
Abstract
We analyze infant and under-5 mortality trends in Nigeria using data from the demographic and health surveys (DHS) of 2003 and 2008. We use pooled data to enable us carry out logistic regression analysis at the state level and allow for robustness of our results. Our analysis shows wide disparities in both infant and under-5 mortality rates in the six geopolitical zones of Nigeria and the 36 states and the Federal Capital Territory Abuja. Furthermore, the results show highly significant differences in infant and under-5 mortality rates among the six geopolitical zones and among the 36 states of Nigeria. Our result shows that urban advantage over rural areas in under-5 mortality rate only exist among the richest quintiles in Nigeria. We find no evidence of statistically significant difference between the urban poorest and poorer quintiles and the rural poorest and poorer quintiles in both infant and under-5 mortality in Nigeria. We find wealth, educational attainment of the mother, the use of health facility, religion, gender of a child, and number of births in the last 3 years to be highly correlated with infant and under-5 mortality in Nigeria. Both infant and under-5 mortality rates declined between 2003 and 2008 in Nigeria.
Introduction
There is no doubt that the increase in life expectancy in Nigeria from 47 in the 1990s to 52 today is largely from the reduction in infant and under-5 mortality over the same period. Cutler, Deaton, and Lleras-Muney (2006) argued that falling mortality has also meant better health for the living, so that people are also living better, healthier, and longer lives than did their forebears. Their study noted that cross-country evidence does not suggest economic growth will improve health without deliberate public action. Akachi and Canning (2010) argued that in addition to the direct welfare gains from improved health, healthier workers tend to be more productive. Currie (2009) argued that health in childhood affects human capital accumulation and health and labor market status in adulthood. Apouey and Geoffard (2013) found housing conditions, nutrition, and clothing to have large independent effect on child general health. Past studies have found strong association between mothers’ educational attainment and reduction in infant and child mortality (Caldwell, 1979; Kabagenyi & Rutaremwa, 2013; Mosley & Chen, 1984). Cutler et al. (2006) argued that there is a positive relationship between income and health within countries: low-income people live shorter lives than high-income people in a given country. They suggested that health inequalities, also known as gradients, are part of a wider pattern that relates mortality to measures of socio-economic status. They called for further studies on the decline in mortality over time, differences in mortality across countries, and differences in mortality across groups within countries.
Akachi and Canning (2010) argued that the decline in infant mortality in sub-Saharan Africa may have resulted from medical intervention measures and broad-based reductions in exposure to infectious diseases that prevent infant deaths rather than improved nutrition and childhood morbidity. Antai (2010) argued that the rich geographical, cultural, ethnic, and socio-economic diversity of Nigeria implies that immunization uptake varies between and within geographical regions. The study further posits that these differences may result in some segment of children not vaccinated and thus expose the rest of the population to major outbreaks of vaccine preventable diseases. United Nations Children’s Fund (UNICEF; 2009) reports that west and central Africa region has the highest regional under-5 mortality rate in the world. The report showed that under-5 mortality for west and central Africa was 186 per 1,000 live births compared with 160 per 1,000 for sub-Saharan Africa as a whole and 131 per 1,000 for eastern and southern Africa. The literature on infant and child mortality rate is robust for developed countries. Houweling and Kunst (2010) noted that it is only recently that research in inequalities is being studied more systematically in relation to low- and middle-income countries (LMICs). One of the key findings in The National Population Commission (NPC & ICF Macro, 2009) study showed a wide disparity in under-5 mortality within Nigeria. The difference between the south-west zone and north-east zone is 2.5 times, 89 deaths per 1,000 live births in south-west zone and 222 deaths per 1,000 live births in north-east zone. Adedini, Odimegwu, Imasiku, Ononokpono, and Ibisomi (2013) argued that residence in a particular region of Nigeria is a major determinant of infant and child mortality in the country. Antai (2011) found that the risk of under-5 deaths were almost twofold higher for children of mothers residing in the north-east and south-south regions compared with children of mothers in the south-west region.
