
Abstract
Treatment of substance use/misuse (SUM) continues to pose a difficult challenge. This exploratory pilot study evaluated whether a novel mind–body intervention program called “Mind–Body Bridging” (MBB) could be an effective short-term adjuvant intervention for managing SUM and coexisting symptoms in women undergoing residential and outpatient substance use treatment in a community setting. Thirty-eight women attending a local substance abuse (SA) facility were recruited and randomly assigned to either (a) treatment as usual (TAU) or (b) MBB and TAU. The MBB program consisted of 20 sessions and lasted for 10 weeks. Participants were asked to complete a set of self-report questionnaires designed to assess drug/alcohol cravings, impact of past trauma, depression, sleep disturbance, mindfulness, self-compassion, and well-being. They completed the questionnaires at three time points: preintervention, midintervention (after the fifth week), and postintervention. MBB + TAU significantly reduced drug/alcohol cravings, trauma-related thinking, and disturbed sleep in comparison with TAU. Furthermore, MBB + TAU significantly increased mindfulness, self-compassion, and well-being in comparison with TAU. MBB for SUM appears promising as a complementary adjuvant intervention, warranting future larger scale randomized controlled trials of MBB for SUM populations. SUM is a difficult condition to treat and manage clinically, especially given the multiple comorbid conditions that frequently affect those with SUM. In the search to develop effective adjuvant interventions for SUM, the present pilot study suggested that adding MBB to standard SUM treatment in community-based settings could enhance therapeutic efficacy and quality of care.
Introduction
The incidence of substance use/misuse (SUM), ranging from alcohol abuse to the use of illegal drugs, is relatively high in the U.S. general population (Hasin & Keyes, 2011; Merikangas & McClair, 2012). In women suffering from domestic violence, sexual abuse, and trauma, prevalence of substance abuse (SA) is even higher and is frequently associated with mental health conditions, including depression, anxiety, mood disorders, and posttraumatic stress disorder (PTSD)–like symptoms (Dass-Brailsford & Myrick, 2010; Hides, Samet, & Lubman, 2010). The use of illegal substances and/or alcohol in these individuals is believed to be associated with dysfunctional coping strategies to help individuals deal with their difficult experiences (Broadus, Hartje, Roget, Cahoon, & Clinkinbeard, 2010). To account for this presumed connection, a self-medication hypothesis has been proposed to clarify the relationship between emotional states and drug use (Hall & Queener, 2007; Khantzian, 1985, 1997). Clearly, women with SUM problems are in critical need of effective interventions to help them recover from SUM and deal more effectively with their difficult circumstances.
Treatment of those with SUM is often complex, requiring a comprehensive approach that also addresses coexisting conditions such as PTSD, depression, and anxiety. The present study investigated a new mind–body intervention to ascertain its usefulness for improving not only SUM-related measures (such as cravings and drug use consequences) but also the coexisting symptoms frequently associated with SUM.
Mindfulness-based intervention (MBI) is a general term for mind–body interventions that focus on the power of “mental training” in regulating mental and physical health conditions (Begley, 2007). The category of MBI includes Mindfulness-Based Stress Reduction (MBSR; Kabat-Zinn, 1991) and Mindfulness-Based Cognitive Therapy (MBCT; Teasdale et al., 2002; Teasdale et al., 2000). These MBIs and other similar programs have been found to be effective management programs for chronic medical conditions and mental illnesses (Bohlmeijer, Prenger, Taal, & Cuijpers, 2010), as well as SA (Bowen & Enkema, 2014; Bowen & Marlatt, 2009; Bowen et al., 2006; Brewer et al., 2011; Brewer et al., 2009; Davis, Fleming, Bonus, & Baker, 2007; Davis, Goldberg, et al., 2014; Davis, Manley, Goldberg, Smith, & Jorenby, 2014; Garland, Gaylord, Boettiger, & Howard, 2010; Garland et al., 2014; Zgierska et al., 2009). A recent systematic review (Chiesa & Serretti, 2013) suggests that MBIs can reduce drug consumption to a significantly greater extent than other active and inactive control interventions, and MBIs appear to have a promising future as a modality in SUM treatment.
