
Abstract
This study examines the prevalence, and the socioeconomic and demographic determinants of under-five mortality in Benue State, Nigeria. Using a purposive random sampling technique, a total of 1,500 questionnaires were administered to women aged 15 to 49 years and who have ever given birth in 30 communities from 10 sampled local government areas in the state. In addition, focus group discussions and key informant interviews formed sources of data for this research. The analysis of data was carried out using descriptive statistics, child survival analysis, and probit regression model. The pattern of the prevalence of infant and child mortality showed that there are three major child killers in the study area: malaria (38.2%), complications at birth (29.5%), and measles (16.9%). The survival probability results show that children born to parents living in an urban area have more chances (72.6%) of survival, as against 71.4% for children born to parents living in a rural area. The probit regression analysis showed that the pregnancies ever had by the mothers has a greater marginal effect on child survival (6.7%) than the current age of mothers at birth (3.7%) and the age of mother at marriage (0.9%). Based on the findings, recommendations such as empowerment and education of mothers are suggested.
Introduction
It has been estimated that the under-five (U5) mortality rate worldwide declined by 30% between 1990 and 2007 with children’s survival chances increasing in 95% of countries (Overseas Development Institute, 2010; World Health Organization [WHO], 2012). However, early childhood mortality varies among world regions and over time, and the differences are large and increasing. In the highly developed economies, with advanced medical technologies, sufficient diets, and adequate public sanitation, the U5 mortality rates tend to be quite low (below 5 per 1,000). In contrast, within the less developed countries, with the disadvantages of poor diet, limited access to medical technology, and other problems of poverty and public sanitation, the rates tend to be as high as over 100 per 1,000. Among major world regions, the rate is highest in Africa and Asia, while the lowest rates are in North America and Western and Northern European countries (Garry & Larkin, 1989; United Nations, 1998; United Nations Development Programme [UNDP], 2005; WHO, 2010). In addition to this spatial pattern, the differences between regional mortality figures are not only large but also increasing over time (Cleland & Kaufmann, 1993). In 1990, for instance, there were 180 per 1,000 live births in sub-Saharan Africa and only 9 per 1,000 in the industrialized countries—a 20-fold difference. In 2006, this gap had increased to 31-fold with mortality rates of 186 and 6 per 1,000 children in sub-Saharan Africa and industrialized countries, respectively (United Nations Children’s Fund [UNICEF], 2001, 2008).
Progress in child survival remains unacceptable in most developing countries in sub-Saharan Africa where infant and child mortality continues to be higher than in other developing countries of the world (Legrand & Mbacke, 1995; Odubanjo & Olumide, 2007; Salau, Galpin, & Odimegwu, 2006). While sub-Saharan Africa constitutes about 10% of the world population and 23% of the world’s births, the region accounts for more than 40% of the world infant and child mortality, 70% of the world’s people with HIV/AIDS, 80% of AIDS deaths, and 90% of AIDS orphans (Annan, 2001; UNICEF, 2001; WHO, 2005). Of 20 countries in the world identified as having high U5 mortality, 19 are in sub-Saharan Africa. Similarly, of the world’s 20 countries with the highest risk of neonatal deaths, 15 are in Africa (World Bank, 1987; WHO, 2008), and of about 60 countries that are currently off the tract from achieving the Millennium Development Goal–4 (MDG-4; the reduction of child mortality by two thirds by 2015), 40 are African countries (UNICEF, 2008).
Data from the Countdown to 2015, 2011 Report indicated that of the 7.6 million U5 child deaths in 2010, 82% of them occurred in sub-Saharan Africa and South East Asia. In addition, 50% of the U5 deaths in that year occurred in five countries: India, Nigeria, Democratic Republic of the Congo, Pakistan, and China, with India (22%) and Nigeria (11%) together accounting for a third of the total number of U5 deaths worldwide (WHO/UNICEF, 2012). The high risk for U5 deaths in Nigeria is further demonstrated by the fact that in 2010, Nigeria’s U5 deaths to total live births ratio stood at 13.6% (annual number of births and deaths of U5 in thousands were 6,332 and 861, respectively, as in 2010) as against the global and Indian figures of 5.6% and 6.2%, respectively. Indeed, Nigeria, which accounts for about 2.3% of the global population, bore a proportionally higher U5 death burden than even India, which houses 17.9% of the world population (Nte, 2012). Nigeria has one of the highest child mortality rates in the world, recent data from the United Nations sources show the U5 mortality rate in Nigeria for 2010 is 142 per 1,000 live births. Infant mortality rate is 88 per 1,000 live births, and neonatal mortality rate, 40 per 1,000 live births, with a concurrent increase in the number of live births. The low rate of decline is a major cause for concern. With this current rate, Nigeria is not on track in meeting UN MDG’s expected rate of 4.5% annual decline, to reach a target of 64 per 1,000 live births in 2015, which is a few months away.
