
Abstract
The Republic of South Sudan continues to face considerable challenges in meeting maternal, newborn and child health (MNCH) care needs and improving health outcomes. Ongoing instability and population displacement undermine scope for development, and damaged infrastructure, low coverage of health services, and limited government capacity and a human resource base have resulted in a fragmented health system. Despite considerable attention, effort and support, the issues and challenges facing South Sudan remain deep and sustained, and urban–rural disparities are considerable. There is a need to maintain investments in MNCH care and to support developing systems, institutions, and programs. This review of the literature offers a commentary and appraisal of the current MNCH situation in South Sudan. It explores the barriers and challenges of promoting MNCH gains, and identifies priorities that will contribute to addressing the Millennium Development Goals and the emerging health priorities for the post-2015 development agenda.
Keywords
Introduction
Maternal, newborn and child health (MNCH) has received substantial international attention and is high on global health and development agendas. Investing in MNCH is recognised as contributing to poverty reduction, economic growth and productivity, and more stable societies (Singh, Darroch, Ashford, & Vlassof, 2009). Poor MNCH remains a significant problem in many low- and middle-income countries (LMICs) and poses a significant gap to achieving the Millennium Development Goals (MDGs). This review and commentary on the literature focuses on South Sudan, a country that continues to face considerable challenges in meeting MNCH care needs and improving health outcomes. Drawing on both gray and published literature, it provides an overview of the MNCH situation in late-2014, and seeks to bring together available information on the MNCH-related challenges facing South Sudan’s people and systems.
Framing Maternal and Child Health Within the Millennium Development Goals
Of the eight MDGs, set in 2000 with a 2015 end-point, three are specifically focused on health: MDG 4—Reduce Child Mortality, MDG 5—Improve Maternal Health, and MDG 6—Combat HIV/AIDS, Malaria, and other Diseases. Explicit attention to MNCH prompted many global initiatives, including the Partnership for Maternal, Newborn, and Child Health (PMNCH) hosted by the World Health Organization (WHO) and UNICEF and established in 2005 (PMNCH, 2013), and the Countdown to 2015 for Maternal, Newborn, Child Survival. Recognizing the need for a global strategy, United Nations (UN) Secretary General Ban Ki-moon launched “Every Woman, Every Child” in 2010, which set out the key areas requiring action to mobilise financing, strengthen policy, and improve service delivery (PMNCH, 2010).
The MDG 2015 target date has sparked global debate surrounding what should follow. The UN-led global consultation on health from October 2012 to February 2013 led to a report on Health in the post-2015 period. Among a range of proposals that included a focus on universal health coverage, the determinants of health and the unfinished MDG agenda, was also recognition of the significant challenges posed by conflict to improving health in many countries (The World We Want, 2013).
Discussions around health on the post-2015 agenda identified “the unfinished MDG health agenda; a changing agenda for global health; and health in the context of sustainable development” (UNAIDS, UNICEF, United Nations Population Fund [UNFPA], & WHO, 2012). Schweitzer, Makinen, Wilson, and Heymann (2012) recommend “the current MDGs are likely to have to be included in some form in the post-2015 goals” (p. 9). Critique surrounding the globally set quantifiable metrics and targets associated with the MDGs are balanced with recognition that the ability to have some form of targeting and universally agreed goals is of value.
MDGs 4 and 5 are closely related, and have seen considerable gains in the health status of women and children, with under-five and maternal mortality rates falling by nearly 50% in recent years (Horton, 2012; UN, 2012). Despite this, neither goal will be met for most countries, and where progress has been made, this is often unequally distributed (UN, 2012), with disparities evident in health status and the coverage of health interventions between and within countries (Bhutta et al., 2010).
Accelerating progress requires adopting an integrated package of essential interventions, structured around a continuum of care approach, with services delivered by functioning health systems (PMNCH, 2011). Evidence-based interventions are well-known (PMNCH, 2011) and feasible in resource-poor settings (Lule et al., 2005; You, New, & Wardlaw, 2012). Despite knowledge of effective and appropriate interventions, ensuring universal access to essential health services remains challenging in LMICs.
Maternal and Child Health Millennium Development Goals in Sub-Saharan Africa (SSA)
The SSA region has the highest rates of neonatal, under-five, and maternal mortality. Neonatal mortality sits at 35 deaths per 1,000 live births and has seen the least improvement over the last 20 years. Although the average rate of reduction of under-five deaths doubled from 1.2% per year (1990-2000) to 2.4% per year (2000-2010), the overall mortality rate is still high at 121 deaths per 1,000 live births. The rate of decline is insufficient to meet the target of a two-thirds reduction set through the MDGs. Similarly, although maternal mortality has nearly halved globally since 1990, the global target of reducing the maternal mortality ratio (MMR) by three quarters is unlikely to be achieved by 2015, particularly in SSA, the region with the highest MMR (500 deaths per 100,000 live births) and where 56% of all maternal deaths occur (UN, 2012).
“Post”-Conflict Maternal and Child Health Challenges
Health in fragile and conflict-affected states is handicapped by the legacy of violence on society, systems, and economic development. Such states are often characterised by “economic volatility, political instability, infrastructural collapse and human resource scarcity,” all of which contribute to the deterioration of population health and challenges in stabilising systems (Haar & Rubenstein, 2012, p. 289). Haar and Rubenstein (2012) cite evidence of worsened health status and challenges in establishing stable health systems in fragile and conflict-affected states as compared with their geographic neighbors and economic equivalents. Bornemisza and Zwi (2008) highlight the dearth of health systems research in fragile and conflict-affected states, despite the longstanding recognition of the impact of conflict on health systems (Zwi & Ugalde, 1989a, 1989b). By 2012, no fragile or conflict-affected state had achieved a single MDG (Wyeth, 2012).