However, very few studies have focused on the regional differences in Nigeria with specific emphasis on the role of wealth and maternal educational attainment in explaining disparities on infant and child mortality rate. This article, therefore, helps to fill the void that currently exists in the literature by using the demographic and health surveys (DHS) data to examine the impact of wealth, education, beliefs, and location on infant and child mortality rates in the six geopolitical regions of Nigeria. It is evident from the relevant literature above that there is a strong need for an empirical investigation of the source of disparities in infant and child mortality in Nigeria. In Nigeria, most of the decreases in infant and child mortality occurred among the rich just as most of the gains in infant and child mortality took place among the rich developed countries of the world (UNICEF, 2012). Nigeria is one of the least successful countries in Africa in achieving improvements in child survival over the past four decades (Ngowu, Larson, & Kim, 2008). Several public health policies have been under taken at various points in Nigeria. However, the complex nature of the proximate determinants of under-5 and infant mortality has made it difficult to ascertain the exact effectiveness of these policies.
Previous studies identified location as highly correlated with both under-5 and infant mortality in sub-Saharan Africa. The urban–rural difference in under-5 and infant mortality has been documented in sub-Sahara Africa (SSA) (Anyamele, 2009; Cai & Chongsuvivatwong, 2006; Cleland, Bicego, & Fegan, 1992; Fotso, 2006; Knobel, Yang, & Ho, 1994; Kuate-Defo & Diallo, 2002; Lalou & LeGrand, 1997). Given the diverse geographical and cultural nature of Nigeria, we propose to study the differences in infant and under-5 mortality among the six geopolitical zones as well as the 36 states and the Federal Capital Territory Abuja. Given the above backdrop, we test the hypothesis that disparity in infant and under-5 mortality rates in the six geopolitical zones and the different states is correlated with mothers’ educational attainment, wealth, and location.
Understanding these differences if any will enable policy makers and practitioners to design programs that will effectively address the high levels of infant and under-5 mortality rates that are prevalent in Nigeria. To achieve this, we use pooled 2003 and 2008 DHS data for Nigeria. Pooling the data gives us enough data points at the state level for the robustness of the result and generalization from the results. This study marks the first time that infant and under-5 mortality has been studied at state level in Nigeria, thus contributing to our understanding of the differences in infant and under-5 mortality in Nigeria. Past studies have found strong association between poverty and infant and child mortality (see Anyamele, 2011; Cleland et al., 1992; Fotso, 2006; Hong, 2006; McMichael, 2000; Todd, 1996; Victora, Bryce, Fontaine, & Monasch, 2000; Victora et al., 2003; Wagstaff, 2000). Houweling and Kunst (2010) concluded that child mortality is systematically and considerably higher among lower socio-economic groups within countries.
Methods
The analyses were done on Stata 13.1 (2013). The complex nature of the survey design of DHS data meant that we apply the sampling weights to correct for the bias in probability selection. Logistic regression analysis technique is used to examine the effect of wealth quintiles, educational attainment, geopolitical zones, states, the use of health facilities, and urban and rural areas on the probability of infant and child mortality in Nigeria. Using logistic regression technique, we are able to obtain the odds ratio of which group has lower or higher odds of infant and child mortality in Nigeria. The DHS data used in this study are the children’s file data.
The model is given by a linear probability model (LPM) measure of a household experiencing infant or child mortality. If the household has lost a child before or at the 59th month, child mortality Y = 1, otherwise, Y = 0. If the household has lost a child before or at the 12th month, infant Y = 1, otherwise, Y = 0.

Y is a binary variable that takes the values of 1 or 0.

Logistic regression with multiple predictor variables is well suited for this study. Each of the β coefficient estimated is a measure of the expected change in the log odds of a household experiencing infant or child mortality for a unit increase in the corresponding predictor variable holding the other predictor variables constant at certain value. The theoretical framework of our article is based on the work of Mosley and Chen (1984) which suggested combining social science and medical science approaches to study child survival in developing countries. We make no attempt to distinguish between proximate and distal variables in this study.
Data
The sample size for this study is 34,676 households from 2003 and 2008 DHS survey of Nigeria. Our data is made up of 886 primary survey units (PSU). The rural population is made up 71.9% (24,945/34,676) of the sample while 28.1% (9,731/34,676) of the sample is from urban households. 2003 DHS data constitute 17.35% while 82.65% of the sample is from the 2008 DHS data. The zonal composition of the data shows that 17.48% (6,061/34,676) came from the north-central region of Nigeria, 23.20% (8,046/34,676) came from the north-east region, 28.17% (9,768/34,676) is from north-west region, 8.58% (2,974/34,676) of the sample is from south-east region, 11.21% (3,887/34,676) of the sample is from the south-south region, and 11.36% (3,940/34,676) of the sample is from the south-west region of Nigeria. This study utilized 2003 and 2008 DHS pooled data of Nigeria. DHS selected participants for the study through probability sampling procedures. Pooling data from different surveys requires that we account for the differences in survey years and regions. This is achieved by creating a strata identification using year and region as the stratification factor. DHS selected participants for the study through probability sampling procedures. It separated urban and rural strata to provide valid samples of urban and rural populations at the national level.
