
Abstract
Insufficient literature has been produced addressing children with borderline intellectual functioning (BIF) and gifted intellectual functioning (GIF). The goal of this work is to compare levels of self-esteem, depression, anxiety at school, and insecurity among children with BIF and GIF, and a control group of average intellectual functioning (AIF). There were participants of 104 children (fourth grade of primary school). Analyses revealed that children with BIF showed a lower level of self-esteem and higher levels of depression and school anxiety. Moreover, our findings highlight the co-occurrence of school anxiety, depressed mood, and insecurity among the BIF and AIF groups. One of the issues that emerge from this study is the need to implement prevention programs aimed at identifying children with lower or higher levels of intellectual functioning. These findings highlight the importance of establishing what the most appropriate educational and clinical interventions are in reducing the risks of mental disorders in this population.
Keywords
Introduction
Recent studies in the field of developmental psychology have led to an increasing interest in mental health and early identification of mental disorders in the school-aged population (Ahlen, Breitholtz, Barrett, & Gallegos, 2012; Alesi, Rappo, & Pepi, 2014). To date, insufficient literature has been produced addressing the study of this issue in children with borderline intellectual functioning (BIF) and gifted intellectual functioning (GIF). Nevertheless, in spite of their high occurrence, these two intellectual conditions are undertreated and often misinterpreted. They hold heterogeneous groups of children showing some similarities, despite their apparent contrasting nature given by slowness in BIF and precocity in GIF.
First, an ample variety of names is used to label participants falling into these two groups. More clearly, children with BIF are often labeled slow learners or backward learners (Vianello, 2008). Similarly, gifted intellectual children are called children with high intellectual functioning or intellectual “precocity,” high-level potentialities, or talented children.
This overlapping of linguistic labels underlies complex theoretical and methodological issues. We argue that these terms cannot be assumed as synonymous, because they differ in meaningful ways. For example, the expression BIF refers to a condition of boundary between typical and atypical intellectual level, while the expression slow learners taps the long time spent in acquiring school skills or to complete achievement tasks. Similarly, gifted and talented children are not terms to be used interchangeably; giftedness indicates an aptitude in a specific domain (e.g., music, art, athletics, writing . . . ), while talent denotes the result of the giftedness (Majid & Alias, 2010).
Second, other similarities between the two intellectual conditions can be found in their underestimated occurrence, which is largely based prevalently on their IQ values. BIF can be commonly identified as scoring between one and two standard deviations below the IQ mean (range = 70-85) and has a prevalence of 13.6% in the general population. However, this rate decreases to 7% assuming the adaptive functioning as required by the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association [APA], 2013). “ . . . differentiating borderline intellectual functioning and mild intellectual disability (intellectual developmental disorder) requires careful assessment of intellectual and adaptive functions and their discrepancies, particularly in the presence of co-occurring mental disorders that may affect patient compliance with standardized testing procedures.”
Moreover, the main features appear to be the delay and the slowness in the acquisition of motor and cognitive competences. Specifically, children with BIF show late information processing abilities, narrow working memory capacity, limited executive functioning, and selective-attention problems (Ninivaggi, 2001; Schuchardt, Gebhardt, & Maehler, 2010). Social abilities such as perspective taking and the interpretation of social situations are particularly impaired. The cause of this impairment would seem to be an inadequate system of Social Information Processing (SIP) closely linked to the slowness in selective attention, decreased working memory capacity, and increased inhibition processes (Van Nieuwenhuijzen, Vriens, Scheepmakerc, Smitc, & Porton, 2011).
However, Gifted Intellectual Children commonly score two standard deviations over the IQ mean (more than 130) and have a prevalence of 2.3% in the general population. Revol and Bléandonu (2012) outlined the profile of these children and have identified nine behavioral characteristics: variety of interests, extraordinary curiosity, persistence in front of difficulties, creativity or divergent thinking, leadership, overdeveloped language abilities, high emotional competences, sensitivity, and sense of justice. On the whole, these children show quicker development in one or more areas: physical, cognitive, linguistic, and social (Gur, 2011). Gifted children are often described as intrusive and full of energy; from early childhood, they are very curious, inquisitive, and keen to discuss concepts of their interest and create extensive descriptions. Moreover, they produce their first words and sentences very early on, subsequently mastering a broad vocabulary; they use their language in a creative way, and they produce complex sentences, making up stories, and are able to understand symbolic or abstract meanings. Often, these children dislike cooperating with their chronological-age peers because they do not share similar interests. Consequently, they prefer working alone or with older children and adults (Smutny, 2000).