MNCH often deteriorates during a period of conflict. In addition to poor health outcomes resulting from violent conflict and its effects on the health system, “girls and women are particularly at risk as they are less likely to be able to protect themselves from violence” (Southall, 2011). Infants and children experience heightened risk of communicable diseases, physical and mental trauma, and developmental disorders as compared with their non-conflict-affected counterparts (Bustreo, Genovese, Omobono, Axelsson, & Bannon, 2005). Women and girls are at a greatly increased risk of sexual and other forms of gender-based violence and the associated risks to physical and psychosocial health and well-being (Southall, 2011).
Objectives of the Article
This article focuses on South Sudan and brings together available information on MNCH in late 2014, highlighting the ongoing challenges facing its systems and people. We undertook a narrative review, drawing on a range of databases such as Medline, Embase, and Google Scholar, to identify relevant peer-reviewed and gray literature. We drew on these data and insights to reflect on what is known about the MNCH situation in South Sudan, and its relationship to conflict and health system development. Although admittedly not fully comprehensive, we draw on available evidence to synthesise the issues being faced and contribute to debates around South Sudan development prospects, including the 2015 MDG deadline.
South Sudan Background and Health System
South Sudan general background
The Republic of South Sudan is the world’s newest nation, gaining independence in 2011 (Karimi, 2011). Its capital and largest city is Juba, located in the southern state of Central Equatoria (Wakabi, 2006). The population of South Sudan in 2008 was 8.26 million (South Sudan National Bureau of Statistics, 2012). It is a land-locked country, bordered by Ethiopia, Kenya, Uganda, the Democratic Republic of the Congo, the Central African Republic, and Sudan (South Sudan National Bureau of Statistics, 2012).
Although both Sudan and South Sudan are rich in natural resources, South Sudan in particular has an abundance of natural resources and contains the majority of oil reserves. Although this has the potential to contribute to economic growth and poverty reduction, giving South Sudan a major advantage over many “post”-conflict 1 governments (National Population Council, 2010), it is also a source of ongoing conflict and instability—the so-called “resource curse” (Mbaku & Smith, 2012), as witnessed again in 2013 and 2014.
After 21 years of civil war in Sudan, the signing of a Comprehensive Peace Agreement (CPA) between the Government of Sudan and the Sudan People’s Liberation Movement/Army (SPLM/SPLA) in January 2005 brought an end to Africa’s longest running conflict between the North and South (UNFPA, 2006). Six years later, the Republic of South Sudan declared independence on 9 July 2011 (Embassy of the Republic of South Sudan in Washington, 2011; Karimi, 2011). A timeline of major political developments in South Sudan from 1956 to date highlights ongoing instability (Table 1).
South Sudan—Timeline and Chronology of Major Political Developments.

Source. (BBC News, 2015).
Background to South Sudan health system
Damaged infrastructure, limited human resources, weak stewardship, and a proliferation of non-government organisations (NGOs) characterise health systems in many countries emerging from conflict, and lead to disrupted and fragmented delivery of health services (Roberts, Guy, Sondorp, & Lee-Jones, 2008). In South Sudan, two decades of civil war resulted in a largely dysfunctional health system and contributed to the deteriorating health status of the population during and after the conflict (Neuse, Davis, Masbayi, Harvey, & Rajkotia, 2008), leaving a third of the population without access to adequate health services (Rajkotia, Boulenger, & Pressman, 2007). The health status of the population is marked by high health needs, limited health service provision, and significant urban–rural and regional disparities (Roberts, Damundu, Lomoro, & Sondorp, 2010).
The Ministry of Health (MoH) operates in line with the decentralisation policy of the interim constitution of South Sudan (2005) and the Local Government Act (2009). According to the “Health Sector Development Plan 2011-2015,” the decentralised organisational structure should be based on four levels of administrative structure: central, state, county, and community (MoH & Government of South Sudan [GoSS], 2011), as shown in Figure 1 and outlined below. However, the reality on the ground shows many functions underdeveloped, particularly at the lower levels.

Ministry of Health organisational structure.
It is envisaged that the Central MoH will provide policy guidance, leadership, and funds for services, and is responsible for monitoring and evaluation. The State MoH, located in each state capital, is responsible for annual management work plans, joint assessments, planning, monitoring and evaluation, the referral system, and implementation of government health care and services. The County MoH should oversee monthly management work plans, joint strategic planning based on local needs, assessment and analysis of local health and managerial needs, supervision, guidance and monitoring, the referral system, and implementation of health care and services. The Community MoH (Primary Health Care Units and Centers) should ensure implementation of the Basic Package of Health Services (BPHS), weekly work plans, outreach activities, the referral system, and community participation (Rajkotia et al., 2007).
The BPHS outlines a package of health care services that should be affordable and accessible to the majority of the population, at the primary and secondary health care levels. It covers curative, promotive, preventive, and managerial activities (MoH & GoSS, 2011). Combined contributions from the GoSS and the Multi-Donor Trust Fund (MDTF) initially allowed for the provision of the BPHS (Health Systems for Outcomes, 2009); however, according to the Health Sector Development Plan 2011-2015, NGOs are often the primary providers (MoH & GoSS, 2011).