In the present exploratory study, we evaluated the effects of a relatively new MBI intervention called Mind–Body Bridging (MBB; Block & Block, 2007), as a potential adjuvant mind–body intervention in the management of SUM. MBB is predicated on a model of mind–body connections in which awareness plays a critical role in (a) recognizing disharmonious mind–body states and (b) transforming these states into more coherent mind–body states. Like better-known modalities such as mindfulness meditation and cognitive-behavioral therapy (CBT), MBB can foster the cultivation of awareness and a reduction in dysfunctional thinking. However, MBB does not involve formal practice of meditation or individual psychotherapy, and the core of basic techniques can be conveyed and experientially practiced quickly, from the first few hours of training.
For those readers who may not be familiar with MBB, we offer the following descriptions. MBB consists of cognitive, attentional, and experiential techniques for cultivating present-focused, nonjudgmental awareness of one’s body, emotions, and thoughts. When practiced regularly, MBB may lead to enhanced well-being, cognitive flexibility, and acceptance of distressing sensations, emotions, and thoughts. MBB was designed to transform self-centered cognitive/emotional processing, so that MBB practitioners may be able to make a shift away from a self-centered narrative thinking style, to adopt a more “experiential” present-centered thinking style.
At an experiential level, MBB first teaches everyday awareness skills (e.g., using sights, sounds, and tactile sensations) to help the individual calm the mind and relax the body. Everyday awareness practices allow individuals to develop a more present-centered awareness in the context of Activity of Daily Living (ADL), such as bathing, doing dishes, and cleaning the house. This part of MBB practice is somewhat analogous to the informal practice of mindfulness that is usually pursued after training in formal practices of mindfulness in MBSR (e.g., sitting meditation, walking meditation, body-scan meditation). Awareness practices in MBB are seen as the first critical component to be practiced and mastered, because they form the foundations of MBB training. Second, MBB teaches the individual to recognize and become aware of a dysfunctional mind–body state characterized by ruminative thoughts, involuntary contraction of awareness, body tension, and impaired mental or physical functioning. For example, specific “mind–body mapping” exercises employ a technique of written free association to reveal particular thought patterns called “Requirements,” expectations about how one and the world “should be” at each moment. When Requirements are excessively self-centered and not fulfilled, they can quickly and easily lead to a dysfunctional mind–body state. Learning how to “defuse Requirements” through mind–body mapping is the second critical component of MBB.
Although Requirements in MBB and dysfunctional beliefs in CBT may seem similar, there are some critical differences between the two concepts. First, a Requirement need not necessarily be maladaptive or dysfunctional in itself; such Requirements might include “I should work harder” or “Every driver should drive safely.” More importantly, a critical difference seems to lie in how Requirements or beliefs are identified and released. While a rationally oriented logical analysis may be a primary means for identifying the content of beliefs in CBT, MBB directs clients to use both mind and body in identifying and working with Requirements. This process in the identification and recognition of Requirements is crucially dependent on the cultivation of awareness practiced in an earlier phase of MBB training. When individuals continue to use awareness practices and learn to recognize Requirements, their awareness expands, helping them more effectively deal with difficulties in their daily lives. Defusing Requirements may seem to follow naturally from recognizing Requirements, provided that the cultivation of awareness has been regularly practiced. In this way, MBB carries awareness practices one critical step further by addressing the underlying cause of the resistances to clarity, that is, mental afflictions caused by an individual’s fixed idea of who he or she thinks he or she is, known as the “Identity System” (or I-System) in MBB teaching language.
