined to use religious coping (Hvidtjørn et al., 2014). This finding by Hvidtjørn et al. (2014) is in line with another study of 480 hospitalized Danish patients where religiousness became more pronounced for men as severity of an illness progressed. For women, severity of illness correlated with lower scores on the religiousness variables (la Cour, 2008).
Viewed together with the Norwegian research by Kvande, Klöckner, Moksnes, and Espnes (2015) on social support and by Sørensen, Danbolt, et al. (2012) on depression, the relationship between religiousness and mental health may show different mechanisms across gender. Religiousness seems to be particularly beneficial for the men in these studies in terms of coping and social support, and it may become more important to men compared with women when faced with illness. Furthermore, although women are generally found to be more religious than men, they seem to express their religion differently. Whereas women engage in the more subjective or affective dimensions of prayer or comfort from religion, men are more engaged in church attendance, church membership, or volunteerism (Sullins, 2006). Sullins (2006) examined people’s use of the active and affective dimensions of religion based on data from both the General Social Survey (1998-2002) and the International Social Survey Programme (1998) and found a larger difference between women and men in the affective dimensions than in the activity dimensions. These findings lead one to ask whether active religiousness is more influential to men’s well-being, and affective religiousness is more beneficial to women’s well-being.
Few empirical studies have investigated associations between both affective and active domains of religiousness and well-being from a gender perspective. This study is particularly relevant to discussions of religion as a potential facilitator for positive mental health outcomes among the general population. Based on the literature reviewed above, with the exception of the Scandinavian studies, women’s well-being seems to be more strongly related to church attendance and religious experience as compared with men. However, others argue that women rely on the affective rather than active domain of religiousness, with the opposite pattern for men (Sullins, 2006). The Scandinavian studies reviewed here show that although at least one study found women to be more involved in religion compared with men (Sørensen, Lien, et al., 2012), the relationship between religiousness and beneficial mental health outcomes seems to be stronger for men.
Across the research literature, we note that church attendance is operationalized in different ways. Specifically, some studies view church attendance synonymously with attendance at services, but others extend this definition to include activities such as participation in prayer groups, bible study groups, or other meetings. When separating studies treating church attendance as merely worship service attendance, we find that women benefit more from church attendance (Hintikka, 2001; Lewis et al., 2011). However, men seem to benefit more in cases where the measures of church attendance reflect an extended range of activities in the church (Maselko & Kubzansky, 2006; McFarland, 2010). For example, the Norwegian study by Sørensen, Danbolt, et al. (2012) on church attendance and depression does not restrict church attendance to worship service attendance because respondents are asked, “How often in the last six months have you been to church or a house of prayer?” Consequently, the divergent findings across nations may be linked to different measures of church attendance. If so, a differential association between church attendance and well-being and between religious experiences and well-being for men and women may be linked to the distinction between “active men” and “affective women.” That is, women may benefit more from affective domains of religiousness, and men more from active domains across contexts.
The present study was conducted with the aim of examining gender differences in associations between church attendance and well-being—and between religious experience and well-being—while controlling for the influence of education, age, and long-standing health problems. Because of the dearth of research on religion–health associations in a secular context in general, and on gender differences in religion–health associations in particular, specific hypotheses are not formed to guide the present study. However, based on the above theoretical perspectives and empirical studies, the present study will explore questions organized in two areas:
Do differential associations exist between religiousness and well-being among men and women? If associations between church attendance and well-being, and between religious experiences and well-being, differ for women and men, the functional benefits of religion may vary depending on gender. Women and men may differ in terms of which mental health problems they experience, as well as in how they cope with those problems. As some have argued that men are more involved in active domains of religiousness, and women more involved in affective religiousness, we also ask whether this pattern applies to mental health benefits from religion. Thus, is church attendance more strongly linked to well-being for men, and religious experiences more strongly linked to well-being for women?
Are gender differences in associations between church attendance and mental health equal across contexts? Different operationalizations of church attendance may be related to whether studies find women or men to benefit the most from church attendance. If men benefit more in a Norwegian context where church attendance may reflect more than merely service attendance, findings in a Norwegian context may not be that different from findings in other cultures.
Method
Procedure and Sample
The data for this cross-sectional study were collected in 2009 from the general Norwegian population. An independent company, EDB Business Partner, randomly selected 3,000 individuals from the national registration office in two steps: First, 2,500 individuals between the ages of 18 and 75 were drawn, and then an additional 500 individuals between 60 and 75 years of age were drawn to increase the proportion of elderly participants (Figure 1). A questionnaire designed to address issues relating to health, religion, spirituality, view of life, and working life was sent to each respondent’s home address. One reminder was sent four weeks after the first mailing, and the total response rate was N = 653 (22%). When comparing responders with non-responders, we found no significant gender differences, χ2(1, N = 2,347) = 3.33, p = .068, but responders were significantly older than non-responders, mean age (SD) = 50 (16.2) versus 48 (17.1) years, t(1,043) = −3.44, p = .001. The chi-square test for significant gender differences approached significance, thus reflecting that a larger proportion of women participated in the study. For the present study, we used data from n = 539 participants due to incomplete data provided by the remaining n = 114 participants. We excluded respondents if more than 66% (50 items) of their responses were “not applicable” (based on the 76 religiousness items in the questionnaire with the possible “not applicable” response option). Consequently, proportions of data present across all single items in our models ranged from 65% to 94%. A comparison of the present sample with Norwegian population data (http://www.ssb.no/english) showed that our study sample had a lower proportion of younger respondents aged 18 to 39 (29% vs. 41%) and a higher proportion of older respondents aged 60 to 75 (38% vs. 21%). The present sample also had higher proportions of women (56% vs. 49%), higher levels of education (42% vs. 30%), a larger proportion of members of the Church of Norway (80% vs. 76%), and fewer with no church membership. Ethical guidelines were followed, and the study was approved by the Regional Committee for Medical Research Ethics (REK), and the Norwegian Data Inspectorate approved the collection of data.