These are aggregate values, but most importantly, infant and child mortality rates in Nigeria vary spatially among the geopolitical zones of the country and between rural and urban residence. The values include Northeast (222 per 1,000 live births), which recorded the highest U5 mortality rate; the Northwest (217 per 1,000 live births) ; and the Southwest (89 per 1,000 live births), which has the lowest rate among the geopolitical zones. U5 mortality was higher in the rural areas with a rate of 191 per 1,000 live births as against the 121 deaths per 1,000 live births in the urban areas. One of the striking features of the mortality pattern is the consistently high mortality rates in the northern part of Nigeria (Aigbe & Zamu, 2012; National Population Commission [NPC], 2009). Most of such studies on the patterns and determinants of early childhood mortality in Nigeria have been at aggregate levels geopolitical zones while neglecting the critical influence of community-level variables and small area variations (Salau et al., 2006). In Nigeria, for instance, studies on mortality among children were conducted in eastern and south western parts of the country using secondary data, but the results were used to make generalizations in respect of childhood mortality for the nation as a whole. Such studies, among others, include Lawoyin (2001); Antai, Ghilagaber, Wedren, Macassa, and Moradi (2009); Folake, Abiodun, and Wilna (2008); Ogbe (2008); Uthman (2008); Ojikutu (2008, 2010); and Mesike and Mojekwu (2012). Such generalizations, according to Premananda et al. (2004) and Overseas Development Institute (2010), can be misleading as there is ample evidence that infant and child mortality tends to follow contours of social and economic progress across and within communities in the country.
It becomes imperative, therefore, for researches on the prevalence and determinants of early childhood mortality to be conducted using community-level and small area variation data (Salau et al., 2006). Such research will help in the design and implementation of policies and interventions to lower disparities and achieve mortality decline nationwide. It is on this premise that such a community-level study is important in Benue State where dearth of studies on prevalence and determinants of U5 mortality exist.
Materials and Method
The Study Area
The study area, Benue State, lies between latitudes 6°30′ and 8°10′N of the Equator and between longitudes 7°50′ and 10°E′ of the Greenwich Meridian. It is surrounded by six states, namely, Nassarawa to the north, Taraba to the northeast, Cross River and Ebonyi to the south, Enugu to the southwest, and Kogi to the west. There is also a short international boundary between the state and the Republic of Cameroun along Nigeria’s southeast border. Benue State is made up of 23 local government areas (LGAs); 14 and 9 of these LGAs correspond with the ethnic territory of the Tiv and Idoma people, respectively. Figure 1 shows the 23 LGAs that make up the state.

Map of Benue State, Nigeria (ministry of lands and survey, Makurdi).
With a population figure of more than four million inhabitants (4,253,641), the state is the ninth most populous state in Nigeria. Made up of 2,144,043 males and 2,109,598 females, the state has a sex ratio of 1.02, a literacy rate of 44.7% among the population aged 6 years and above, and a population density of about 130 persons per square kilometer (Federal Republic of Nigeria, 2009; NPC, 2009). There are three major ethnic groups inhabiting the state. The Tiv form about two thirds of the population and are found in 14 of the 23 LGAs. The Idomas and the Igedes occupy the remaining 9 LGAs. Other ethnic groups include the Etulo, who are mainly found in Katsina Ala and Buruku LGAs, the Afia in Ado, the Nyifon in Buruku, and the Jukuns in Makurdi and Guma LGAs.