The DHS surveys were conducted in single rounds with two main survey instruments: household schedule and individual questionnaire for women of reproductive age 15 to 49 years. Whereas the household schedule collects a list of household members and basic household demographic information and is used to select respondents who are eligible for individual survey, the individual survey provides information on household assets, reproductive histories, health, and nutritional status of the women’s young children.
The DHS surveys use the following assets and services in constructing the wealth index. DHS wealth index is made up of the following items: flooring, water supply, sanitation facilities, electricity, radio, television, telephone, refrigerator, vehicle, persons per sleeping room, ownership of agricultural land, domestic servant, and some country-specific items. Principal components analysis (PCA) is used for the DHS wealth index. The DHS procedure uses SPSS factor analysis method. First, the indicator variables are standardized by calculating z-scores, then factor coefficient scores are calculated for each household’s index value. The resulting sum is itself a standardized score with a mean of zero and a standard deviation of one.
Rutstein and Johnson (2004) argued that wealth as a measure of economic status has several advantages. It represents a more permanent status than does either income or consumption. A pooled model represents data on different countries pooled together without regard to differences that may result in different coefficients. Houweling and Kunst (2010) suggested future studies to examine the comparability of the wealth indices, and to complement these by measures based on educational level, ethnicity, geography, and other dimensions of social position. Wooldridge (2013) stated that an independently pooled cross section is obtained by sampling randomly from a large population at different points in time, usually, but not necessarily, different years. Ware (1984) concluded that women who have been to school lose fewer of their children in childhood and infancy than their unschooled peers. Schultz (1984) concluded that empirical study of the biological and behavioral determinants of child survival may proceed in two directions: either to estimate the reduced-form unconditional relationships between child survival and individual and community level variables that are assumed to be exogenous to the many demographic, consumer, and producer choices a household makes over time or to estimate both the demand equations for health inputs and the production function linking health inputs to child survival by simultaneous structural equation methods. Child survival should be viewed as one among many endogenous household variables that are modified by economic and demographic choices (Schultz, 1984).
Description of Variables Used
The categorical and socio-economic and socio-demographic variables used for the multivariate analysis are in Table 6: mother’s educational attainment (no education, primary, secondary, and higher), place of residence (urban/rural residence), wealth quintiles (poorest 20% is assigned the lowest quintile and the richest 20% is assigned the highest quintile), geopolitical regions or zones of six (north-central, north-east, north-west, south-east, south-south, and south-west), religion (Christians, Islam, Traditionalist, Other), child sex (male or female), birth in the last 3 years, (less than or equal to two births, or more than two births), birth order (less than or equal to four or more than four), place of residence (rural or urban), and use of health facility (use or not use health facility in the last 12 months).
Statistical Models
Table 6 is the multivariate logistic regression that shows the odds ratio of infant and child mortality based on mother’s educational attainment, wealth quintiles, zonal place of residence, religion, child sex, number of births in the last 3 years, birth order less than four, place of residence either rural or urban, and use of health facility.
Model 1 is multivariate logistic regression of infant mortality in Nigeria for 2003 and 2008 DHS data. Model 2 is also multivariate logistic regression of infant mortality in Nigeria for 2003 and 2008 DHS data. However, we test the effect of place of residence for urban/rural on infant mortality in Nigeria in Model 2. Model 3 is multivariate logistic regression of child mortality in Nigeria for 2003 and 2008 DHS data. Model 6 is multivariate logistic regression of child mortality in Nigeria with urban/rural place of residence as an independent variable to account for differences in place of residence for 2003 and 2008 DHS data.