Third, the elevated co-occurrence between the above-described intellectual conditions and school complaints such as learning disabilities (LD) and attention deficit hyperactivity disorders (ADHD; Vianello, 2008) is worth noting.
Ample evidence has been found associating BIF and LDs, especially dyslexia. This comorbidity paradoxically seems to contrast the diagnosis criterion of exclusion of impaired intellectual level in children with LD. However, a close association between the two conditions has been postulated by Vianello (2014), who argued that the comorbidity of BIF and LD is 1 each 408 to 571 pupils on the basis of the guidelines of Consensus Conference (AA.VV., 2009). Karande, Kanchan, and Kulkarni (2008) documented the academic history of 55 children with BIF and have found high rates of comorbidity with poor school performance (89.1%) and difficulties in writing (92.7%) and mathematics (76.4%). This is consistent with results of Fernell and Ek (2010) who focused a great amount of academic difficulties, namely, the struggle to cope with school tasks and classroom demands, conduct disorders, and externalizing symptoms associated with lower levels of inhibition. Through analyzing this issue in depth, several possible explanations for the comorbidity of BIF and LD can be hypothesized. First, an impaired processing speed can be identified as a main factor that limits “the amount of information that can be processed in a given time interval” with longer reaction times (RTs) in cognitive tasks and slower performance in intellectual tasks (Bonifacci & Snowling, 2007). Second, the delayed cognitive development and information processing characterizing the BIF creates memory or selective-attention problems, which in turn compromise the capacity to successfully acquire school capacities (Van Nieuwenhuijzen et al., 2011).
Moreover, epidemiological studies have revealed in children and adolescents with BIF high rates of ADHD ranging between 20% and 30% as well as behavioral problems about 58.2% (Karande et al., 2008).
However, the association between giftedness and LDs has been controversial (Kirmani, Al-Kadi, Iftikhar, & Mayat, 2014; Majid & Alias, 2010). In his recent review, Vaivre-Douret (2011) analyzed factors involved in the neuropsychological and psychopathological etiology of LDs in high-level potentialities children. The first factors included written language disorders such as dyslexia, spelling difficulties, dyscalculia, and dysgraphia. The second factors embraced underperforming, psycho-affective immaturity, anxiety, and behavioral fluctuations. The author therefore argued how the typical precocity of this population could make these children more vulnerable in developing LDs because it consents to use compensation strategies, which, in turn, mask eventual learning difficulties and make difficult the diagnosis in highly gifted children.
A certain number of studies reported the comorbidity between giftedness and ADHD (Bénony, Van Der Elst, Chahraoui, Bénony, & Marnier, 2007; Karande et al., 2008; Kirmani et al., 2014). Specifically, multiple and contradictory causes have been identified in this population: (a) the typical motor instability associated with hyperactivity and impulsivity, (b) boredom in the classroom due to out-of-ordinary intellectual capacities determining a higher processing speed, (c) the quickness to complete school tasks before classmates, and (d) the affective development and relational difficulties with peers (Revol & Bléandonu, 2012).
Fourth, a variety of authors documented children with BIF as a population at high risk of mental health disorders (Cooper, Smiley, Morrison, Williamson, & Allan, 2007; Einfeld et al., 2006: Emerson & Hatton, 2007). It has been demonstrated that a large number of children with BIF are more likely to show higher rates of anxiety and depression as well as developing neurotic and personality disorders as opposed to typically developing peers (Emerson, Einfeld, & Stancliffe, 2010; Fernell & Ek, 2010).
Anxiety disorders are considered the most prevalent mental impairments in typical and atypical children (Kozina, 2014). Anxiety is a discomfort reaction associated with unpleasant emotions and a state of distress occurring in response to situations or tasks that are perceived as threatening to self-worth (Pereira, Barros, & Mendonça, 2012). Moreover, anxiety disorders are frequently in comorbidity with depressive symptoms with rates ranging from 16% to 50% increasing in chronicity and severity (Jacobson & Newman, 2014). A common core of high negative affects is the leading cause of this comorbidity. The consequence is the interference with daily functioning for a sizable population of children (Cooper et al., 2007; Wright, Banerjee, Hoek, Rieffe, & Novin, 2010). However, scholars and practitioners agree that natural concerns clearly follow developmental waves during the growth. Fears regarding separation anxiety decrease during early childhood, whereas fears about school and school anxiety increase during later childhood (Grills-Taquechel, Fletcher, Vaughn, & Stuebing, 2012). So school anxiety is the most frequent fear occurring during school age. It describes a discomfort reaction associated with unpleasant emotions and a state of distress occurring in response to situations involving school learning tasks that are perceived as threatening to self-worth.