Flowchart of study sample.
Measures
Demographics included questions on gender, age, education, and religious affiliation. The level of education was detected by providing three choices: (a) primary school, (b) high school, and (c) college/university. Religious affiliation was assessed by asking people, “are you a member of a religious community” with eight response options: (a) Church of Norway, (b) Evangelical Lutheran Free Church, (c) Roman Catholic Church, (d) Pentecostal movement, (e) Islamic community, (f) Norwegian Humanist Association, (g) No membership, (h) Other membership (open-ended question). The item on religious affiliation was developed for this study, and the listing of options was based on the largest communities in Norway in 2008 (Statistics Norway, 2013).
Long-standing health problems were assessed by the following question: “Do you suffer from any long-standing (at least one year) limiting somatic or psychiatric illness, disease or disability?” with a dichotomous response option (Yes, No). The item has been used in international studies (Ayis, Gooberman-Hill, Ebrahim, & Collaboration, 2003) and in population-based studies in Norway (Krokstad, Johnsen, & Westin, 2002; Løhre, Rise, & Steinsbekk, 2012).
Church attendance was assessed by three items from King and Hunt’s (1972) Dimensions of Religion Scale. Each participant was asked how frequently they engaged in three aspects of church attendance. The items used a 5-point scale ranging from low (1) to high (5), in addition to a sixth response option of (6) not applicable. The categories of possible response options differed between the three items. The first item, “How often have you taken Holy Communion during the past year?” included response options (1) never, (2) seldom, (3) occasionally, (4) fairly regularly, and (5) regularly. The second item, “During the last year, how many Sundays per month on average have you gone to a worship service?” was reported as (1) none, (2) one, (3) two, (4) three, and (5) four. The final item, “If not prevented by unavoidable circumstances, I attend church,” was reported as (1) never, (2) seldom, (3) monthly, (4) weekly, and (5) several times a week. The three items together comprised the dimension of church attendance. The previously reported Cronbach’s alpha for church attendance is .82 (King & Hunt, 1972), and for the present study, we found a Cronbach’s alpha of .89. As the measures of church attendance are appropriate for Christian denominations, we know less about its applicability to others. Consequently, we ran all structural equation models (SEM) performed in this study using only Christian participants. The patterns of associations were equal to the analysis performed on the total sample. This indicates that in a Norwegian setting, the measures apply equally well to the general population as to Christian denominations in particular.
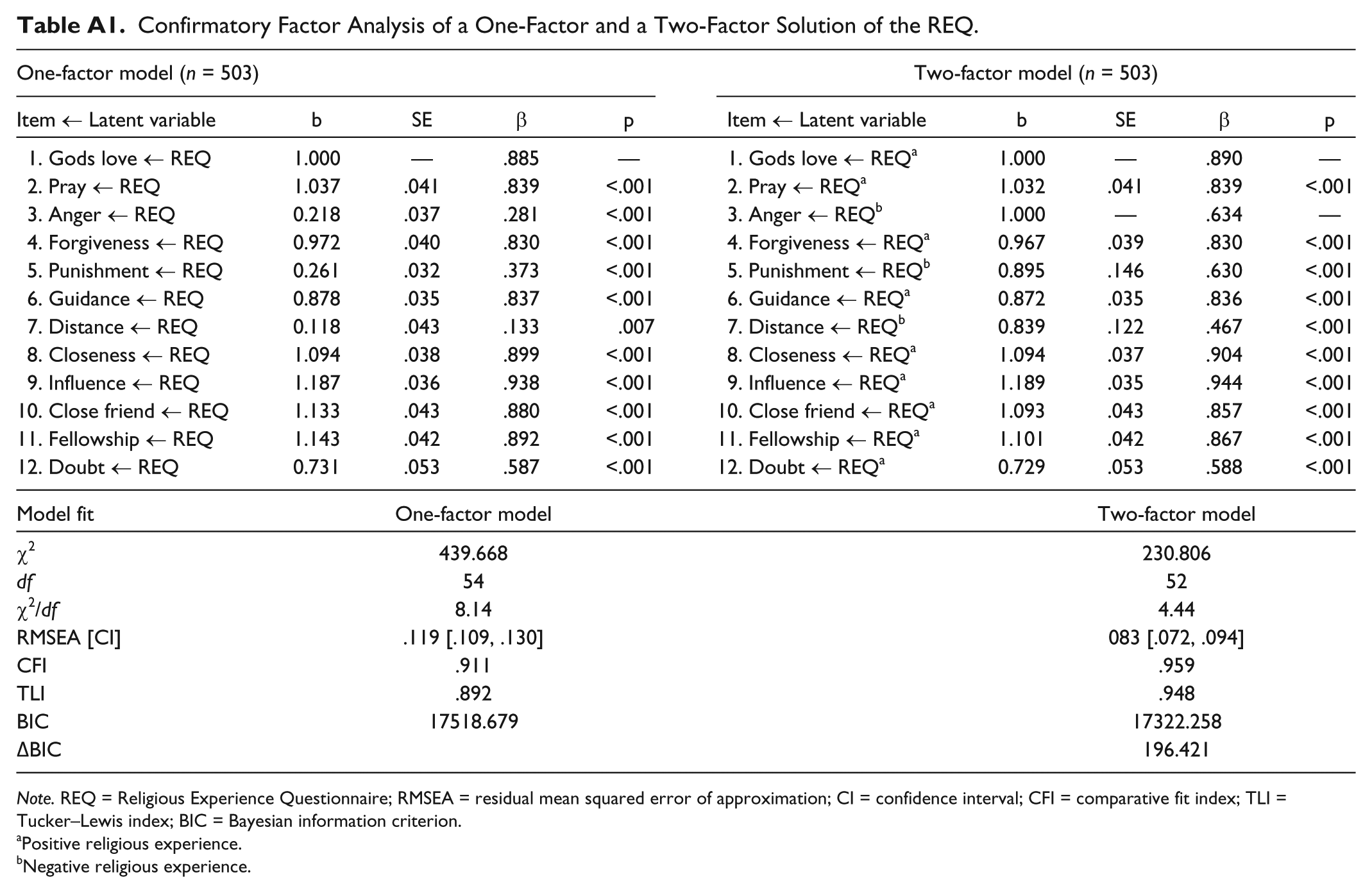