Theoretical Framework
This study is based on the model of the factors of infant and child mortality developed by Mosley and Chen (1984) and modified by Casterline, Cooksey, and Ismail (1989) and Bryman and Cramer (1990). This model assumes that death is the final biological expression of a process that is determined basically by the economic, demographic, and social structure of any area. These determinants of infant and child mortality, which this study examined according to the model categories by Mosley and Chen, are as follows: (a) the socioeconomic characteristics such as mother’s education, occupation, residence, resources of the household, income of the mother, and medical care; (b) the intervening or housing conditions or environmental variables such as source of water, toilet facilities, and distance from home to the nearest health facility; and (c) the demographic variables such as age of mother at childbirth, birth order, previous birth interval, breastfeeding, and sex of the child. This study therefore uses the model by Mosley and Chen to appraise how these socioeconomic and demographic factors influence childhood mortality in Benue State, Nigeria.
The Selection of Sample Population
In the selection of the sample population, the following steps were adopted. First, Makurdi LGA, the LGA that houses the seat of administration and power in the state, was purposively selected. Thereafter, using simple random sampling, three LGAs were selected from each of the three geopolitical zones in the state, thereby giving each of the LGAs in each of the geopolitical zones in the state an equal opportunity of being selected for the study. From the 10 LGAs so selected, three communities were randomly selected for the study, giving a total of 30 communities. Finally, from each of the 30 communities selected for the study, 50 women aged 15 to 49 (the prime reproductive cohort of the population) who had ever married and who had given birth at least once in the past 5 years preceding the survey, irrespective of place and outcome of delivery, and who are residents (at least 1 year) of such communities were, also, randomly selected, ensuring a fair spread of the respondents across the communities. This gave the study population of 1,500 respondents. Of the 10 study LGAs, 3 of them are better disposed in terms of health facilities, educational institutions, government offices, daily marketing, and transportation systems, and they are regarded as urban LGAs, while the others are rural LGAs. The three urban LGAs are Makurdi, Otukpo, and Katsina Ala. The sampled LGAs and the list of the sampled communities for the study are presented in Table 1.
List of LGAs and Sampled Communities.

Note. LGA = local government area.
Data Collection
The data for this study were generated using primary and secondary sources. The primary source of data was through questionnaire administration while the secondary sources were books, journals, official documents, conferences, and seminal papers. Copies of the questionnaire were administered to the 1,500 women aged 15 to 49. The distribution and retrieval rate of the questionnaire is shown in Table 2.
Distribution and Retrieval of Study Questionnaire.

Note. LGA = local government area.
Based on the sensitivity and peculiarities of the items in the questionnaire and the need to give the respondents a level of confidentiality during the interview, trained female research assistants (known within the communities), comprising teachers in the primary schools and female health workers within the communities, were used as research assistants in data collection. The health officers were assigned to supervise the data collection process in each of the sampled LGAs and a coordinator oversees the process in each of the senatorial districts. The need for the research assistants to understand the local dialects of the communities was stressed as interpreters were not only likely to increase the bill of data collection but also more likely to cause the loss of vital information due to wrong interpretation and due to the respondents’ unwillingness to release vital personal information to a crowd. The issue of understanding the local dialects of the communities becomes important as adjoining communities in the same LGA in the state may not understand each other (a peculiarity of the Middle Belt Region that houses about 75% of the ethnic groups in Nigeria).
Data Analyses
Descriptive statistics as means, percentages, maps, and charts were used to describe the incidence and pattern of childhood mortality in the study area. In addition to these statistical tools, the Child Survival Probability Model was used to calculate the chances of child survival and dying. These probabilities were calculated using the following equations as outlined by Rajaratnam (2003):

where CEB represents the number of children ever born by women in group i, and FP i is the female population in group i; and

where D i is the proportion dead among children ever born to women in group i, and CD i represents the total number of children dead to women in group i.
Converting the proportion of children ever born who have died into a probability of dying gives

and

where qx is the probability of dying among children ever born and Lx is the probability of survival among children ever born.
In addition, the probit regression model was also used not only to bring out the strength of each of the independent variables (regression coefficient) on the dependent variable (infant and child mortality) but also to highlight the impact on the dependent variable (marginal probability effect) of the slightest change in any of the independent variables. The probit regression model, though similar to the multiple regression, has an advantage over the latter because of its inbuilt mechanism to bring out the marginal probability effect of each of the independent variables over the dependent variable.