Descriptive Statistics
Trends in Infant and Child Mortality in Nigeria
Figure 1 presents the change in infant mortality in the 36 states of Nigeria and the Federal Capital Territory (FCT) Abuja between 2003 and 2008. Among the 36 state, 11 states and the FCT Abuja saw an increase or no change in infant mortality between 2003 and 2008. Infant mortality declined in 25 of the 36 states between 2003 and 2008. Figure 1 also shows that Oyo State, Imo State, and FCT Abuja, with 118%, 116%, and 77% had the highest increase in infant mortality respectively between 2003 and 2008. Among the 25 states where infant mortality decreased, Nassarawa State, Ondo State, and Osun State recorded the highest decrease in infant mortality (64%, 47%, and 45% respectively) between 2003 and 2008. Overall, infant mortality decreased from 100.7 to 81.6 per 1,000 live births or by 18.97% between 2003 and 2008 in Nigeria.

Trend in infant mortality 2003-2008 in 36 states of Nigeria.
Figure 2 shows under-5 or child mortality in the 36 states of Nigeria between 2003 and 2008. Child mortality increased in 8 of the 36 states and in FCT Abuja between 2003 and 2008. Abia State, Imo State, and Anambra State had an increase of 93.54%, 75%, and 33.76% respectively between 2003 and 2008. Child or under-5 mortality decreased in 28 of the 36 states of Nigeria between 2003 and 2008. Among the 28 states that recorded decreases in child mortality, Nassarawa State, Zamfara State, and Osun State saw declines of 58.88%, 48.74%, and 46% respectively between 2003 and 2008. From 2003 to 2008, Nigeria recorded a decline of 19.93% in child mortality. Child mortality decreased from 139.5 to 111.7 per 1,000 live births during this period. Among the 36 states, Zamfara State had the highest under-5 mortality rate of 230.8 per 1,000 live births in 2003, whereas Kwara state had the lowest under-5 mortality rate of 34.1 per 1,000 live births in 2003.

Trend in under-5 mortality 2003-2008 in 36 states in Nigeria.
Figure 3 presents the change in urban under-5 mortality rates in the six geopolitical zones of Nigeria. From Figure 3 we see that south-west geopolitical zone had the highest decline in child mortality. South-west zone recorded a decline of approximately 30% in child mortality during this period. South-south and north-west geopolitical zones each recorded a decline of 21% in child mortality. North-east geopolitical zone saw a decline of 14% in child mortality whereas south-east geopolitical zone had a decline of 11% in child mortality. The only geopolitical zone that recorded an increase in child or under-5 mortality in all the zones was the north-central geopolitical zone. North-central geopolitical zone had an increase of 14% in child or under-5 mortality rate in her urban areas. Figure 4 is the change in child or under-5 mortality in rural Nigeria among the six geopolitical zones. Figure 4 shows south-east geopolitical zone as the only geopolitical zone with increase in child mortality in the rural areas of Nigeria. Among the other five geopolitical zones where child or under-5 mortality decreased in the rural areas, north-east geopolitical zone had the highest decrease. North-east rural geopolitical zone recorded a decrease of 31%. South-south geopolitical zone was second in reducing rural child mortality with a decrease of 29% between 2003 and 2008. North-central, north-west, and south-west geopolitical zones followed in child mortality reduction of 25%, 20% and 4% respectively.

Change in urban under-5 mortality in six geopolitical zones of Nigeria 2003-2008.

Change in rural under-5 mortality in six geopolitical zones of Nigeria 2003-2008.
Table 1 shows the distribution of risk of infant and child mortality in the six regions of Nigeria. Table 1 shows the proportion of wealth quintiles, mothers’ education, number of births in the last 3 years, religion, and other variables that explain the disparities in infant and child mortality in Nigeria in the six regions. Table 1 shows that among the poorest wealth quintiles, the risk of infant and child mortality is 12.76 times higher (10.46/.82) in the north-east region compared with the south-west region. However, among the richest wealth quintiles, the risk of infant and child mortality is (4.57/.70) is 6.53 times higher in the south-west region compared with the north-east region of Nigeria.
Distribution of Risk of Infant and Child Mortality by Region of Residence in Nigeria Pooled 2003 and 2008 DHS.

Note. DHS = demographic and health surveys.
p < .05. **p < .01. ***p < .001.