Religious experience was assessed using the revised version of the Religious Experience Questionnaire (REQ; Edwards, 1976). The REQ consists of 12 items (compared with 8 items in the original version) that were designed to reflect a personal affective relationship with God (Hill & Hood, 1999). The scale was developed following King (1967), with the dimension of “personal religious experience,” which was composed of items reflecting the perceived influence of God in one’s life, including feelings of being forgiven for sins and referring to God when making decisions. Examples of items in the REQ are “I experience an awareness of God’s love” and “I pray privately in places other than church.” The items were rated on a 7-point Likert-type scale with the response options (1) never, (2) almost never, (3) rarely, (4) sometimes, (5) often, (6) almost all the time, and (7) always. Although a one-factor structure of the REQ has previously been used by other researchers (Brokaw & Edwards, 1994; Tisdale et al., 1997), an examination of the factor structure for the present study’s Norwegian sample found better support for a two-factor structure (see appendix). Consequently, a two-factor structure with positive and negative REQ was used in this study, and Cronbach’s alpha for Positive REQ was .96 and for negative REQ .61.
Well-Being was assessed using one dimension of the Spiritual Well-Being Scale (SWB)—EWB (English SWBS © 1982, C. W. Ellison and R. F. Paloutzian. Norwegian translation SWBS © 2011, R. F. Paloutzian. All rights reserved). Twenty items compose the SWB Scale and distribute equally between religious well-being (RWB) and EWB (C. W. Ellison, 1983; Paloutzian & Ellison, 1982). EWB includes questions on contentment with meaning, purpose, and satisfaction in life. As opposed to RWB, EWB has no specific relation to God and religion. Examples of items are, “I feel that life is a positive experience” and “Life doesn’t have much meaning.” The items were rated on a 6-point Likert-type scale with response options (1) strongly agree, (2) agree, (3) somewhat agree, (4) somewhat disagree, (5) disagree, and (6) strongly disagree. The internal consistency of RWB and EWB is reported by others with Cronbach’s alphas of .79 and .87 (unknown order) for an African American sample (Utsey et al., 2007), and .78, .84, .87, and .91 for EWB in groups having members of four different religious communities (Genia, 2001). The present study found a Cronbach’s alpha of .82 for EWB.
All measures were translated from English into Norwegian by two bilingual native-Norwegian academics. Following this, the translation of all items was evaluated by a Norwegian academic working in sociology of religion to ensure correct item meaning.
Statistical Analysis
Frequencies were used to describe the sample on level of education, religious affiliation, and long-standing health problems. Means and standard deviations were calculated for age, church attendance, positive and negative religious experience, and EWB. Cronbach’s alpha was used to examine the internal consistency of church attendance, positive and negative religious experience, and EWB. All the above calculations (frequencies, mean, standard deviation, Cronbach’s alpha) were performed using SPSS Version 20.0 for Windows (SPSS, Inc., Chicago, Illinois, the United States). Multiple-groups SEM using Mplus software (Muthén & Muthén, 1998-2012) was used to calculate correlations between the latent constructs: frequency of church attendance, positive religious experience, negative religious experience, and EWB. Furthermore, we tested for significant mean differences on the four latent constructs across women and men. A p value of < .05 was regarded as statistically significant for all analyses in the present study.