The functioning of health care services within South Sudan is described by the MoH (MoH & GoSS, 2011) as structured around four key levels: community, primary, secondary, and specialised care, linked by a referral system. Community health care should be provided by community health workers, maternal and child health workers, and home health promoters. Primary health care units are meant to be the first point of contact between communities and the health system and should provide basic preventive, promotive, and curative care for around 15,000 people. These units aim to provide higher-level services for around 50,000 people and, in addition to services offered by primary health care units, provide basic diagnostic laboratory services and maternity care. County hospitals and state hospitals should provide secondary-level care, including comprehensive obstetric care, in-patient care, and surgery, for around 300,000 and 500,000 people, respectively. Numerous gaps and challenges are encountered at each of these levels, however, particularly in equipping and strengthening them to reach even minimum standards (MoH & GoSS, 2011).
Health indicators
More than 50% of the South Sudanese population lives below the poverty line, with particularly high levels of poverty in rural areas (South Sudan National Bureau of Statistics, 2012). This is comparable with the SSA average of 47% of people living on less than $1.25 a day (UN, 2012). The adult literacy rate in South Sudan is also low at just 27% (53% urban areas and 22% rural areas) with the rate among females half that of males (South Sudan National Bureau of Statistics, 2012). Minimal progress has been made toward meeting the MDG targets (Mustafa & Alsiddiq, 2007; WHO, 2009). The GoSS is working toward achieving these goals, but has argued it will require time beyond 2015 (GoSS, 2011). Maternal, newborn, and child mortality indicators used for monitoring progress toward the achievement of MDGs 4 and 5 remain high (Table 2). Mortality rates and other indicators are also presented below. Data vary considerably by place of residence, mother’s education, gender, and wealth index, although data classified according to these determinants are not always available.
South Sudan—Key Indicators/Trends in Maternal, Newborn, and Child Health (2000-2010).
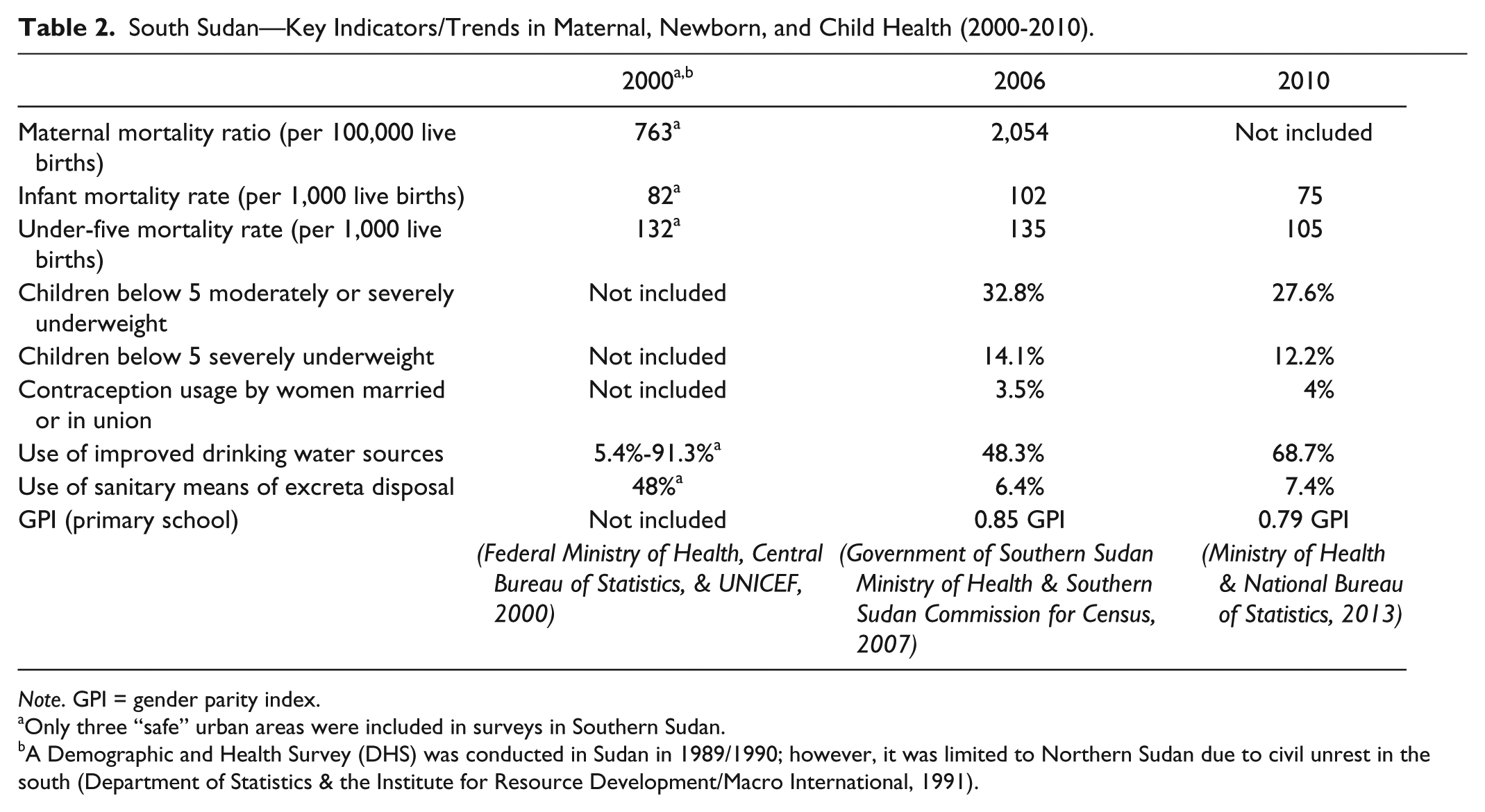
Note. GPI = gender parity index.