Table 2 shows the distribution of the risk of infant mortality in the six regions of Nigeria. The risk of infant mortality is (2.58/0.72) 3.58 times higher for the poorest wealth quintiles compared with the richest wealth quintiles in Nigeria. The risk of infant mortality between the poorest wealth quintiles in the south-west region and the poorest wealth quintiles in the north-east region shows a disparity of (4.75/.48) 9.9 times higher for the north-east region. Within the north-east region, we see a very high degree of disparity between the richest wealth quintile and the poorest wealth quintile. The difference in risk of infant mortality is (4.75/.08) 59.4 times higher for the poorest wealth quintile in north-east region.
Distribution of Risk of Infant Mortality by Region of Residence in Nigeria Pooled 2003 and 2008 DHS.

Note. DHS = demographic and health surveys.
p < .05. **p < .01. ***p < .001.
Table 3 shows a similar pattern that we saw in both Tables 1 and 2. Wealth and education show a gradient in child mortality in Nigeria. North-west region has the highest risk of child mortality among mothers with no education. The risk of child mortality is (11.24/1.19) 9.4 times higher for mothers with no education in north-west compared with mothers with no education in the south-west region of Nigeria. The risk of child mortality is (9.21/2.45) 3.76 times higher in rural Nigeria compared with urban Nigeria. Also, Table 3 shows that the risk of child mortality in Nigeria is (8.72/2.94) 2.97 times higher for those who did not use health facility over the last 12 months compared with those who used it over the same period. The distribution of risk of child mortality is almost consistent across the six regions for households that made use of health facilities. However, the risk of child mortality between the south-west region and south-east, south-south, north-central, north-east, and north-west is 1.93 times, 2.16 times, 2.15 times, 2.73 times and 3.10 times respectively.
Distribution of Risk of Child Mortality by Region of Residence in Nigeria Pooled 2003 and 2008 DHS.

Note. DHS = demographic and health surveys.
p < .05. **p < .01. ***p < .001.
Table 4 is the unweighted infant mortality in the 36 States of Nigeria and Federal Capital Territory (FCT) Abuja. Table 4 shows the actual survey counts in both 2003 and 2008. Table 4 also shows the mean mortality rate per 1,000 live births in the two DHS surveys. We calculate the percentage change in the rate of mortality for each state by the following: [Mean mortality rate of 2008 − Mean mortality rate of 2003] / Mean mortality rate of 2003 × 100. For Under-5 or child mortality, we applied the above method in Table 5. As discussed elsewhere, the results are consistent with Figures 1 and 2.
Unweighted Infant Mortality Trend in 36 Nigeria States in 2003 and 2008.