At this age, the close relationship between depressive symptoms and anxiety is largely reinforced by lower levels of school self-esteem (Bernaras, Jaureguizar, Soroa, Ibabe, & Cuevas, 2011). Karande et al. (2008) explain this loss of self-esteem by claiming the significant emotional distress linked to difficulties in school, social, or vocational competences. Often, lower levels of school self-esteem are associated to poor achievement at school. Specifically, higher achievers are more likely to develop positive school emotions and affects, which, in turn, reinforce their engagement and motivation in school activities, while students with school underachievement are more likely to show lower global self-esteem and to report increasing anxious and depressive symptomatology.
Similarly, gifted children were reported to be highly vulnerable in developing mental health disorders. From a developmental perspective, this risk already manifested during childhood may grow and become significant in adolescence; gifted adolescents often show anxiety and depressive symptoms associated with inhibition and academic disinvestment as well as immature affective development and relational difficulties with their peers. In turn, distress and anxiety reinforce a loss of interest in learning by creating intellectual inhibition and refuse to cope with challenging tasks (Vaivre-Douret, 2011). Mood and conduct disorders are the direct consequence of this situation (Bénony et al., 2007; Guénolé et al., 2013). As Majid and Alias (2010) state “ironically, the gift does not only bring joy and happiness, but it also brings with it danger, anxiety and disappointment” (p. 63). Moreover, giftedness can become a limit if the gap between cognitive and emotional development is too wide. This may lead to the phenomenon “Shattered Idealism,” which is characterized by a negative self-awareness and maladaptive motivational profile, which has an effect on disruptive behaviors (Alesi, Rappo, & Pepi, 2012; Blakeley, 2001).
Given the literature findings and speculative interpretations, comparisons of ratings of depression, school anxiety, insecurity, and self-esteem at school endorsed by pupils with different levels of intellectual functioning (BIF, AIF, GIF groups) were assessed. In particular, the following hypotheses will be tested in this research:
Method
Participants
Participants were 104 non-clinical children whose mean age was 9.5 years (range = 8.7-9.9 years). With regard to sex, there were 35 female and 69 male participants. They were selected from a sample of 265 pupils on the basis of their level of intelligence. All children were attending fourth grade of the primary school and fell into three groups on the basis of level of intelligence: (a) BIF, (b) AIF, and (c) GIF. The BIF group was composed of 25 children, aged 9.6 (range = 8.8-9.9 years), with Raven’s scores lower than 15 percentile and mental age greater than 8 years. The AIF group was composed of 62 children aged 9.4 (range = 8.7-9.7 years), with Raven’s scores from 35 to 75 percentile. Finally, the GIF group was composed of 17 children aged 9.4 (range = 8.9-9.5 years), with Raven’s scores higher than 88.
Prior to the start of the study, written informed consent was provided by each participant’s parents. Moreover, appropriate local ethics committee approval was obtained from the University of Palermo.
Materials
Raven’s Progressive Matrices
The Raven’s (2008) Progressive Matrices were administered to measure general intelligence. This test evaluates the development of logical thinking. Given a matrix of geometric shapes, children were required to select the correct missing shape among a set of items. For each item, evaluation was binary, with a score of 1 being attributed to each correct item, and 0 to incorrect items.
OL test
The Organizzazioni Logiche (OL; Vianello & Marin, 1997) test was administered to determine mental age of the participants. The OL test consists of 18 items subdivided into three areas of logical operation (ordering, numbering, and classification). Evaluation was binary for each item, with a mark of 1 being attributed to each correct item and 0 to each incorrect item. The raw data thus obtained were then transformed into a measure of mental age (range = 4-8 years) using appropriate conversion tables. The OL test shows good validity, with a .68 correlation with Wechsler Intelligence Scale and a.78 correlation with the Columbia Mental Maturity Scale. The reliability of the OL test is .87.