Only three “safe” urban areas were included in surveys in Southern Sudan.
A Demographic and Health Survey (DHS) was conducted in Sudan in 1989/1990; however, it was limited to Northern Sudan due to civil unrest in the south (Department of Statistics & the Institute for Resource Development/Macro International, 1991).
In South Sudan, nearly 7% of women aged 15 to 49 marry before their 15th birthday, a substantial reduction from 16.7% in 2006. However, 45% still married before the age of 18 in 2010, which is an increase from the 2006 average of 41% (MoH & National Bureau of Statistics, 2013). Young women experience exacerbated problems during pregnancy and delivery due to incomplete body growth (Bearinger, Sieving, Ferguson, & Sharma, 2007), and are particularly at risk of obstetric fistulae and obstructed labor.
In 2010, the average rate of contraception use for women married or in union in South Sudan was 4%, only 0.5% higher than in 2006 (MoH & National Bureau of Statistics, 2013). This can be compared with 8% in Sudan as a whole (including Southern Sudan at that time; GoSS MoH & Southern Sudan Commission for Census, 2007) and 25% in SSA (UN, 2012). Access to family planning is strongly linked to gender equity, empowerment of women, education, and employment, and is a vital component to saving lives and preserving health through preventing untimely and unwanted pregnancies (Cleland et al., 2006; Grown, Gupta, & Pande, 2005; Prata, Sreenivas, Greig, Walsh, & Potts, 2010; United Nations Children’s Fund, 2012). Polygamy and polygyny are common in South Sudan, with 41% of all unions in 2010 being polygynous. Fewer than 10% of those in polygamous unions use safe sex practices (MoH & National Bureau of Statistics, 2013).
In Sudan (including Southern Sudan) in 2006, 36.4% of women received antenatal care (ANC) from a medical doctor, 12.7% from a nurse or midwife, and 14.5% from a traditional birth attendant. This contrasted with Southern Sudan at the same time, where only 9.8% of women received ANC from a medical doctor, 16.4% from a nurse or midwife, and 28.6% from a traditional birth attendant (GoSS MoH & Southern Sudan Commission for Census, 2007). Thus, only 26.2% of women in Southern Sudan received ANC by skilled health personnel in 2006; this increased to 40.3% in 2010; however, only 17% of women had the recommended 4 or more ANC visits (MoH & National Bureau of Statistics, 2013). Pregnancy outcomes in LMICs can be greatly improved through ANC (WHO, 2005).
The majority of maternal deaths occur during labor, delivery, and the immediate post-partum period, and as most are preventable, it is essential that a skilled health professional be available during childbirth. In Sudan as a whole, 49% of births were delivered by skilled personnel in 2006: doctors (6%), nurses or midwives (17%), and auxiliary midwives (26%). These figures are substantially lower in the states of Southern Sudan, with only 4% of deliveries being delivered by a doctor and 7% by nurses and midwives. In both Northern and Southern states, in 2006, traditional birth attendants assisted with 20% of births (GoSS MoH & Southern Sudan Commission for Census, 2007), which increased to 34% in South Sudan in 2010 (MoH & National Bureau of Statistics, 2013). In 2006, friends and family assisted in 16% of births in the North and 36% in the South (GoSS MoH & Southern Sudan Commission for Census, 2007).
The postnatal period is critical for mothers and newborns as they are at the highest risk of death during delivery and in the first hours and days following childbirth. Newborn survival is inextricably linked to the health and survival of the mother; thus, the early postnatal period is an important period for delivering integrated interventions to both. Postnatal care services from a skilled health care provider following delivery optimise mother and newborn health, promote healthy behaviors and healthy household practices, and strengthen linkages between maternal health and child health programs (Sines, Syed, Wall, & Worley, 2007). Data on the postnatal period in South Sudan appear to be scarce.
A child born in South Sudan has a 25% chance of dying before age five(WHO, 2009); high mortality in under-fives is associated with pneumonia, malaria, and diarrheal diseases. Malnutrition is common: 27.6% of children below five are moderately or severely underweight and 12.2% severely underweight (MoH & National Bureau of Statistics, 2013). South Sudan has one of the lowest levels of immunisation in the world (UNICEF, 2011), with some sources suggesting this has deteriorated over the past five years, whereas others suggest this results from variations in data collection and sampling. In 2010, only 4.3% of children aged 12 to 23 months had vaccination cards available, compared with around 13% in Southern Sudan in 2006. Measles vaccination coverage differed little between 2006 and 2010 (27.7% vs. 26.3%, respectively), as did the proportion of children who received all recommended vaccinations (2.7% in 2006 vs. 2.6% in 2010; MoH & National Bureau of Statistics, 2013).