Source. DHS 2003, 2008 data and authors calculations.
Note. NA = not applicable; DHS = demographic and health surveys. Values in parenthesis represent decrease in mortality.
Unweighted Under-5 Mortality Trend in 36 Nigeria States in 2003 and 2008.
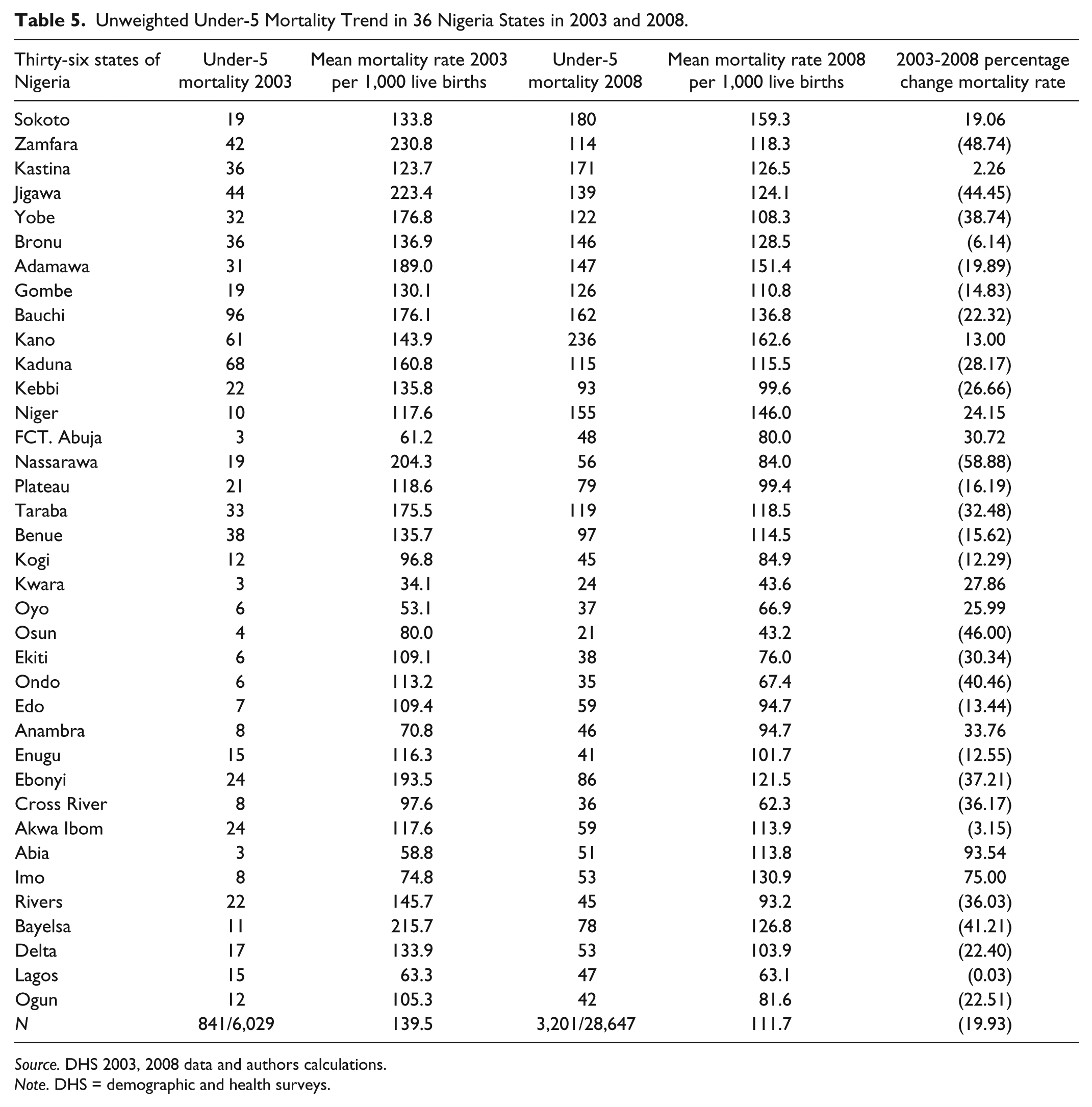
Source. DHS 2003, 2008 data and authors calculations.
Note. DHS = demographic and health surveys.
Estimation Results
Table 6 shows the summary of the different logistic regressions on infant and under-5 mortality rates in Nigeria. Model 1 is the pooled infant multivariate logistic regression. Model 1 shows an inverse relationship in infant mortality with primary, secondary, and higher educational attainment. However, only higher education is significant in lowering the risk of infant mortality. The richer and the richest wealth quintiles show the risk of infant mortality falling. Compared with the north-central geopolitical zone as the referent point, north-east geopolitical zone has an odds ratio of 1.05. Basically, the odds of experiencing infant mortality increase by 5% in north-east geopolitical zone than in north-central geopolitical zone. The odds of infant mortality increase by 2% in north-west geopolitical zone than in north-central geopolitical zone. The odds of child mortality increase by 15% in south-east geopolitical zone than in north-central geopolitical zone. The odds of infant mortality increase by 6% in south-south geopolitical zone compared with north-central geopolitical zone. The odds of infant mortality decrease by 19.2% in south-west geopolitical zone. This is the only geopolitical zone with lower odds of infant mortality than north-central geopolitical zone among the six geopolitical zones in Nigeria.
Logistic Regression Models on Infant and Child Mortality in Nigeria 2003 and 2008 DHS Data.

Note. t statistics in parentheses. DHS = demographic and health surveys.
p < .10. *p < .05. **p < .01. ***p < .001.
When we examine the effect of religion on infant mortality, we see that those who practice traditional religion has odds of 1.11 times higher in infant mortality than those who practice Christian religion in Nigeria. The odds of infant mortality for those who practice Islam is 5.23% lower compared with those who practice Christian religion. Although this result is not significant, however, the odds of infant mortality is 1.75 times higher for Other religions compared with Christian religion and are statistically significant. Table 1 show that female children have higher odds of surviving than male children in Nigeria. The odds of infant mortality decrease by 13.75% for female infant compared with male infant in Nigeria. The odds of infant mortality increase by 5.1 times for mothers who had more than two births in the last 3 years.