SEM with maximum-likelihood estimation using Mplus software was used to evaluate the research questions. SEM is shown to have a number of advantages compared with other statistical techniques, such as multiple regression. SEM enables you to calculate complex models using both latent and single-item variables, to include cases with missing values, and to control for measurement errors when using latent variables (Geiser, 2013; Muthén & Muthén, 1998-2012). Prior to testing for significant gender differences in our SEM model, we tested for measurement invariance across gender to ensure the measurement model was equal for women and men. Then, we specified our model with direct effects from church attendance, positive religious experience, and negative religious experience on EWB. The model also controlled for the influence of education, age, and long-standing health problems on EWB. We used multiple-group modeling to test for significant gender differences. Hence, separate models for women and men are specified within the same overall model. The models were tested in three steps. First, we examined the overall model fit (Model 1) according to the residual mean squared error of approximation (RMSEA) with values less than .07 for adequate fit, and .03 for excellent fit (Steiger, 2007). Values of above .90 for the comparative fit index (CFI) and the Tucker–Lewis index (TLI) were regarded as good-enough fits (Hu & Bentler, 1999). These fit thresholds were used to evaluate all further models. Second, we performed a global test by comparing a constrained with an unconstrained model. In the first model, the three regression coefficients from the effect of church attendance, positive religious experience, and negative religious experience on EWB were constrained so they were equal between genders. In the second model, the regression coefficients were free to vary, and the two models were evaluated by comparing chi-square statistics, absolute goodness-of-fit indices, and the Bayesian information criterion (BIC). When comparing models on BIC, unit changes of >10 across models were regarded as very strong indices showing that the model with the lowest BIC fits the data better (Kass & Raftery, 1995). In our third step, each of the three regression coefficients from the effect of church attendance, positive religious experience, and negative religious experience on EWB was tested for significant differences across gender using the Wald test for parameter constraints. Three separate models were run, each constraining one of the three regression coefficients so it was equal across gender.
In all analyses using Mplus software, missing data were processed using full information maximum-likelihood (FIML) estimation and included both system missing data and responses of “not applicable” on single items on church attendance and religious experience. FIML is regarded as one of the most robust methods for dealing with missing data (Schlomer, Bauman, & Card, 2010). To determine the procedure for handling missing responses, Schlomer et al.’s (2010) guidelines for best practice for evaluating missing values were followed. We therefore evaluated the pattern of missing values using Missing Variables Analysis (MVA), and Little’s missing completely at random (MCAR) test was used to determine the pattern of missing responses. We included 202 questionnaire items in the analysis, and the results showed that the data were MCAR (χ2 = 36102.501, df = 86,118, p = 1.000). Although MCAR is considered to have minimal effects on estimates and standard errors, we used FIML to include most responders. Because some items were intended to measure religiousness among Christian participants, additional analyses were conducted excluding participants whose religious affiliation was not Christian. The results revealed the same pattern, so we report the overall results here.
Results
Descriptive Statistics and Correlations Between Study Variables by Gender
The sample (n = 528) was distributed relatively evenly across gender with 56% women (Table 1). Women and men were both highly educated with college/university degrees (42% and 44%), most were members of the Church of Norway (79% and 81%), and about one third had long-standing health problems (31% and 27%). No significant differences were found between women and men on age, level of education, religious affiliation, or long-standing health problems, all ps > .05.
Distribution Characteristics (Mean, Standard Deviation, n [%]) Among Women and Men in the Present Sample.

Note. Missing n = 0-19.
Comparisons were made using a two-sided independent-samples t test for the continuous variable (age), and Pearson’s chi-squared tests were used for categorical variables (education, church membership, long-standing health problems).
The level of positive religious experience significantly differed across gender with a lower mean for men than for women (difference: −0.372 scale points, see Table 2). No significant differences were found between women and men on level of church attendance, negative religious experience, or EWB. Bivariate correlations between study variables (Table 3) show that negative religious experience was significantly and inversely associated with EWB for both women and men. Church attendance and positive religious experience were significantly associated with EWB for women but not for men. Significant correlations between church attendance and positive religious experience were similar across gender. The same pattern was found for correlations between church attendance and negative religious experience. Finally, the correlation between positive and negative religious experience was significant for both genders, but stronger correlations were found for men as compared with women.
Descriptives of the Study Variables (Mean [Standard Deviation] and Internal Consistencies) Among Women and Men.

Note. N (for means [SD]a) varies between 264 and 283 for women and 207 and 217 for men.
Calculated in SPSS based on aggregated observed variables.
Calculated in MPlus based on latent means in which women represent the baseline group, N = 515.
Correlation Coefficients for the Study Variables for Women and Men.
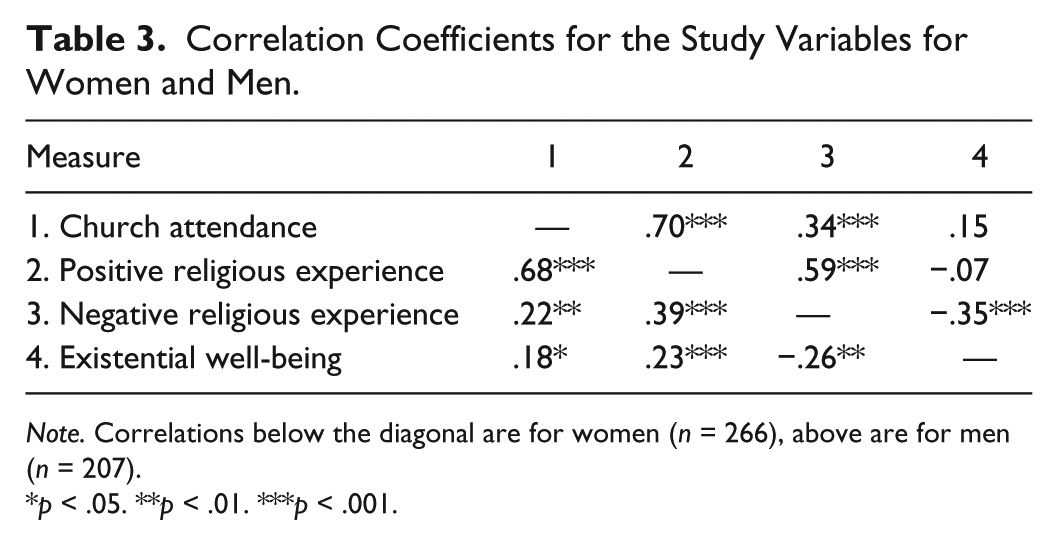
Note. Correlations below the diagonal are for women (n = 266), above are for men (n = 207).
p < .05. **p < .01. ***p < .001.