School self-esteem
The Test Multidimensionale Autostima (TMA)–Multidimensional Test of Self-Esteem, realized by Bracken (1992), was used to measure self-esteem at school. This test assesses the global self-worth by means of six different scales of self-esteem (Social, Competence, Affect, School, Family, and Physical).
The administration was individual. In particular, for our research, we used the scale to evaluate the school self-esteem. This scale consisted of 25 items, positive and negative, related to the way pupils feel about themselves in the school domain. Participants were asked to express their level of agreement with statements such as I am proud of my schoolwork or I do not understand much what I read. Each item was presented on a 4-point Likert-type scale from absolutely true to absolutely false. The test–retest reliability of the battery was r = .90.
School anxiety
Self Administrated Psychiatric Scales for Children and Adolescents (SAFA) was an Italian test (Cianchetti & Fancello, 2001) aimed at assessing mental impairments in children and adolescents with age ranging from 8 to 18 years.
Specifically, SAFA was a battery that consisted of six scales, subdivided in subscales, suitable to be administrated separately. The scales were Anxiety (SAFA A), Depression (SAFA D), Obsessive–Compulsive Symptoms (SAFA O), Somatic Symptoms and Hypochondria (SAFA S), Phobias (SAFA F), and Psychogenic Eating Disorders (SAFA P).
Moreover, each scale consisted of two versions suitable for participants aged 8 to 10 years and 11 to 18 years.
Each item was scored from 0 to 2.
In our study, SAFA A and SAFA D were administered. The first measured the school anxiety, with 12 items, such as When I go to school I often feel very nervous. The second measured the depressed mood, with six items, such as I often feel sad without any reason, and the insecurity, with six items, such as I am sure of myself.
Each item was presented on a 3-point scale from true to false.
The test–retest reliability of the battery was r = .90.
Procedure
At the beginning of the research, a screening was done on all fourth graders from two public schools located in quarters of medium socioeconomic level. The screening was carried out in 3 months. All children were assessed with the Raven’s Progressive Matrices to evaluate their level of intellectual functioning. To evaluate mental age in BIF group, children were assessed with the OL test.
All children with Raven’s scores lower than 15 percentile were administered with the OL test to identify their mental age. Only the children who had a mental age greater than 8 were grouped with BIF.
All children with Raven’s scores from 35 to 75 percentile were grouped with AIF.
All children with Raven’s scores higher than 88 were grouped with GIF.
After the screening, 104 children were selected and subdivided into 3 groups: group BIF (n = 25 pupils) characterized by low level of intellectual functioning, group AIF (n = 62 pupils) characterized by average level of intellectual functioning, group GIF (n = 17 pupils) characterized by high level of intellectual functioning.
All children were administered School Self-Esteem, School Anxiety, Depressed Mood, and Insecurity tests. The order of presentation of the four tests was balanced.
The administration modality was individual, and it did not last more than 25 min.
Results
The first goal of this study was to verify whether intellectual functioning, in our sample, would follow a normal distribution.
The Levene’s test revealed that the distribution of intellectual functioning in our sample of 265 children with mean age of 8.5 years was nearly normal (p < .001; see Table 1).
Homogeneity of Variance Test.
We found a nearly normative distribution in which most pupils (66.03%) showed average levels of intellectual functioning. Pupils with BIF were 15.47%, and pupils with high intellectual functioning were 6.42%.
The second goal of this study aimed to investigate the level of school self-esteem, school anxiety, depressed mood, and insecurity in the three groups of children with different levels of intellectual functioning (BIF, AIF, GIF groups).
To investigate this issue, a one-way ANOVA was performed using the level of intellectual functioning as an independent variable, while the dependent ones were school self-esteem, school anxiety, depressed mood, and insecurity. The one-way ANOVA was calculated. The level of significance was set at p < .05. The SPSS software (Version 20 for Windows) was used.
One-way results revealed significant differences for self-esteem, F(2, 101) = 3.086, p = .05; school anxiety, F(2, 101) = 4.341, p = .016; and depressed mood, F(2, 101) = 4.592, p = .012. There were no significant differences for insecurity, F(2, 101) = 1.019, p = .356.
After the application of Bonferroni post hoc test (p < .05), we observed significant differences between the BIF group and the GIF group. To be more precise, pupils with BIF showed a lower level of self-esteem (M = 95.96) than pupils with high intellectual functioning (M = 104.35).
With regard to the level of school anxiety, the analysis of Bonferroni post hoc test (p < .05) revealed that the BIF group (M = 55.12) showed higher level of school anxiety than the AIF group (M = 46.97).