Higher birth order is positively associated with under-5 mortality in Nigeria. The odds of infant mortality decrease by 83.67% for birth order lower than four. The odds of infant mortality decrease by 12.65% for those who use health facility and the result is highly statistically significant.
Model 2 is the logistic regression of infant mortality in Nigeria with place of residence as an explanatory variable. The results are similar to the results in Model 1. From Table 6 we see that living in urban Nigeria results in lowering the risk of infant mortality by 13.75%. When we examine infant mortality in the six geopolitical zones with north-central as the referent zone, we find a similar pattern as in Model 1.
Model 3 is the logistic regression for child mortality in Nigeria. As evident in the result, educational attainment is now significant at both secondary and higher level. The signs performed as expected. Both the richer and richest wealth quintiles are highly associated with reduction in under-5 mortality in Nigeria. The odds of child mortality for the richest wealth quintile decrease by 37.67% compared with the poorest wealth quintile. The odds of child mortality for the richer wealth quintile decrease by 20.05% compared with the poorest wealth quintile. The odds of child mortality increased in the six geopolitical regions with the exception of south-west geopolitical region when compared with the north-central geopolitical zone. The odds of child mortality in the six zones of north-east, north-west, south-east, and south-south increased by 17.44%, 20.63%, 15.94%, and 12.49% compared with north-central zone respectively. The odds of child mortality in south-west geopolitical zone decrease by 21.10% compared with north-central geopolitical zone. On religion, we find the odds of child mortality in Nigeria increase by 22.79% for traditional religion compared with Christian religion. The odds of child mortality in Nigeria increase by 79.74% for Other religion. The odds of child mortality in Nigeria decrease by 2.81% for Islam compared with Christian religion.
The variable representing lower than or equal to two births in the last 3 years is highly inversely associated with decrease in under-5 mortality rate in Nigeria. The odds of child mortality in Nigeria decrease by 80.71%. Birth order lower or equal to four decreases child mortality in Nigeria and is highly significant. The odds of child mortality in Nigeria for female child falls by 11.72% compared with a male child in Nigeria. The variable for health use is significant in explaining child mortality in Nigeria.
Model 4 is the logistic regression of child mortality in Nigeria with place of residence included as an explanatory variable. Educational attainment is highly significant in reducing child mortality at secondary and higher levels. The odds of child mortality in Nigeria decrease by 2.26%, 15.83%, and 39.22% for mothers with primary, secondary and higher education respectively compared with mothers with no education. The wealth variable is highly significant for the richest quintile and barely significant for the richer quintile. Among the six geopolitical zones, only south-south geopolitical zone is not significant compared with the north-central zone. Although the south-east is barely significant at 10% level of significance, the north-east and north-west zones have higher odds of child mortality compared with the north-central zone and are statistically significant. Only the south-west zone has a lower odds of child mortality compared with the north-central zone in Nigeria. On religion, we see a similar pattern with the results of Model 3. Again, similar to the result on infant mortality with place of residence in Model 2, we find the odds of child mortality in urban Nigeria to be 15.34% lower compared with child mortality in rural Nigeria.
Discussion
This study showed that both infant and child mortality was significantly associated with region of residence in Nigeria. The risk of infant mortality is significantly higher for mothers in north-east and north-west regions of Nigeria after adjusting for wealth and mothers’ education compared with mothers in south-west and north-central regions of Nigeria. This result is similar to the findings of Antai (2011). The results in Table 6 Models 1 to 4 seem to confirm the high proportions in Table 1 of mothers with no education and primary education in the three northern regions compared with the three southern regions of Nigeria.
Table 1 also shows a high proportion of the poorest and poorer wealth quintiles resident in the northern regions of Nigeria compared with the proportion that is resident in the southern regions of the country. Higher proportions of the richer and richest wealth quintiles are resident in the southern regions of Nigeria compared with the proportion resident in the northern regions of Nigeria. The findings in this study indicate that the south-west region has the lowest infant and child mortality in Nigeria. Obviously, this is an indication of the fact that more health facilities, social amenities, and educational institutions are available in the south-west region than in any other region of Nigeria.