Measurement Invariance and Model Fit
A prerequisite for testing structural differences in a multiple-group SEM model is to establish measurement invariance across groups in the model. Hence, we compared two confirmatory factor analysis (CFA) models, a constrained model with equal factor loadings across groups, and an unconstrained model in which the factor loadings were freely estimated for each group. The results showed that the constrained model (N = 473), χ2(772) = 1,598.61, p < .05, χ2/df = 2.07, RMSEA = .067, CFI = .882, TLI = .878, BIC = 30,884, had a lower BIC value compared with the less restrictive model (N = 473), χ2(751) = 1,555.17, p < .05, χ2/df = 2.07, RMSEA = .067, CFI = .886, TLI = .878, BIC = 30,970. This indicates that allowing the factor loadings to be freely estimated for women and men did not lead to a better fit in the model as the BIC value increased from 30,884 to 30,970. However, even if measurement invariance could be established, our constrained model did not show adequate fit to the data. Thus, we examined the modification indices to obtain a better understanding of possible sources of poor fit in our model. Consequently, two larger modification indices were examined further. That is, according to the modification index, a correlation between the residuals of REQ Items 10 and 11, and between EWB Items 2 and 6 would consequently cause the largest reduction in chi-square. REQ Items 10 and 11 were placed on a separate page in the questionnaire; Items 1 to 9 were placed at the end of Page 7, while Items 10, 11, and 12 were placed on Page 8. REQ Items 10 and 11 especially concerned an experience of close bonds between the person and God. Both the location of the items in the questionnaire and the common theme of the items could be the cause of the items being more correlated to each other rather than to the latent variable, as predicted by the model. EWB Items 2 and 6 concerned uncertainty about the future, which could be the reason for the correlation between Items 2 and 6. We allowed some item residuals to correlate: REQ Item 10 (pray to God) with Item 11 (fellowship with God), and EWB Item 2 (uncertainty of origin and purpose) with Item 6 (unsettled future). The rerun of the model with the two correlations added resulted in an adequate fit to the data, N = 473; χ2(768) = 1,456.04, p < .05, χ2/df = 1.90, RMSEA = .062, CFI = .902, TLI = .898 (Figure 2).
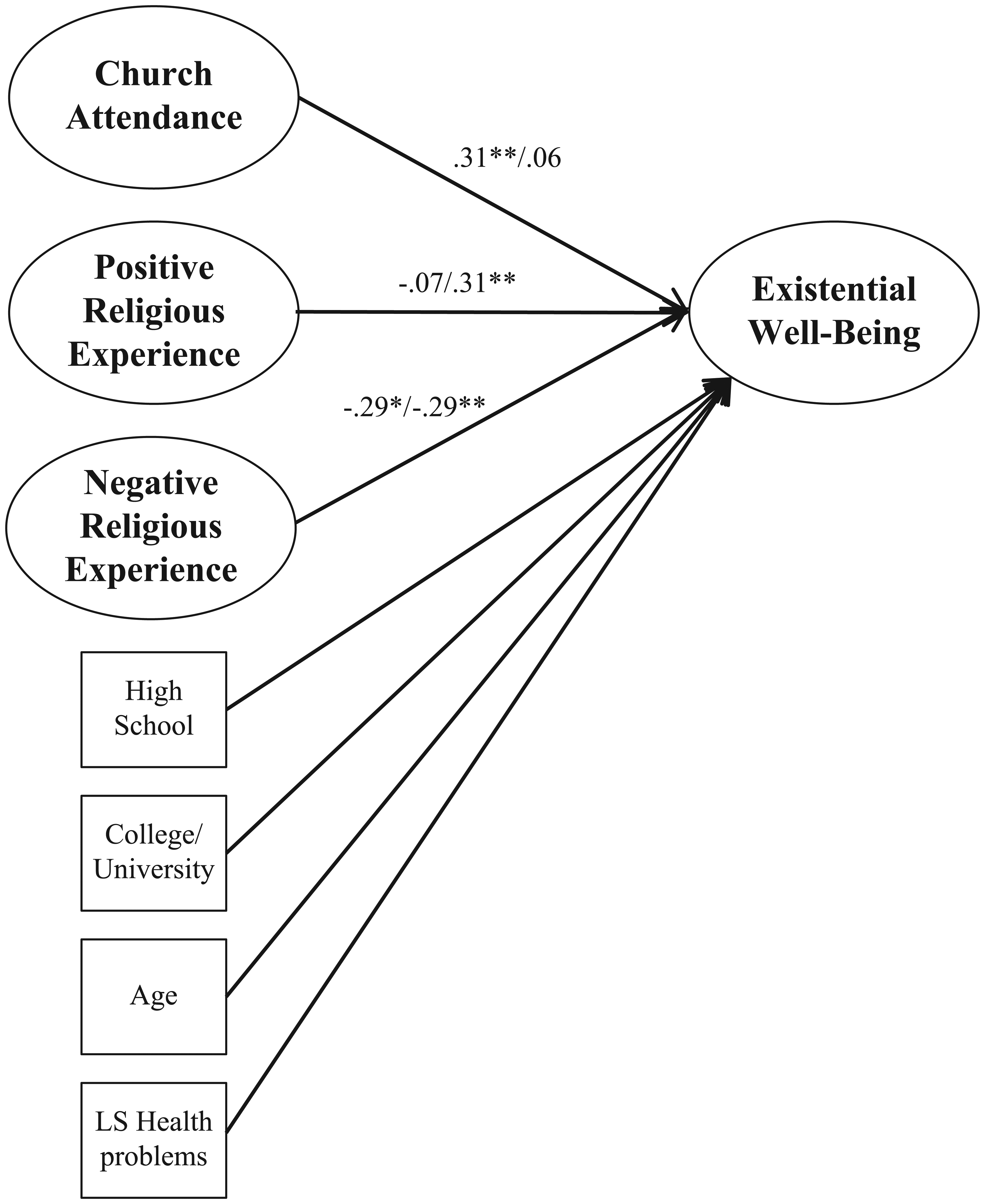
Church attendance, religious experience, and existential well-being: Gender differences controlling for education, age, and long-standing health problems.