Finally, the BIF group (M = 49.68) revealed higher level of depressed mood than the AIF group (M = 45.10) and the GIF group (M = 44.53; see Table 2 for means and standard deviations of self-esteem, school anxiety, depressed mood, and insecurity by group).
Descriptive Statistics for Self-Esteem, School Anxiety, Depressed Mood, Insecurity in Three Groups.

Regarding the relationship between self-esteem, school anxiety, depressed mood, and insecurity, our analysis showed a significant positive correlation between school anxiety, depressed mood, and insecurity, and a significant negative correlation between school anxiety and school self-esteem was found in the BIF and AIF groups.
We observed, also, a significant negative correlation between insecurity and self-esteem, and a significant positive correlation between insecurity and depressed mood in the GIF group (see Tables 3, 4, and 5 for correlations).
Correlations Between School Self-Esteem, School Anxiety, Depressed Mood, and Insecurity in Group With Borderline Intellectual Functioning.
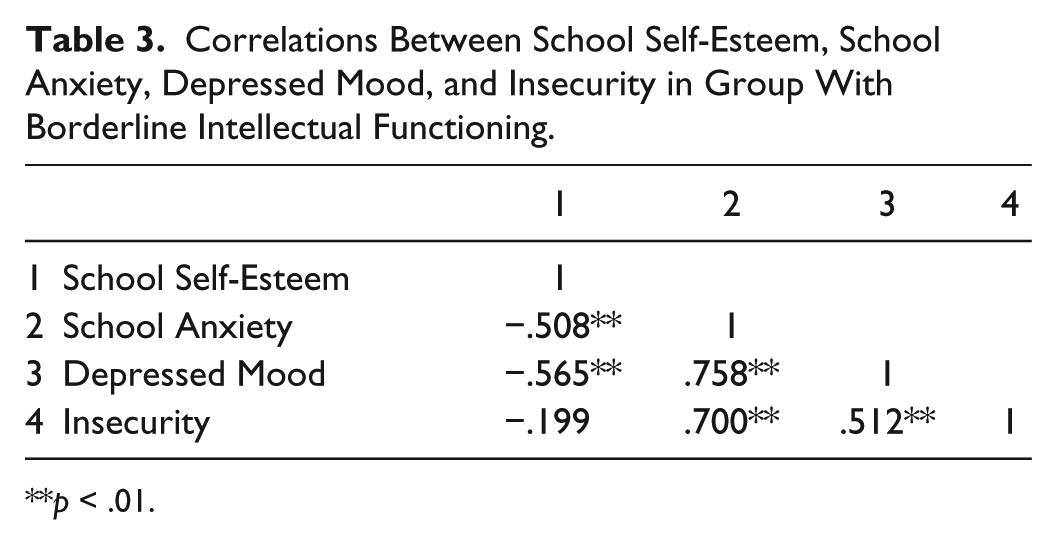
p < .01.
Correlations Between School Self-Esteem, School Anxiety, Depressed Mood, and Insecurity in Group With Average Intellectual Functioning.

p < .05. **p < .01.
Correlations Between School Self-Esteem, School Anxiety, Depressed Mood, and Insecurity in Group With Gifted Intellectual Functioning.

p < .05.
Discussion
This study set out to determine whether intellectual functioning would follow a normal distribution. We further extended previous studies by examining simultaneously three levels of intellectual functioning: (a) BIF, (b) AIF, and (c) GIF. We choose to study two opposite intellectual conditions because both BIF and GIF are often under-recognized and misdiagnosed (Revol & Bléandonu, 2012; Schuchardt et al., 2010). Moreover, epidemiological research reveals that increasing demands of contemporary society for higher levels of intellectual functioning enable these groups to be at considerable risk of psychopathology from early childhood. As a consequence, we compared the emotional profile, composed by the levels of self-esteem, anxiety, depression, and insecurity among children with low, average, and high intellectual functioning. First, we found a nearly normative distribution in which the majority of children (66.03%) showed an average level of intellectual functioning, while a minority showed a level of intellectual functioning below or above the median IQ. Specifically, children with BIF were 15.47%, and children with GIF were 6.42%. These rates are consistent with other research, which found an occurrence for individuals with BIF of about 12% to 13% in the general population if we consider only the scores on the intelligence scales without measures of adaptive functioning (Ninivaggi, 2001; Vianello, 2008). Other studies report the prevalence of 2.3% for intellectual gifted children in the general population (Revol & Bléandonu, 2012).