Health System Influences and Challenges in South Sudan
The line between acute humanitarian intervention and longer-term health development in South Sudan is blurred (Cometto, Fritsche, & Sondorp, 2010; Downie, 2012), as in many “post”-conflict and fragile states (see, for example, Macrae, Zwi, & Gilson, 1996). Recurring bouts of violence and political instability make transitioning from humanitarian service provision into national development challenging for government officials, development partners, and citizens. Decades of humanitarian assistance “fragmented horizontally a variety of actors (at least 76 NGOs and six UN agencies) and vertically across multiple disease-specific control programmes” coupled with costly, short-term and inefficient operations, severely impeded the development of institutions, systems, policies, and personnel to contribute to longer-term development in Southern Sudan (Cometto et al., 2010). Post-independence optimism was shattered by the government’s decision to halt oil production in January 2012, hindering both planned health system development and damaging relationships with external donors (Green, 2012).
A broad set of issues have an impact on effective development and are briefly described below.
Governance
Throughout the period of conflict and immediately following the referendum, governance in Southern Sudan was absent or constrained by the low capacity of government and lack of personnel. Initiatives aimed at improving governance following the referendum had mixed results (Bennett et al., 2010), although the launch of the Health Sector Development Plan in early 2012 provided an opportunity to facilitate improvement. Governance and implementation arrangements are coordinated by development partners, usually in collaboration with South Sudan’s MoH. Despite the MoH demanding greater ownership, some concern around the level of “fiduciary and governance risks” remains (Australian Agency for International Development [AusAID], 2012). The lack of personnel skilled in policy, planning, and oversight presents a serious challenge for governance (Downie, 2012).
Security
Localised conflicts remain in South Sudan, due in part to disputes over border areas and oil-revenue sharing (the British Broadcasting Corporation [BBC] News, 2014; GoSS, 2011; Maxwell, Gelsdorf, & Santschi, 2012; United Nations High Commissioner for Refugees [UNHCR], 2013; UNICEF, 2011). Widespread conflict broke out in South Sudan in December 2013, leading to thousands of deaths and the displacement of more than half a million people before a ceasefire was signed between the government and rebels on January 23, 2014 (Whiting & Migiro, 2014). By late 2014, tensions remained high, and over 1.9 million people were reported to be displaced since December 2013, of whom 1.4 million were displaced internally (Office for the Coordination of Humanitarian Affairs, 2014).
South Sudan also continues to experience other ongoing conflicts and security challenges, including intertribal conflicts, widespread landmines and unexploded ordnance, influx of returnees, and natural disasters. Years of conflict contributed to the disintegration of social fabric, leading to decreased protection and conditions exposing people to high levels of violence and exploitation (UNICEF, 2011).
Landmines and unexploded ordnance (UXO) pose a continued threat to communities in South Sudan, despite growing awareness and control efforts (GoSS, 2011). The National Mine Action Authority, which oversees relevant activities in South Sudan, and other associated organizations have increased the awareness of nearly two million people concerning mine risks and have removed more than 50,000 landmines and UXOs (UN Mission in South Sudan, 2013).
South Sudan also faces a degree of internal insecurity resulting from the return of refugees from camps in other countries of Africa, refugees fleeing to South Sudan from conflicts elsewhere in Africa, and growing numbers of internally displaced people (IDP) due to ongoing instability. The number of IDPs remained high in 2013 (UNHCR, 2013).
In addition to experiencing prolonged conflict, South Sudan is also prone to natural disasters; a National Baseline Household Survey conducted in 2009 found that 56% of the population suffered from drought or floods (GoSS, 2011).
Funding/international aid environment
In the presence of recurrent violence and instability in South Sudan, several key funding programs were ended simultaneously and replaced by less generous programs (Downie, 2012). The MDTF, which had covered several key health initiatives in South Sudan, was operationally closed on December 31, 2012, and financially closed at the end of June 2013 (Independent Evaluation of the Multi-Donor Trust Fund for South Sudan [MDTF-SS], 2013). The MDTF marshalled the financial resources of several external donors, but concerns regarding ongoing funding remain. The MDTF contributed to establishing and strengthening state institutions and expanded public services and delivery. One identified problem was the transition from the Rapid Impact Emergency Project (RIEP) to more sustainable services and systems (Independent Evaluation of the MDTF-SS, 2013).
South Sudan was due to receive a US$130 million credit from the World Bank Group’s Fund for the poorest countries, the International Development Association (IDA; World Bank, 2013), as well as funding and support from several other sources including United States Agency for International Development (USAID) and Department for International Development, UK (DFID; MoH, n.d.). It was hoped that some oil revenues would also be directed to MNCH, given its focus within the National Health Plan (Downie, 2012; Rai, Ramadhan, & Tulchinsky, 2012). Adequate levels of sustained funding are vital to improving health outcomes (Zwi, 2011).
To better coordinate health service delivery between the ranges of stakeholders in South Sudan, a “division of labour” has been implemented, based on geographical coverage among three key health development partners: USAID, DFID, and the World Bank. Stakeholders involved in the financing and provision of health services in South Sudan include health development partners, international NGOs, national NGOs, faith-based organisations, and the private sector (MoH, n.d.).
Coordination, fragmentation, and aid effectiveness
Before independence, health assistance to South Sudan was characterised as being “supply driven” (Downie, 2012, p. 11). Like many conflict-affected states, development partners and NGOs provided fragmented services suited to their own interests, covering selected regions. Fox and Manu (2012) suggest that coordination by the major development partners in South Sudan improved following a geographic division of responsibility for health assistance among development partners.