Structural Differences of SEM Model Across Gender
To test structural differences between the models for the two genders systematically, a model with the additional constraint of equal structural regression weights was tested against a model that only assumed measurement invariance but allowed all structural regression weights to be estimated freely. Both models showed adequate fit to the data (Table 4). The fit indices were similar, apart from marginal changes in CFI. However, as BIC improved by >10 units from the less constrained to the more constrained model, this indicates that gender does not moderate the structural paths from church attendance, positive religious experience, and negative religious experience to EWB altogether. In other words, a model that assumes equal structural regression paths receives a better overall fit expressed in a lower BIC as compared with a more complex model with individually estimated regression weights for men and women.
Comparing the Fit Indices and BIC for the Unconstrained and Constrained Multiple-Group SEM Models.

Note. N = 473. BIC = Bayesian Information Criterion; RMSEA = root mean square error of approximation; CFI = comparative fit index; TLI = Tucker–Lewis index; SEM = structural equation modeling.
All regression weights (from church attendance, positive experience, and negative experience, to existential well-being) constrained to be equal for women and men.
Nevertheless, for descriptive purposes, the regression paths were examined individually across gender (Figure 2). For women, positive religious experience had a significant positive association to EWB, while negative religious experience had a significant negative association to EWB. No significant relationship was found between level of church attendance and EWB. For men (Figure 2), the level of church attendance had a significant positive relationship with EWB, and negative religious experience had a significant negative association with EWB. No significant association was found between positive religious experience and EWB for men.
Even if the overall model with equality constraints fit the data better, we also specifically examined whether each of the three regression paths significantly differed for women and men, so three separate models were run by means of a Wald test, each placing an equality constraint for each of the three regression paths. The results showed a significantly stronger relationship between positive religious experience and EWB for women than for men, Wald (df = 1) = 4.55, p < .05. No significant differences between women and men were found for the regression path from church attendance, Wald (df = 1) = 2.10, p = .15, or negative religious experience, Wald (df = 1) = 0.14, p = .71, to EWB.
Discussion
The purpose of this study was to examine whether frequency of church attendance and religious experiences were related to EWB differently for women and men, and further to examine differences across contexts when taking into account church attendance. Results from the global test showed that the female model was not significantly different from the male model. The pattern of associations within the models, however, did differ by gender. Among men, EWB was positively related to frequency of church attendance and inversely related to reported negative religious experiences. Among women, EWB was predicted by both positive and negative experiences, but not by frequency of church attendance. The fact that this study found differences in the models for women and men suggests that this is a complex phenomenon; we will discuss this further. Nevertheless, the paucity of studies in a Norwegian context calls for more studies to be conducted.
Active Men and Affective Women—Differential Associations to Well-Being?
Although a great majority of evidence indicates that women are more religious than men (Francis, 1997), this was not consistently supported by the present findings. Women did report positive religious experiences at a higher rate than did men, but women and men attended church equally often and did not differ in the their reports of negative religious experiences. Although questions regarding whether women or men are the most religious may appear unrelated to the main question in this study on the effects of religiousness on well-being, these two questions may be related if one assumes that engagement in religion may be motivated by increased well-being. Increased well-being may be achieved by different means. For men, church attendance was positively, and negative religious experience was negatively, related to EWB, whereas positive religious experiences predicted EWB for women.
The current findings are consistent with a growing body of research. McFarland’s (2010) prospective study showed that men showed more mental health benefits from organizational religious involvement than did women. Research by Maselko and Kubzansky (2006) found that religious attendance and spiritual experiences were related to the well-being of women, but that men’s well-being was more strongly related to weekly religious attendance. More frequent church attendance was related to less depression for men in a Norwegian context (Sørensen, Danbolt, et al., 2012). In a related vein, younger religious men in Norway report higher levels of tangible and emotional support than did women or non-religious men (Kvande, Reidunsdatter, et al., 2015). Our finding that church attendance only influenced well-being for men is, however, not in line with the theoretical perspectives of women’s coping mechanisms being more emotion-focused and seeking others for support. If this were the case, one would expect that both church attendance and religious experiences would benefit women more than men. Nevertheless, attending church frequently may not necessarily increase perceptions of social support, and correlations between church attendance and mental health vary according to religious traditions (Schwadel & Falci, 2012).