The construct of the I-System may be associated with self-referential thinking and the default mode networks in the brain (Hamilton et al., 2011; Sheline et al., 2009; Spreng & Grady, 2010; Whitfield-Gabrieli & Ford, 2012). When MBB practitioners begin to make use of this “I-System” construct experientially, this facilitates the degree to which they can easily link experientially manifested indicators of disharmonious mind–body states with underlying Requirements that operate implicitly in particular situations. This new skill in linking experiential indicators with hidden Requirements soon enables MBB practitioners to readily recognize and defuse troublesome Requirements. Metaphorically speaking, awareness of the active I-System can serve as a pivot point for transforming disharmonious mind–body states by first recognizing Requirements and then defusing them through the use of cultivated present-centered awareness. Rapid development and acquisition of these new experiential skills may potentially account for MBB’s therapeutic usefulness after just a few sessions of MBB (see Tollefson, Webb, Shumway, Block, & Nakamura, 2009, for more detailed descriptions of session content of a generic MBB program).
MBB has been offered to help people with a wide variety of medical conditions, as well as healthy individuals, with promising results. In one study, MBB reduced domestic violence recidivism in offenders (Tollefson et al., 2009). In other studies, a sleep-focused MBB program led to improvements in self-reported sleep and PTSD symptoms in veterans (Nakamura, Lipschitz, Landward, Kuhn, & West, 2011), and significant improvements in self-reported sleep and depression in cancer survivors (Nakamura, Lipschitz, Kuhn, Kinney, & Donaldson, 2013). Furthermore, MBB is easy to learn, and benefits accrue rapidly, as demonstrated in these previous studies of MBB (Nakamura et al., 2013; Nakamura et al., 2011). Together, these studies provide encouraging preliminary evidence that MBB could serve as a potentially promising intervention for reducing several other mental health conditions, such as those that often co-occur with substance use disorders (SUDs). For this study, our pilot MBB program for SUD was implemented at an SA facility as a group intervention program that consisted of 20 sessions over 10 weeks (with 2 MBB sessions each week). This format of 20 sessions during a 10-week program was adapted in accordance with the standard program structure utilized at the local SA facility. In this pilot exploratory study, we evaluated MBB in a group of women with SUM attending either a residential or outpatient SA program.
Objectives and Hypotheses
The main aim of the exploratory study was to evaluate whether the MBB program would be an effective adjuvant intervention for managing (a) cravings and drug use consequences and (b) coexisting psychological symptoms in women undergoing a substance use treatment program. A central hypothesis of this exploratory study was that MBB training would assist individuals in cultivating awareness (i.e., mindfulness), resulting in increased awareness of their senses and their dysfunctional mind–body states. This would lead individuals to avoid untoward thoughts and reduce cravings for illegal substances and/or alcohol. Thus, craving was used as the endpoint outcome measure of the pilot study. We specifically hypothesized that, compared with those who were randomly assigned to treatment as usual (TAU), the participants randomly assigned to MBB + TAU would have improved outcomes in (a) reducing cravings for illicit drugs/alcohol, (b) lessening of coexisting symptoms (symptoms associated with trauma, disturbed sleep, or depression), and (c) improving well-being, self-compassion, and mindfulness.
Method
Study Participants
The study sample consisted of women aged 18 to 55 attending an SA treatment program at a facility in Salt Lake City, Utah. This SA facility is a nonprofit organization that offers alcoholism and chemical dependency treatment and education services in Utah, providing services for women only. It provides a full range of comprehensive drug-free alcoholism and chemical dependency treatment services for women, including pregnant women, women with children, and mothers working to reunify with their children. The SA facility is abstinence-oriented in regard to SUD treatment. Programs at the SA facility are designed to provide holistic treatment by addressing the biological, psychological, and social needs of clients. Treatment is individualized to meet each person’s needs and focuses on recovery issues, such as family violence, abuse, depression and mental health issues, interpersonal skills, employment, social networks and activities, and parenting. Besides individual counseling, the SA facility conducts group sessions to help clients deal with social issues and social interactions. Behavioral health treatment services included residential, day treatment, intensive outpatient, outpatient, and aftercare services, as well as education and prevention services. All clients at the SA facility were comprehensively evaluated by clinical staff at intake to document that they had a primary Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) diagnosis of substance use dependence. Placement in levels of treatment was in accordance with American Society of Addiction Medicine (ASAM) guidelines. As the SA facility is a women-only treatment center, no males were enrolled in the study. We enrolled mostly residential patients and a few outpatient clients (see Table 1).