Promoting aid effectiveness is a significant issue given prior history of fragmentation and poor coordination. Global attention to development effectiveness has led to attention being focused on issues such as national ownership, mutual accountability, transparency, and coordination—all relevant to more effective aid. Debates concerning this broader aid and development context simultaneously offer guidance and place pressure on both the South Sudanese government and its development partners to promote better practice.
South Sudan is a founding member of the g7+, an intergovernmental organization of “fragile” and “post”-conflict states. It draws on the New Deal for engagement in fragile states, a declaration concerning how best to progress development in the least developed states with the support of the international community (Dyori, n.d.). The New Deal (g7+, 2011) offers guidance on engagement between fragile states and their development partners, and specifically sets out objectives concerning the achievement of five peace- and state-building goals as the foundation for progressing the MDG targets. These include promoting “legitimate politics,” security, justice, economic foundations, and revenues and services. South Sudan is piloting the New Deal and completed its first fragility assessment in late 2012, the first element of the “pathway out of fragility” (Ministry of Finance and Economic Planning, 2012).
Maternal and Child Health Service-Related Challenges
Access
Delays in seeking medical care are a significant factor contributing to maternal deaths (Geller, Cox, Callaghan, & Berg, 2006; Mathai, 2008), and women with obstetric complications in LMIC, such as South Sudan, face numerous barriers to access (Barkat, Rahman, Bose, Com, & Akhter, 1997; Mbaruku, van Roosmalen, Kimondo, Bilango, & Bergström, 2009), as outlined below.
Geographical
Pregnant women in South Sudan often experience considerable time delays when trying to reach a health facility for treatment (Karoshi & Keith, 2009; Sivaganesh & Senarath, 2009). Geographic barriers impede women with obstetric complications from accessing emergency obstetric care (Borghi, Ensor, Somanathan, Lissner, & Mills, 2006). Access is generally worse in rural than urban areas, and 83% of the population in South Sudan is rural (South Sudan National Bureau of Statistics, 2012). Women in South Sudan may travel long distances by foot to reach health centers (Murphy, 2007), as many villages do not have road access and families do not have access to vehicles or public transportation. It may take literally days for women with life-threatening conditions to reach a health care facility; many women die from treatable complications.
Financial
The cost of receiving health care is another major constraint in South Sudan, due to the need for transportation, physician and facility fees, and the cost of medications and other medical supplies (Borghi et al., 2006). Pregnant women may be seen by community members as a “burden” due to the high costs, often unaffordable by families, associated with childbirth. The government has committed to free services in the public sector (GoSS, 2011); however, under-the-counter payments have been reported, which will require ongoing monitoring (Rajkotia et al., 2007), and, as in other settings, time lost seeking money to pay for care may delay access to crucial services and lead to loss of life (Lewis, 2003; Prata et al., 2010).
Cultural and Social
At a global level, achieving the MDG targets relies heavily on women’s empowerment and equal access to education, work, health care, and decision making, yet MDG 3, concerning the promotion of gender equality and empowerment of women, remains largely unfulfilled (UN, 2012). Women in rural areas often do not have the power to seek, receive, or communicate around health issues, including information that can help prevent maternal mortality such as safe abortion, family planning, and antenatal care (Lewis, 2003). Girls continue to be discriminated against with respect to education at all levels, yet education enables women to gain the knowledge, confidence, skills, and opportunities to increase their social and economic status in their household and in society (Gill, Pande, & Malhotra, 2007). Educated women have better health outcomes; for each additional year of education achieved by 1,000 women, two maternal deaths will be prevented (World Bank, 2002).
Gender inequalities and discrimination lie at the root of child marriage, common in South Sudan. The most recent Household Health Survey indicated that 7.3% of girls are married before 15 years of age, and 45.2% before 18 (MoH & National Bureau of Statistics, 2013). Early marriage has harmful consequences associated with risks of pregnancy, sexual violence, and sexually transmitted infections including HIV. Pregnancy and delivery are particularly dangerous for adolescents, who have a five times greater risk of dying in childbirth than women in their 20s (WHO &UNFPA, 2006).
The contraceptive prevalence rate among married women or those in other unions is particularly low in South Sudan, reflecting the high levels of illiteracy and lack of education about reproductive health and family planning (Rajkotia et al., 2007; WHO, 2009). Even with education opportunities, women, and especially adolescents, often lack access to consistently and appropriately stocked family planning services and distribution points (Aquilina et al., 2006). South Sudan has high fertility rates, estimated at 6.7 births per woman (MoH, 2011), which exacerbate the high risk of maternal death (MoH & National Bureau of Statistics, 2013; New Sudan Center for Statistics and Evaluation & UNICEF, 2004).
Gender inequality is also high in South Sudan, and gender-based violence widespread (Learning on Gender and Conflict in Africa, 2012; World Bank, 2013). The Independent Evaluation of the MDTF-SS (2013) found that gender inequality was not a Task Force priority during initial implementation phases, and it was not until 2009 that it received proper attention. Addressing gender inequalities has now been identified as a key priority in South Sudan (GoSS, 2011; MoH & GoSS, 2011).