The present results may also reflect the active and affective distinction used to describe gender differences in religious involvement (Sullins, 2006). That is, men do not attend church more often than women, but attending church may be more important to men’s well-being. This may be because it extends men’s social networks in a way that offers greater social support than is found in other social contexts. Within the stress-buffering and coping perspective, women seem to experience social support in a wide range of contexts; they include more people in their primary network, they are more satisfied with their networks, and they report a greater benefit from their networks than do men (Fuhrer & Stansfeld, 2002; Walen & Lachman, 2000). From this perspective, church attendance may be an important way to form close ties with others and to extend ones social network; consequently, church attendance becomes especially important for men as a source of social support. Consistent with this notion is research by la Cour (2008), who found that religiousness became more important for Danish men who were hospitalized than for women as they became increasingly ill. Similarly, more frequent church attendance was associated with less depression for men, but not for women, after losing a loved one (Sørensen, Danbolt, et al., 2012). The above studies imply that as the severity of a negative life event increases, religiousness yields more benefits for men than for women. In the present study, we observed the gender differences after controlling for long-standing health problems. Based on these findings, further research is warranted to confirm the apparent benefits of church attendance on well-being in men who face health problems, and to verify that the effects do not extend to women.
In the present study, we found women’s close communion with God or the transcendent (positive religious experiences) to be related to EWB. This finding could be associated with women’s general psychological health in that they more often experience anxiety and depression, and more often use emotion-focused coping strategies than do men (Rosenfield & Mouzon, 2013). Thus, experiencing a meaningful and close relationship with the transcendent may be one way of coping emotionally with adversity. Results from a study of Norwegians found that both spiritually based coping and support from coreligionists were related to EWB (Kvande, Klöckner, et al., 2015).
Based on these findings, it seems likely that men may benefit more from active religiousness in the form of church attendance, and women may benefit more from affective religiousness in the form of positive religious experiences. Nevertheless, as it appears also to involve severity of illness or other stressful life events, further studies should differentiate between such events in addition to gender.
Religion and Differential Benefits to Mental Health Across Gender—Equal Patterns of Associations Across Context?
Although some studies support our findings that church attendance may be more beneficial to men (Krause et al., 2002; Maselko & Kubzansky, 2006; McFarland, 2010; Sørensen, Danbolt, et al., 2012), other studies find church attendance to be more beneficial for women (Hintikka, 2001; Lewis et al., 2011). Reviewing the studies mentioned in this article, we see that most Scandinavian studies (Hvidtjørn et al., 2014; Kvande, Reidunsdatter, et al., 2015; la Cour, 2008; Sørensen, Danbolt, et al., 2012) tend to find that men may experience greater benefit from religion compared with women. One exception, however, is the Finnish study by Hintikka (2001) where church attendance was related to less mental health problems for women, but not men. Despite the deviant findings by Hintikka, and focusing solely on the Norwegian and Danish findings, it seems relevant to consider what may be different in a Scandinavian context where men and not women tend to benefit more from church attendance.
One reason for the divergent findings in the literature may be the measures used in the different studies. The studies by Hintikka (2001) and Lewis et al. (2011) relied on a single item to measure attendance at religious services. In contrast, the studies by McFarland (2010) and Maselko and Kubzansky (2006) measure public religious participation according to several items tapping into both frequency of service attendance and also participation in other activities such as prayer groups, meetings, and bible study groups. The present study used three items to reflect more than merely worship service attendance. Taken as a whole, the studies supporting a stronger relationship between church attendance and well-being or mental health for men have in common that they extend the measure of church attendance beyond that of attending services. This raises the question, could a combination of the different activities in the church be particularly beneficial for men? According to Krause et al. (2002), this may indeed be the case. In a prospective study on church-based emotional support with about 400 U.S. Presbyterian church members, findings revealed that over time, men reported better self-rated health. The authors argued that due to differences in gender socialization, it may be easier for men to experience emotional support with coreligionists compared with others outside the church. Krause et al. also suggest that the often subordinate position of women in the church may be a reason why their emotional support from others in the congregation was related to poorer self-rated health over time, a finding that was also confirmed by Maselko and Kubzansky, who found a positive association between women’s public religious activities and distress.
Based on these findings, activities in the church extending beyond service attendance may enhance men’s well-being more than women’s. Nevertheless, as church attendance measures are sometimes very general, it may be hard to interpret how people understand the item and rate their behavior according to the question. This may be the case in the study by Lewis et al. (2011), which asked participants about attendance at a place of worship. The respondents may report service attendance, other activities, or both. Further studies across a range of cultural contexts are clearly needed to examine whether findings differ according to operationalization of church attendance.
Finally, comparability presents a great challenge in the present study, as very few studies internationally, and none in Norway, have examined the specific constructs of church attendance, religious experiences, and EWB when testing differences across gender. More studies are clearly needed to examine the role of religion and the potentially beneficial effects in the lives of Norwegian women and men.