These facilities provide an enabling environment that reduces the risk of infant and child mortality. Table 1 shows that 70.45% did not make use of health facility, and only 29.55% used health facility in Nigeria. However, compared with Nigeria, the proportion in the south-west region who did not use health facility to those that used it is almost the same, with those who used it 5.76% slightly higher than those who did not use it (5.60%). The two other southern regions of Nigeria, south-east and south-south regions, show a smaller difference between those who used health facility and those who did not use it. In the south-east region, the proportion who used health facility is 2.95% compared with 5.63% who did not use health facility. In the south-south region, the proportion is 4.18% who used it compared with 7.03% who did not use health facility.
In north-central region, the proportion that used health facility is 5.60% compared with 11.88% who did not use health facility. In the north-east region, the proportion that used health facility is 5.80% compared with 17.41% who did not use health facility. In the north-west region, the proportion that used health facility is 5.27% compared with 22.90% who did not use health facility. The proportion of mothers having two or more births in the last 3 years is higher in the northern regions of Nigeria than in the southern regions of Nigeria. The above findings are consistent with the conclusions reached by Adedini et al. (2013).
The results from multivariate logistic regressions of Table 6 show that mothers with higher level of educational attainment has lower odds of infant mortality and it is statistically significant. For child mortality, the odds are even better. Mothers with both secondary and higher levels of educational attainment have lower odds of child mortality in Nigeria and these results are statistically significant at both 5% and 1% level respectively. This finding gives credence to previous studies (Anyamele, 2011; Caldwell, 1979; Kabagenyi & Rutaremwa, 2013; Mosley & Chen, 1984).
Table 6 shows that household wealth is statistically significant at both richer and richest wealth quintiles in reducing infant mortality as evident on both Model 1 and Model 2 respectively. Models 3 and 4 on Table 6 show that richer and richest wealth households in Nigeria have lower odds of child mortality. These results are similar to the findings of past studies (Anyamele, 2011; Fotso, 2006; Hong, 2006; Houweling & Kunst, 2010; McMichael, 2000; Todd, 1996; Victora et al., 2000; Victora et al., 2003; Wagstaff, 2000). The multivariate logistic regressions of Table 6 on Model 1 show that geographical place of residence is only statistically significant in reducing infant mortality in the south-west region of Nigeria. Furthermore, this result is similar to the result of Model 2 that used urban/rural residence as an explanatory variable. Models 3 and 4 show that north-east and north-west has higher odds of child mortality in Nigeria. Also, Model 4 shows that the south-east region has higher odds of child mortality and it is statistically significant only at 10% level of significance. Again, the results from both Models 3 and 4 show that the south-west region has lower odds of child mortality in Nigeria. From Model 4 we see that households that live in urban areas have lower odds of child mortality than households that live in rural areas of Nigeria. This is also the result on infant mortality in Model 1 from Table 6. These results are similar to previous findings on rural/urban residence (Anyamele, 2009; Cai & Chongsuvivatwong, 2006; Fotso, 2006; Kuate-Defo & Diallo, 2002). The limitation of this study comes from not being able to include the 2013 DHS data.
Conclusion and Policy Implications
This study has established strong disparity in infant and under-5 mortality rates between the six geopolitical zones of Nigeria and in the 36 states. Furthermore, our findings show that urban Nigeria continues to have advantage over rural Nigeria in infant and under-5 mortality rates. Educational attainment, wealth, the use of health facility, and religion appear to be strongly associated with both infant and under-5 mortality rates in Nigeria.
Some of these findings are in agreement with previous studies on the topic (Adedini et al., 2013; Antai, 2011; Anyamele, 2009, 2011; Ettarh & Kimani, 2012; Houweling & Kunst, 2010; Van de Poel, O’Donnell, & Doorsaer, 2009). The policy implications of these findings are that policies and programs should be implemented to target poverty alleviation in both rural and urban areas of Nigeria. It is also evident from our results that increasing educational attainment and literacy levels in all the states will greatly reduce infant and under-5 mortality rates in Nigeria. It is obvious from our results that Nigeria continues to have high infant and under-5 mortality rates. This finding gives credence to previous work by (Ngowu et al., 2008). However, the trends show a steady decline in both infant and under-5 mortality rates in Nigeria.
The intervention measures in infant and children immunization of 2003 in most of the north-west and north-east geopolitical zones seem to have helped in the reduction of infant and under-5 mortality rates in the two zones. Such efforts should continue in all the zones of Nigeria.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.