Second, we found significant differences between our three groups in the emotional profile. Children with BIF showed the lowest level of self-esteem and, conversely, the highest levels of school anxiety and depressed mood.
There are similarities between this emotional profile and that described by previous work in this field highlighting how low levels of school self-esteem and self-concept are commonly associated with intellectual functioning below the median IQ (Bénony et al., 2007; Majid & Alias, 2010). Individuals who experienced repeated failure, such as those with BIF, are more likely to show higher rates of anxiety and depression as well as to develop neurotic and personality disorders as opposed to their typically developing peers (Emerson et al., 2010; Fernell & Ek, 2010). When faced with some perceived or real threats, novel or ambiguous events, children with BIF are more likely to make cognitive errors or distortions characterized by a negative bias in the interpretation of facts (Pereira et al., 2012). Moreover, anxiety disorders are frequently associated with depressive symptoms with rates ranging from 16% to 50% increasing in chronicity and severity (Jacobson & Newman, 2014). The consequence is the interference with daily functioning (Wright et al., 2010).
Nevertheless, gifted children show an emotional profile characterized by significant higher self-esteem and lower depression levels than children with BIF. This is in contrast with previous studies, which underlie the close association between the lack of school self-esteem and depressive disorders in gifted children as the result of the asynchrony among their cognitive and emotional abilities (Karande et al., 2008). In the attempt to explain our result, we raise a developmental issue. More precisely, this emotional profile in our group of children with giftedness may be explained by the young age of our participants. First, we hypothesize that deficits may become increasingly evident over the time when the gap between cognitive and emotional abilities increases and environmental demands enhance. Second, if we consider the changes in self-worth across the life span and the age trajectory, self-esteem is generally quite elevated and not stable during childhood (Pepi, Faria, & Alesi, 2006; Trzesniewski, Donellan, & Robins, 2003).
Other findings to emerge from this research were the correlations between the emotional variables. Consistent with our third hypothesis, in the groups of pupils with BIF and AIF, significant positive correlations between school anxiety, depressed mood, and insecurity were observed. A possible explanation for this might be that anxiety and depression regularly co-occur with rates ranging from 0.40 to 0.70 both in clinical and non-clinical samples (Wright et al., 2010). This comorbidity bases on common high negative feelings. A lower intellectual functioning enhances the perception of negative self-competence and increases negative affects such as depressed mood, reduced pleasure and interest, irritability, fatigue, and weakened concentration.
Conversely, school anxiety and school self-esteem were negatively correlated. As mentioned by Bernaras et al. (2011), lower levels of self-esteem reinforce the anxiety. In other words, negative self-perception and self-worth increase the discomfort reaction occurring in response to threatening events. Taken together, these results indirectly suggest the key role of environmental factors such as family and school as sources of anxiety. Consistently, wide research shows that negative parents’ and teachers’ behaviors or information provided to children are associated with increased fear and anxiety. Specifically, the following factors have been found to predict anxiety disorders in children: parents’ or teachers’ anxiety, parents’ or teachers’ criticism and rejection, adults’ overcontrol and overprotection, insecure parent–child attachment, and maladaptive parenting behaviors, parental warmth, and family cohesion (Drake & Ginsburg, 2012).
No differences were found between children with BIF and GIF. The reason for this might be related to the fact that the development of negative thoughts and worries depends on logical reasoning and elaborate decisional processes. Therefore, we have to acknowledge that children with BIF have an IQ level not significantly below the median IQ. It is possible that, at this age, their intellectual level preserve their perception and awareness of their own abilities. Moreover, our results may be attributed to the age of participants and need to be interpreted as evidence in favor of a linear increase of risk to develop anxiety and depression symptoms by age. In other words, the development of negative thoughts and worries is not stable but increases over time and is largely influenced by failure experiences that accumulate with growth (Alesi et al., 2014).