According to Albert (2007) and Kim (2010), the model equation is as follows:

where Y represents the dependent variable (infant and child mortality), b0 is the intercept (constant) that scales the equation, b1, . . . bn represent the regression coefficients, X1 to Xn stand for the independent variables (socioeconomic variables, maternal reproductive-related factors, and health seeking behavior of the parents), and e represents the error term.
Results and Discussion
Age Differentials of Infant and Child Mortality
The results show that the age at which a child dies in the study area varies from one LGA to the other (inter-LGA variation). The inter-LGA variations presented in Table 3 show the proportionate contribution of each LGA to the overall child death in the study area with Otukpo, Ado, and Katsina Ala (in that order) leading the other LGAs in terms of perinatal deaths; Vandeikya, Otukpo, Agatu, and Ado recorded higher statistics of neonatal mortality. The postneonatal mortality figures are higher in such LGAs as Agatu, Otukpo, and Gwer East while Makurdi, Guma, and Agatu recorded the worst child death statistics in the study area. The explanation for this observed pattern hinges on the availability and accessibility as well as the readiness on the part of the caregivers to patronize the facilities. Furthermore, the referral role played by such LGAs as Makurdi, Otukpo, and Katsina Ala in their respective zones may partly explain the observed pattern as the process of death, which might have originated in the rural LGAs and might have ended up in these urban LGAs.
Age Distribution of Infant and Child Mortality in the Study Area (%).

Note. LGA = local government area.
Pattern of Infant and Child Mortality by Causes of Death
The chances of child survival depend, among others, on the prevailing health challenges in the study area. The major causes of child death in the study area include birth complications, malaria, diarrhea, measles, HIV/AIDS (through mother to child transmission), tetanus, and tuberculosis. The prevalence of these challenges varies not only across the study area but also across the childhood ages as shown on Table 4.
Causes of Infant and Child Death in the Study Area (%).

Note. LGA = local government area; TB = tuberculosis.
The prevalence of birth complications is outstanding in such rural LGAs as Ado, Gwer East, Logo, and Vandeikya and in the urban LGA of Katsina Ala. Lack of health care services for mothers during pregnancy and birth or the low utilization of such services even when available, poor hygiene, and little understanding of newborn care are the likely issues responsible for this challenge in the study area. Malaria, an infectious disease transmitted by female mosquitoes, remains a major health problem in the study area as it runs through the study area with Otukpo and Agatu LGAs having the highest prevalence rate. The antimalarial initiative of the government needs to be given more serious attention in the study area. Also, measles, usually spread by contact with nasal or throat secretions of those infected, is also present in all the LGAs with its effects more intense in such LGAs as Guma, Tarka, and Agatu. Diarrhea is caused by the presence of parasites in food and water. Children succumb to such parasites more quickly than adults because of their weak responsive immune system. Diarrhea thrives in conditions of poor diet, poor hygiene, and contaminated water. This child killer is seen in all the LGAs with very serious cases noted in Ado, Guma, Vandeikya, Makurdi, and Tarka LGAs. In the study area also, HIV/AIDS is usually contacted by babies from their mothers during pregnancy, birth, or breastfeeding, while some were exposed to contaminated needles or blood. Subsequently, Benue State has the highest HIV/AIDS prevalence in the country, which stands at 12.5% and 13.3% in the urban and rural areas, respectively (Federal Ministry of Health [FMOH], 2005). Among the LGAs in the study area where the HIV/AIDS prevalence is notable are Tarka, Otukpo, Vandeikya, Ado, and Agatu. The prevalence of tuberculosis and tetanus in the study area, compared with killer diseases in the study area, is minimal because of the antenatal and child immunization services. However, substantial cases of tuberculosis are noted in Logo, Ado, Katsina Ala, and Gwer East, while tetanus featured more in Ado, Otukpo, and Vandeikya LGAs.
Apart from the variation in the prevalence of these causes of early childhood death across the study area, the age of the child at death also varies with the causes of death because of the age-specific nature of the causes. For instance, as shown in Table 5, birth complications and pediatric HIV/AIDS are prominent with the perinatal age; tetanus is noted at the neonatal and perinatal stages, while diarrhea, malaria, and measles are challenges faced at the postneonatal and child stages. On the whole, malaria, measles, complications at birth, and diarrhea (in that order) are the leading causes of U5 deaths in the study area. The knowledge of the pattern of prevalence of these childhood health challenges in the study area is of great importance to health policy formulators.