There are many forms of traditional practice in South Sudan, and much health-seeking behavior relates to traditional medicine. Traditional healers are often sought due to personal beliefs, or because no other means of health care is available or accessible (MoH, 2009). According to the National Baseline Household Survey 2009, 47% of the household population in South Sudan that does not have access to a health care facility seeks help from traditional healers (South Sudan National Bureau of Statistics, 2012). South Sudan is home to more than 60 ethnic groups (Jok, 2011; Kimenyi, 2012), held together primarily by their shared struggle and collective opposition to the north (Jok, 2011). Health-seeking behavior in general, and for these varied groups, remains inadequately understood (MoH & GoSS, 2011; National Population Council, 2010), and a key objective of the 2011-2015 Health Sector Development Plan is to improve access to, and the delivery of, quality primary health services through, among other things, mobilising the community around appropriate health care seeking (MoH & GoSS, 2011).
Applying multi-faceted concepts of access to primary health care, as elaborated by Levesque, Harris, and Russell (2013), will be helpful in identifying enablers that should be supported and barriers that need to be addressed.
Health facilities and human resources for health
Human resources for health (HRH) play a pivotal role in the availability, accessibility, and equity of health services. The availability of skilled birth attendants able to detect, prevent, and manage obstetric complications as well as to provide drugs, equipment, and other supplies is the single most important factor in preventing maternal deaths (Rosenfield & Schwartz, 2005). South Sudan’s health worker density is far lower than the minimum threshold recommended by the WHO (Gupta et al., 2011). In 2009-2010, there were a reported total of 189 physicians across 8 states (a doctor/population ratio of 1:65,574) and 309 midwives (a midwife/population ratio of 1:39,088; MoH, 2010). Figures vary however, with other sources suggesting 1 midwife for every 125,000 women (Kolok, 2013).
South Sudan has experienced a critical shortage of skilled human resources in all sectors, including health (MoH & GoSS, 2011). Development of institutional and human resource capacity is a stated government priority (MoH, 2010), and although innovative training of frontline health workers has commenced, considerable constraints remain (Fehling et al., 2013).
Even when women do have the means of reaching a health service, inadequate numbers of high quality services and facilities (and insufficient numbers of qualified personnel to staff the services) can increase delays and raise the risk of maternal mortality. Delays can occur when facilities do not have the capacity to perform basic services, which can put women with emergency complications at heightened risk of maternal mortality (Karoshi & Keith, 2009). Poor maternal health outcomes in South Sudan are strongly connected to poor prenatal, delivery, and postnatal care services in health facilities (Rai et al., 2012), and inadequate links between the community and the first level of the referral system significantly increase the risk of maternal death for women. Health facilities in South Sudan often also face chronic shortages of medicines and other necessary supplies. Medicines are supplied through the MoH, however transportation to facilities, and storage within these facilities, remains a significant challenge (Ministry of Health & Government of South Sudan, 2011).
Health service providers in “post”-conflict settings need to understand and be sensitive to the differing community perspectives around health and health care, and of the importance of building trust in health services (Zwi, Bunde-Birouste, Grove, Waller, & Ritchie, 2006). They must also be sensitive to historical inequalities, socio-cultural and economic developments, and eroded trust that might be present (Schweitzer et al., 2012).
Discussion
This review has reflected on the widespread MNCH needs and challenges in South Sudan. The civil war fractured social structures, displaced millions of people, destroyed much of the physical infrastructure, and led to the collapse of the public health system, resulting in high morbidity and mortality (GoSS, 2011). Despite efforts by the GoSS and the international community, South Sudan remains far from achieving the MDGs, a major challenge in all “fragile” and conflict-affected states. A broad and comprehensive approach to addressing population-based MNCH is required, along with ongoing support to developing institutions and systems.
Priority Areas
Three priority areas emerge from this narrative review: (a) addressing the macro-political and “post”-conflict security and development context, (b) focusing on the key determinants of health, and (c) building the health system, its capacity, and its capabilities, with the support of the international community. These priorities are interrelated and should be simultaneously considered in addressing MNCH needs, though are discussed separately below.
Macro-political and “post”-conflict security and development context
South Sudan and other “fragile” and “post”-conflict states have shown least progress toward meeting MDG targets and exhibit the most pressing health and development needs. The conflict-to-peace transition and the challenges of nation building are fundamental, requiring deep and sustained commitment by both government and development partners. These are mutually reinforcing—charting a vision for the country’s development and establishing a sense of security and stability along with effective governance are central to securing international community support and engagement.
The debate around the MDG targets and the development goals being formulated for the post-2015 period highlight the search for solutions to some of the most complex development needs. This debate, however, also provides some opportunity and space, in part in association with the g7+ and other “fragile” and “post”-conflict states, to highlight the specificity of their needs alongside their commitment to addressing the development deficit present within their countries. Nascent local civil society, along with engaged global civil society, will play an important part in keeping this debate alive and accountability in focus (The World We Want, 2013).
Key determinants that influence health outcomes
This narrative review highlights the poor health status and MNCH outcomes in South Sudan, and draws attention to the need to address the determinants of health if improved outcomes are to be achieved. Despite the many obstacles and challenges in South Sudan, peace and security, and addressing basic needs of nutrition, shelter, employment, and water and sanitation, among others, require attention. Gender equality, and the education of girls and women, is vital and requires high levels of government commitment and leadership, as “low rates of primary school completion and high gender disparities pose enormous challenges to the development of South Sudan” (UNICEF, 2011). The South Sudan Household Health Surveys of 2006 and 2010 demonstrate that women with more years of schooling have both higher levels of knowledge about health and better health outcomes, as do their families.