Finally, in the GIF group, we found a significant negative correlation between self-esteem and emotional insecurity as well as a significant positive correlation between depressed mood and insecurity. These findings were unexpected and suggest the key role of family to influence the emotional profile of these children. According to the Emotional Security Theory (Cummings & Davies, 1996), children’s emotional insecurity is strongly influenced by environmental factors such as family sense of protection and safety. Therefore, the insecurity is more likely negatively associated with self-esteem because it demonstrates the failure of the above-mentioned process aimed at maintaining the sense of safety and security. This failure results in emotional dis-regulation experiences and a negative worth of self. In turn, emotional insecurity is designated as an explanatory mechanism for internalizing and externalizing problems (Cummings, Cheung, & Davies, 2013; Cummings, George, McCoy, & Davies, 2010). It seems possible that the insecurity is related to low self-esteem only in the GIF group given the typical sensitivity and psycho-affective immaturity of these children, which make them particularly sensitive to environmental claims.
However, it is interesting to note in all three groups of this study the positive correlation between insecurity and depressed mood. A possible explanation lies in the nature of these emotional conditions sharing a common basis of negative feelings, which enables children at high risk of mental disorders.
To sum up, it is crucial to acknowledge that future research is needed to build on the shortcoming of this study. The most important limitation lies in the fact that we did the assessment of intellectual functioning only on the basis of the IQ. A further study to assess both IQ and adaptive behaviors is therefore recommended. Moreover, in future investigations, it might be possible to investigate learning profiles of children with low, average, and high intellectual functioning. Another source of weakness in this study is the participants’ age ranging from 8.7 to 9.9 years. This range is small and not necessarily representative of the population of Italian schoolchildren, a factor that may limit the generalizability of the results. Additional research should extend the sample to older students to assess our hypothesis that the gap between intellectual and emotional functioning increases with age.
Nevertheless, challenges and future directions should incorporate research that addresses issues concerning environmental factors and also examine mechanisms mediating family/school sources and children’s temperamental vulnerability to develop maladaptive emotional profiles.
Despite this, our work provides support for the need of a multifaceted approach of study considering simultaneously intellectual and emotional functioning. To our knowledge, the literature is lacking on the relationship between intellectual levels, anxiety, and depression in school-age children. This is an intriguing one, which could be usefully explored in further research.
Implications
The evidence from this study suggests the importance of the prevention programs aimed at identifying at an early age high-risk cases showing increased levels of depression and anxiety in children with lower or higher levels of intellectual functioning. These programs would result in positive significant effects to limit or reduce anxious or depressive behaviors and to prevent mental health problems or personality dysfunctions in adulthood (Allison, Nativio, Mitchell, Ren, & Yuhasz, 2014; Cuijpers, Van Straten, Smits, & Smit, 2006; Jacobson & Newman, 2014). Generally, the intervention programs aim to train coping and problem-solving strategies to face controllable and uncontrollable problems and reduce the risk of high anxiety by favoring the self-regulation and the management of stressful school situations. Indeed, school is the ideal context to provide preventive interventions to a large number of children before a disorder occurs in full scale. One of the most valued preventive programs is the FRIENDS for Life program. It is a short cognitive-behavioral intervention, delivered by classroom teachers, and aimed to reduce both anxiety and depressive symptoms (Ahlen et al., 2012).
It is of worth to note another intervention program combining educational and clinical approaches. This is the cognitive-behavioral therapy (CBT)–based training. It is a program based on coping and problem-solving strategies to reduce cognitive maladaptive strategies in schoolchildren aged 9 to 10 years. This program is delivered in classroom by teachers previously trained by school psychologists. The effective findings highlight the importance to associate appropriate educational and clinical interventions.
More specifically, Shaw (2008) postulated the necessity to improve the education of students with BIF. The author planned an educational program aimed at developing the instructional practices to improve resilience skills. In turn, these skills allow pupils with BIF to cope with emotional and behavioral dysregulation as well as problematic social functioning.
Second, parental intervention programs are needed. Poor parenting profiles were often referred (Fenning, Baker, Baker, & Crnic, 2007). Specifically, mothers of children with BIF were found to be less positive and sensitive than mothers of typically developing children as well as lacking of explanatory models for their children’s difficulties.
However, the education of gifted children necessitates special programs and adapted school curricula able to adequately stimulate the cognitive abilities of these pupils. The Personalized Model of Education for Gifted Children is an appreciated educational program, which takes into consideration the psychological and behavioral characteristics of gifted children (Kelemen, 2010). It is a program to control and reduce emotional and environmental risk factors, which may cause underachievement and social-emotional maladjustments. The goal is to develop an autonomous personality and improve the level of self-esteem resulting in the prevention of maladaptive self-awareness, perfectionism, and social isolation (Majid & Alias, 2010).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.