Pattern of Infant and Child Mortality Based on the Causes of Death (%).

The impact of these death causes on the different LGAs in the study area as reported by our respondents is shown in Table 4. The influence of these causes varies among the LGAs depending on the level of health infrastructural development. The table shows greater infant deaths through birth complications, HIV/AIDS (through mother–child transmission), and tetanus. However, the older children die more than the infants through diarrhea, malaria, measles, and tuberculosis. Invariably, the infants are greater victims of these causes of death (because of the lower immune system) than the older children across the LGAs except in Guma and Makurdi LGAs, with Guma LGA recording the sharpest difference between the two categories of childhood deaths while the urban LGAs recorded lower childhood deaths than the rural communities across the study area.
Pattern of Child Survival Probability Status in the Study Area
From the discussions on the spatial patterns of infant and child mortality in the study area, it is evident that the survival probability status of the child varies from one LGA to the other, depending, among others, on the age dispensation of the child and that of the mothers, the rural–urban residence status, the prevalence of the causes of childhood death, and the availability or otherwise of facilities to address the health challenges of both the child and that of their mothers. The child survival probability across the LGAs is shown in Table 6.
Probability of Child Survival in the LGAs Across the Study Area.

Note. LGA = local government area; CEB = children ever born; CED = children ever dead; M = male; F = female; T = total.
The table shows that Agatu, Makurdi, and Ado (in that order) recorded the highest childbirths among the LGAs in the study area. This may not be unconnected with the fact that these three LGAs are part of the senatorial district noted in the past for the highest HIV/AIDS prevalence not only in the state but also nationwide. Furthermore, the prevalence of malaria and measles among the three LGAs may also contribute to their position in terms of child deaths among the LGAs.
The probability of a child dying is highest in Ado, Otukpo, and Agatu LGAs. These LGAs, by implication, experience the lowest probability of child survival in the study area. Two of the LGAs (Otukpo and Agatu), for instance, top all the others in malaria prevalence. Makurdi LGA recorded the highest probability of child survival among the LGAs of study for obvious reasons of being the LGA that houses the seat of state administration as well as the LGA with the best network of health and other social amenities. On the whole, the female child has a higher probability of survival than her male counterpart. The results also show that a child born to parents living in the urban LGAs, on the average, has a higher survival probability (72.6%) than his or her counterparts whose parents reside in the rural LGAs (71.4%). This is because of the preponderance of child survival programs in the urban rather than in the rural LGAs. Quite a number of child deaths in the urban LGAs were actually from the rural LGAs in attempts by rural parents taking advantage of the referral health facilities in the urban areas.
Probit Regression Analysis of the Determinants of Infant and Child Mortality in the Study Area
In an attempt to bring out the list of the most influential determinants of early childhood mortality, their strength and marginal effect on the incidence of infant and child mortality in the study area, all the independent variables (maternal reproductive-related variables, socioeconomic, and the health seeking behavior of the parents) were subjected to the probit regression analysis. The result of the analysis, presented in Table 7, showed the list of independent variables considered to be of greater relevance to the incidence of child survival in the study area. This result has an adjusted R2 value of .433 implying that 43.3% of the variance in infant and child mortality in the study area is explained by the model. Among the maternal reproductive-related variables, the age of the mothers, the age at marriage, and the number of pregnancies ever had were considered more relevant by the model than the other considerations within the group as the other factors, more or less, depend on these three. The level of education of the mothers, the paternal employment status, the size of the households, the type of living houses, and the locality of residence of parents featured so prominently among the socioeconomic factors while the variables from the health seeking behavior of the parents include visit to the antenatal clinic, ownership of the facilities patronized during pregnancy as antenatal clinic, the length of breastfeeding by the mothers, and the immunization status of the child. The values of the probit regression coefficients suggest that infant immunization (.991), pregnancies ever had by the mothers (.520), and their locality of residence (.332) are more critical to predicting the incidence of infant and child mortality in the study area than the other variables.
Probit Regression Analysis of the Determinants of U5 Mortality in the Study Area.