Strengths and Limitations
The use of general population-based data is an important strength of our study as it may provide information on the prevalence and magnitude of religiousness and health in the Norwegian population. Nevertheless, to generalize from population data, the response rate needs to be as high as possible, thus decreasing the chances of non-response error. A response rate of 22% in the present study may automatically present a threat to its generalizability for the rest of the population. However, as the representation of the population in the data material still seems to be reasonably accurate in terms of age, gender, and level of education, the data may still represent the population. An additional strength of the study is the use of scales compared with single-item measures, which are likely to cover more aspects of the phenomenon. One limitation in the present study is the cross-sectional design, and consequently, no causal inferences can be made from the associations. It is thus impossible to say whether women who experience high levels of EWB tend to have more positive religious experiences, or vice versa. An additional limitation is related to the lack of significant differences in the global test when comparing the female with the male model. Furthermore, although the relationship between church attendance, religious experiences, and EWB showed different patterns for women and men, the only significant difference between women and men was the association between positive religious experiences and EWB. Consequently, our results should be interpreted with caution, and the value of this study is more of a descriptive nature that may guide further research on gender differences. As we know that relationships between religiousness and health are more pronounced among highly religious populations (Diener, Tay, & Myers, 2011), it may be that a population study in a highly secular context will not reflect clear gender differences that would otherwise be found in specific congregations. Further studies and preferably prospective studies should be carried out to test for gender differences in religiousness and well-being across different contexts.
Conclusion
Researchers point to gender differences in the relationship between religiousness and mental health. The present study adds to this literature by finding that church attendance seems to be more important for men’s well-being, but that positive religious experiences are important for women’s well-being. Consequently, our findings support the notion that men benefit more from active religiousness and women more from affective religiousness. Although studies in a Scandinavian context, especially Norway and Denmark, seem to support a greater benefit for religiousness on men’s mental health and well-being, this has not been a consistent finding in other contexts. However, the specific measures used in the studies appear to be an important factor; in studies where church attendance reflects more than merely service attendance, the patterns of gender differences are different from studies that rely on service attendance. Future studies should be prospective in design to examine the causal mechanisms between religiousness and health in general. We also need more studies in a secular context to examine gender differences in religion and health among people suffering from illness, as well as in specific congregations.
Footnotes
Appendix
Confirmatory Factor Analysis of a One-Factor and a Two-Factor Solution of the REQ.
| One-factor model (n = 503) |
Two-factor model (n = 503) |
||||||||
|---|---|---|---|---|---|---|---|---|---|
| Item ← Latent variable | b | SE | β | p | Item ← Latent variable | b | SE | β | p |
| 1. Gods love ← REQ | 1.000 | — | .885 | — | 1. Gods love ← REQ a | 1.000 | — | .890 | — |
| 2. Pray ← REQ | 1.037 | .041 | .839 | <.001 | 2. Pray ← REQ a | 1.032 | .041 | .839 | <.001 |
| 3. Anger ← REQ | 0.218 | .037 | .281 | <.001 | 3. Anger ← REQ b | 1.000 | — | .634 | — |
| 4. Forgiveness ← REQ | 0.972 | .040 | .830 | <.001 | 4. Forgiveness ← REQ a | 0.967 | .039 | .830 | <.001 |
| 5. Punishment ← REQ | 0.261 | .032 | .373 | <.001 | 5. Punishment ← REQ b | 0.895 | .146 | .630 | <.001 |
| 6. Guidance ← REQ | 0.878 | .035 | .837 | <.001 | 6. Guidance ← REQ a | 0.872 | .035 | .836 | <.001 |
| 7. Distance ← REQ | 0.118 | .043 | .133 | .007 | 7. Distance ← REQ b | 0.839 | .122 | .467 | <.001 |
| 8. Closeness ← REQ | 1.094 | .038 | .899 | <.001 | 8. Closeness ← REQ a | 1.094 | .037 | .904 | <.001 |
| 9. Influence ← REQ | 1.187 | .036 | .938 | <.001 | 9. Influence ← REQ a | 1.189 | .035 | .944 | <.001 |
| 10. Close friend ← REQ | 1.133 | .043 | .880 | <.001 | 10. Close friend ← REQ a | 1.093 | .043 | .857 | <.001 |
| 11. Fellowship ← REQ | 1.143 | .042 | .892 | <.001 | 11. Fellowship ← REQ a | 1.101 | .042 | .867 | <.001 |
| 12. Doubt ← REQ | 0.731 | .053 | .587 | <.001 | 12. Doubt ← REQ a | 0.729 | .053 | .588 | <.001 |
| Model fit | One-factor model | Two-factor model | |||||||
| χ2 | 439.668 | 230.806 | |||||||
| df | 54 | 52 | |||||||
| χ2/df | 8.14 | 4.44 | |||||||
| RMSEA [CI] | .119 [.109, .130] | 083 [.072, .094] | |||||||
| CFI | .911 | .959 | |||||||
| TLI | .892 | .948 | |||||||
| BIC | 17518.679 | 17322.258 | |||||||
| ΔBIC | 196.421 | ||||||||
Note. REQ = Religious Experience Questionnaire; RMSEA = residual mean squared error of approximation; CI = confidence interval; CFI = comparative fit index; TLI = Tucker–Lewis index; BIC = Bayesian information criterion.
Positive religious experience.
Negative religious experience.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.