Baseline Demographics for Participants.

Note. All variables reflect the number of participants, unless indicated. TAU = treatment as usual; MBB = Mind–Body Bridging; ASAM = American Society of Addiction Medicine; SA = substance abuse. GED = General Educational Development
Mean with SD in parentheses.
Inclusion criteria
Participants were restricted to those currently attending an SA treatment program, who were likely to remain in treatment at the facility for the duration of the entire study (as judged by the SA facility personnel on the basis of when clients entered into the program), comprising 10 weeks of treatment sessions plus pre- and postassessments. Eligible participants were fluent in English.
Exclusion criteria
SA facility clients were excluded from the study if they exhibited (a) active psychosis/psychotic symptoms that prevented them from appropriately participating in therapy and behavioral groups or (b) suicidal ideation, as ascertained by their SA facility therapist. As an agency, the SA facility treated SUD and co-occurring mental health disorders, so conditions such as depression, PTSD, anxiety, and personality disorders are fairly common in this population. Every client in the SA program had a primary diagnosis of SUD. Our main recruitment pool comprised clients who were at the time participating in the regular SA facility program (TAU, see below). All clients in TAU were potentially eligible to participate in the study; therefore, no client who expressed an interest in participating in the study was excluded from the study.
All study-related activities were conducted at the SA treatment facility, including recruitment, obtaining informed consent, collecting study data from participants, and conducting the interventions. All client medical information was stored at the facility. De-identified data collection sheets were transferred to the Pain Research Center for data analysis. The Institutional Review Board at the University of Utah reviewed and approved all aspects of the study. The ClinicalTrials.gov Identifier for the study is NCT01438346.
Study Design
This pilot study was a prospective, two parallel-group randomized controlled study comprising 38 participants assigned to one of two groups: (a) Control group - TAU (n = 20) or (b) Experimental group - MBB + TAU (n = 18). The MBB group attended MBB sessions at the same time that the TAU group attended their regular classes. During the study, participants in the MBB group attended 20 MBB sessions, 2 sessions per week, approximately 2 hr each, spread out over a period of 10 weeks. For the rest of the week, they maintained their regular TAU schedule. Study-related sessions for both groups were held during the day on Tuesday and Thursday afternoons at the same times. The study was conducted from May 2012 through November 2012. After stratified randomization was done, the proportions of residential and day clients were approximately the same in the TAU and MBB groups.
Interventions
TAU
All participants in the study followed the regular schedule at the SA facility. As background, residential clients stay in program housing off-site, and in addition to individual therapy and case management, they are required to attend daily therapeutic and psychoeducational groups at the SA facility, from Monday to Friday from 9:00 a.m. until 3:30 p.m. Day clients are required to attend groups at the SA facility from 9:00 a.m. until early afternoon. Services provided for all levels of clients include case management, individual, group, and family therapy; life skills classes; relapse prevention techniques; behavior management groups; and parenting classes. All study participants attended regular classes throughout the week. However, participants in the MBB group attended two MBB sessions in place of two of the TAU classes each week at a regular time of 1:30 p.m. to 3:30 p.m. on 2 weekdays. Because of the clients’ intensive schedules, it was determined for the purposes of the study that MBB instruction would replace two daytime regular classes rather than trying to schedule additional classes after their regular schedule. The two classes that were supplanted in the MBB group were psychoeducational groups focusing on anger management and women’s special topics. Women’s special topics were tailored to the general client population’s needs and included speakers from the community, who provided instruction to augment SA recovery, on topics such as nutrition, smoking cessation, and healthy living.
Each week, the TAU group members who were study participants met for their regular classes together with the clients who were not participating in the study. An SA facility clinical staff member provided the classes, with various activities related to the above-listed topics and detailed how these activities might help individuals deal with their SA and related psychological issues. Specifically, as part of the TAU classes comprising the study, TAU participants were given homework consisting of written assignments and behavioral practices that they were encouraged to complete.