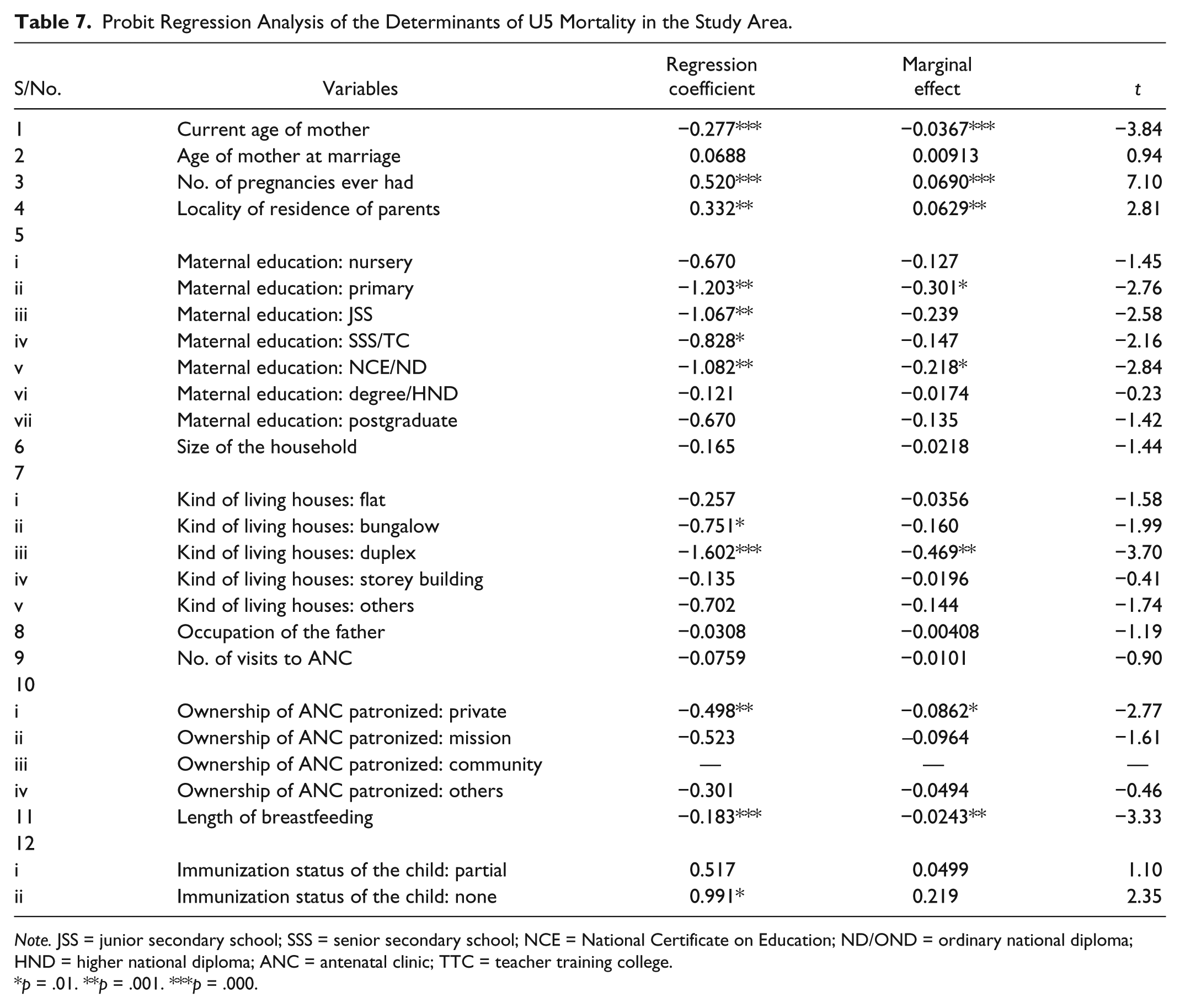
Note. JSS = junior secondary school; SSS = senior secondary school; NCE = National Certificate on Education; ND/OND = ordinary national diploma; HND = higher national diploma; ANC = antenatal clinic; TTC = teacher training college.
p = .01. **p = .001. ***p = .000.
However, the marginal probability effect of the independent variables on the incidence of early childhood mortality is greater for such variables as living houses (46.9%) and maternal educational groups (30.1%) than that for the other variables. This implies that aggressive policies on housing and female child education will go a long way to enhancing the child survival status in the study area.