The UN-led Consultation on Health in the Post-2015 Agenda emphasised that the most disadvantaged, marginalised, stigmatised, and hard-to-reach populations in all countries must be prioritised, and equity must be made explicit in the post-2015 goals (The World We Want, 2013). This echoes broader calls for the more central role of rights within this agenda and the focus on reducing disparities and inequalities. That report also recognised that the goal of achieving universal health access must improve governance and access to decision making, as well as reduce those barriers that relate to gender, income level, and geography (The World We Want, 2013). Improving upstream interventions must complement those operating through health systems and services.
Improved health system and services
This article brings together an extensive range of insights into health system functioning, performance, and challenges in South Sudan. Ongoing conflict has a detrimental impact on health status and health system development, although considerable efforts are now underway to try and move beyond the “post”-conflict challenges and to consolidate nation building. A major element of this agenda is establishing and maintaining effective services operating within a broader health and development policy with long-term objectives. We have highlighted the key challenges present, with an emphasis on applying what is already known to be effective in improving and securing MNCH outcomes for populations in LMICs. Informing policy with evidence (Bowen & Zwi, 2005) requires acute sensitivity to local context. Applying well-established guidance and policies, building and working with trustworthy and committed development partners, is likely to be an essential component of this long-term effort.
The literature highlights the lack of skilled MNCH service providers as the greatest obstacle to achieving improved MNCH in South Sudan (Nelson et al., 2011), with the majority of births still attended by family or friends rather than a trained provider, and delays in seeking medical care contributing to maternal deaths. Human resources for health are critically low in South Sudan and require ongoing investment and commitment to building institutions. Fujita et al. (2013) examined the role of midwives in addressing high maternal mortality in “post”-conflict Cambodia, and highlighted the importance of political commitment, high level leadership, capable mid-level managers, and supportive development partners, if systems and institutions are to be built on an effective and sustainable basis. These all apply to South Sudan.
The health and humanitarian situation in South Sudan, with particular reference to MNCH, requires substantial financial and technical assistance from the international community (Rai et al., 2012). Rai et al. (2012) indicate that technical support should include establishing good governance practices, creating a conducive environment for pooled funding and programs, and establishing an accountability framework. Zwi (2011) argues that the seven “sins” associated with “aid” funding should be carefully avoided in relation to development assistance for health; these include being patient, being more generous, and committing to longer-term building of institutions. Health systems and services should also take into account general lessons learned; according to the Independent Evaluation of the MDTF-SS (2013), recommendations for successful projects included the following:
strong national leadership;
careful preparation, with realistic development objectives and implementation schedules;
recognition of capacity constraints of national implementing institutions;
avoiding top-down approaches;
integrating risk assessment and mitigation measures into the design; and
establishing a robust field implementation presence, with management oversight, and regular engagement with national counterparts.
The South Sudan health sector development plan (MoH & GoSS, 2011) notes the importance of monitoring, evaluation, and operational research. Enhancing our understanding of context—historical, cultural, political, economic, and developmental—and of current capacity and its constraints will be important to assuring appropriate support and capability strengthening.
Post-2015 Agenda
Several issues reflected in the Thematic Consultations for the post-2015 development agenda are acutely relevant to South Sudan: the need to focus on health and related inequalities and disparities, the importance of recognising specific contexts such as conflict and fragility, the centrality of universal health coverage, and the associated right to health. Innovations on the ground and the role of civil society and responsiveness to the community also receive attention.
The Thematic Consultation highlighted the importance of gender equality, accountability, and sustainability as guiding principles for the new development agenda. It argued that MDG health priorities would continue to feature in the post-2015 agenda given the importance of women’s and children’s health, HIV, and other infectious diseases especially in SSA (The World We Want, 2013). A DFID evaluation of the Basic Services Fund in South Sudan (Johnson, Ockelford, & Power, 2013) found that gender equity had not been sufficiently highlighted; addressing this gap will be core to enhancing health and development. The post-2015 development framework should be more “people-centred and rights-based . . . ” with goals and indicators with “universal relevance . . .", while highlighting the importance of country context (The World We Want, 2013).
Conclusion
This narrative review has sought to contextualise the MNCH challenges in “post”-conflict South Sudan. We have highlighted ongoing constraints, barriers, and impediments to improving health outcomes across the MNCH continuum. We draw attention to these within the broad context of international community support to “post”-conflict states and have highlighted opportunities arising as a result of South Sudanese independence, commitment to the MDGs, debates around the post-2015 development agenda, and the emergence of the g7+, which allows South Sudan to engage with its peers and develop shared objectives and frameworks for nation building.
We emphasise a number of core challenges that remain—securing the peace and building macro-economic and political stability; addressing the determinants of health; and building services and systems that are attuned to the realities on the ground. Much remains to be done, however, and sustained, multi-layered, and dependable support are required if advances for MNCH are to be achieved in South Sudan.
Footnotes
Authors’ Note
This article was developed from an earlier piece of work by N.M. supervised by A.Z. J.B. undertook the search for updated literature, assisted by C.S. and N.M. J.B. and A.Z. prepared major revisions of text and subsequent drafts. A.Z. led the team at all stages of the project. All authors approved the final submitted version of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.