TAU sessions were provided by master-level mental health therapists, either fully licensed or being supervised toward licensure.
MBB
A summary of MBB appears in other publications (Nakamura et al., 2013; Nakamura et al., 2011; Tollefson et al., 2009). Briefly, MBB is a mind–body intervention that teaches awareness exercises and mindfulness skills to help individuals recognize a dysfunctional mind–body state marked by heightened self-centeredness. From an MBB perspective, a person’s lack of general awareness, compounded with ruminative thoughts and bodily tension, can lead to impaired mental and/or physical functioning and buildup of stress. Over time, chronic stress can contribute to adverse mental and physical health conditions such as depression, anxiety, insomnia, PTSD, and addiction. The MBB program provides a variety of tools to help people more effectively deal with these health conditions. In MBB language, these tools include awareness exercises, thought labeling techniques, recognizing Requirements, defusing Requirements, and mind–body map exercises. As seen in these descriptors, MBB tools partially overlap with those of other MBIs and cognitive-behavioral interventions.
The MBB program was adapted for the SUM population in the present study to enable participants to understand and approach (from an MBB perspective) how to view and deal with the issues underlying their SUM. For example, in “mind–body mapping” exercises, individuals engage in a writing activity in which they are provided with a written statement of a problem or situation. They then use free association to allow their thoughts to flow, which might include thoughts about themselves, others, and events in their lives. For example, in doing a mapping exercise titled “The Problems I Have When I Use (Illegal Substances),” one may write down responses such as “I need to use drugs to feel good,” “It helps me better deal with my current situation,” “I feel guilty about using,” or “I worry what effect it would have on my child/family/partner.” Then, they evaluate how each response they provided makes them feel. They also can physically locate where in the body they experience tension following each response elicited by the statement. They then implement an awareness exercise of tuning into their senses to help reduce the mental clutter and relieve mental and bodily stress in real time. They can then follow this with the same map to see how settling the mind may impact their new responses that they write down on a second occasion. The 10-week, 20-session MBB curriculum was designed to help the group effectively learn and implement MBB principles and tools. SA facility clinical staff members were consulted in deciding on the length of the MBB intervention session before the 20-session format was selected.
Because of the relatively high levels of trauma experienced by women with SA (Dass-Brailsford & Myrick, 2010), the MBB program made use of the MBB-based Mind–Body Workbook for PTSD (Block & Block, 2010) as part of the curriculum. This workbook was the best resource available for the study population when the present study was conducted. The MBB instructor guided participants through the workbook over the period of the study intervention. The workbook also gave participants the opportunity to practice MBB skills and carry out the various mapping exercises provided in the workbook outside of class hours. Part of the MBB PTSD workbook incorporates trauma maps, which were discussed and implemented during MBB sessions. The purpose of the trauma maps was to help participants identify and resolve past trauma, which often can remain hidden in trauma victims, especially later on in life. The MBB program was structured to help participants resolve their trauma, which could lead to reduced cravings for illegal substances and/or alcohol.
For MBB to be effective, participants were encouraged to learn MBB concepts and practice the techniques regularly (i.e., daily), including completing homework in the form of exercises in the MBB workbook.
MBB sessions were provided by a board-certified Advanced Practice Registered Nurse who is a certified practitioner and senior teacher of MBB. An SA facility clinical staff member audited all MBB sessions.
Outcome Measures
Participants in both groups completed several self-report questionnaires directed toward their SUM and mental health comorbidities, including cravings severity, drug use consequences, sleep, depression, and the impact of traumatic events that occurred in their lives. They also completed questionnaires about mindfulness, self-compassion, and well-being. Responses to all questionnaires were collected at several time points during the study: (a) baseline (pretreatment assessment; 1 week before the start of the interventions, hereafter referred to as the “Pre” assessment), (b) midtreatment assessment (after 5 weeks of sessions, or “Mid”), and (c) posttreatment assessment (1 week after the final session, or “Post”). Assessments comprised the same set of self-report questionnaires at all time points, while the Post assessment also included an exit survey.