The regression results in Table 6 also shows that with reference to mothers aged 15 to 19, a unit increase in the age of the mothers, all things being equal, results in a corresponding decrease of the probability of a child dying by about 3.7%. Conversely, a unit reduction in the age of the mothers, all things being equal, amounts to a corresponding reduction of the probability of a child surviving by the same percentage. The negative implication of teenage pregnancy and childbirth is thus so highlighted. The number of pregnancies ever had by a mother is a factor of child survival as every additional pregnancy increases the child’s nonsurvival probability by about 6.9%. This has to do with the continual weakness of the womb of the mother with increasing number of pregnancies.
The importance of maternal education to the survival of the child is also demonstrated by the table. With reference to illiterate mothers, a unit of additional educational attainment of nursery, all things being equal, yields a 12.7% decrease in the probability of a child dying. Similarly, an attainment of senior secondary school or teacher training college (SSS/TTC) from junior secondary school (JSS) yields an even greater decrease by 14.7% of the probability of a child dying. The occupation of the father, rather than that of the mother, is considered significant by the model. The likely explanation for this scenario in the study area is the unwillingness of mothers to spend on the child without resorting to the husbands. Babies born to employed fathers experienced an enhanced survival of 4.08% over their counterparts born to the unemployed fathers.
The locality of residence of the parents showed that the incidence of infant and child mortality is 6.3% higher in the rural communities than in the urban LGAs. In terms of the health seeking behavior of the parents, particularly that of the mothers, the importance of antenatal visit and its frequency during the gestational period is obvious. The inverse relationship between such visits and the survival of the pregnancy outcome indicates that the more consistent and regular are the visits to the clinic for check-up during pregnancy, the better the likelihood of a healthy outcome. The consistent and regular visits to the antenatal clinics by the pregnant mothers reduce the probability of child dying by 10%. The ownership of such antenatal clinics is considered to be of relevance to a successful pregnancy outcome. With reference to the government-owned clinics, the mothers who made use of private clinics, mission hospitals, and “other” health centers recorded, respectively, higher probabilities of 8.6%, 9.6%, and 4.9% of child dying than the probability recorded by mothers who attended government clinics. The quality of services rendered by the government-owned facilities is much better than that provided by these profit- (or philanthropic)-oriented clinics in the study area.
The protection offered the child by immunization is also acknowledged by the model as children who received no immunization compared with those who received full dosage of immunization have 21.9% higher probability of dying. The importance of breastfeeding as the most nutritious diet of the baby during the formative age is stressed by the model. Babies who are fed with breast milk exclusively for the first 6 months of life and extended to a period of 18 months and above are likely to thrive more than those put on breast milk for a period shorter than 6 months for whatever reasons advanced by the mothers. Such babies in the latter category experience 2.4% higher probability of dying compared with counterparts who are on breast milk for more than a year and half.
Summary of Findings and Recommendation
The incidence of early childhood mortality in the study area showed variations from one LGA to another. The proportional contribution of the U5 deaths among the LGAs indicated that the LGAs in the Benue South senatorial district are worse off than the cases in Benue North and Benue Central senatorial districts. The pattern of the prevalence of the causes of infant and child mortality showed that there are three major child killers in the study area: malaria (38.2%), complications at birth (29.5%), and measles (16.9%). A focus on these three health challenges that account for over three quarters of early childhood deaths in the study area should be the parental cry of the moment in the state. The survival probability results show that children born to parents living in an urban area have more chances of survival, 72.6% as against 71.4% for children born to parents living in a rural area. Furthermore, the probit regression analysis of these maternal variables showed that the pregnancies ever had by the mothers has a greater marginal effect on child survival (6.7%) than the current age of mothers at birth (3.7%) and the age of mother at marriage (0.9%). In the light of the findings of the study, it is recommended that measures should be taken to promote the fulfillment of girls’ and mothers’ potentials not only through education but also through skills development and the eradication of illiteracy for all girls and women without discrimination of any kind. Mothers should also be educated on the need to engage in exclusive breastfeeding of their babies to help make the immune systems of these babies stronger. Governments and parents should also ensure that the children receive full and appropriate immunization for child killer diseases. Finally, the parents should be educated on the need to stop marrying of their daughters at very young ages as such young women may be susceptible to delivery complications that can adversely affect health of the child.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.