Primary measures
Penn Alcohol Craving Scale (PACS)
Craving has been extensively examined as a key factor in addiction research, yet it has remained a contentious issue (Tiffany & Conklin, 2000). Recently, Tiffany and Wray (2012) reviewed the literature on drug craving, with a consideration of use of craving assessment in clinical settings. They suggested that craving might have potential value as a target of intervention (Tiffany & Wray, 2012). Following this line of reasoning, we decided that the primary outcome indicator would be assessed by the PACS (Flannery, Volpicelli, & Pettinati, 1999), which is a five-item self-report measure assessing the extent of cravings over the previous week. It has good internal consistency and high predictive validity for alcohol relapse. Following Bowen et al. (2009), we adapted PACS to include both alcohol and drug cravings. In the present study, Cronbach’s alpha coefficient for PACS total score was .90. The choice of this scale also was motivated by the fact that the scale was used in previous MBI studies for SA (e.g., Bowen et al., 2009).
Short Inventory of Problems–Alcohol and Drugs (SIP-AD)
SIP-AD (Blanchard, Morgenstern, Morgan, Lobouvie, & Bux, 2003) is a 15-item self-report questionnaire adapted from the Inventory of Drug Use Consequences–2R (InDUC-2R; Miller, Tonigan, & Longabaugh, 1995). The SIP-AD assesses the incidence and severity of drug- and alcohol-related problems. In the present study, Cronbach’s alpha coefficient for SIP-AD total score based on the present sample was .95.
Secondary measures
We assessed the degree to which several potentially coexisting self-reported symptoms were impacted by the study interventions in the two groups of women with SUM.
Impact of Event Scale–Revised (IES-R)
The IES-R (Weiss & Marmar, 1996) comprises 22 items and is a self-report measure assessing subjective distress triggered by a traumatic event. It is a revision of the earlier version, the 15-item IES (Horowitz, Wilner, & Alvarez, 1979), which comprises two subscales, Avoidance and Intrusive Thoughts. The IES-R adds 7 items, which are hyperarousal symptoms of PTSD. As part of the assessment, respondents first identify a specific stressful life event and then score the extent to which they were distressed (or not) during the past 7 days by each of the listed items. The IES-R total score ranges from 0 to 88. Although the IES-R is not generally used for clinical diagnosis of PTSD, it can be used to gauge the degree to which participants have been distressed by a particular traumatic event identified by participants themselves. In the present study, we investigated the effects of the interventions on the IES-R total score, as well as the three subscales, Avoidance, Intrusive Thoughts, and Hyperarousal. Cronbach’s alpha coefficient for IES-R total score based on the present sample was .88.
Center for Epidemiologic Studies Depression Scale (CES-D)
The CES-D (Radloff, 1977) is one of the most common screening tests to determine an individual’s depression quotient. The quick self-test measures depressive feelings and behaviors during the past week. In the present study, Cronbach’s alpha coefficient for CES-D total score based on the present sample was .66.
Medical Outcomes Study Sleep Scale (MOS-SS)
The MOS-SS (Hays, Martin, Sesti, & Spritzer, 2005) provides an index of sleep problems and incorporates six sleep scale scores: (a) sleep disturbance, (b) sleep adequacy, (c) daytime somnolence, (d) snoring, (e) waking up short of breath with a headache, and (f) quantity of sleep. Two additional subscales evaluate composite sleep problems based on the above subscales: Sleep Problems Indexes I and II (SPI-I and SPI-II). In the present study, we assessed changes in sleep disturbance using the SPI-II subscale of MOS-SS, comprising sleep disturbance, sleep adequacy, and somnolence. The MOS-SS is similar to the Pittsburgh Sleep Quality Index (PSQI; Buysse, Reynolds, Monk, Berman, & Kupfer, 1989) developed around the same time, which includes more questions about sleep disturbance with seven more items overall. A standard MOS-SS 4-week retrospective assessment form was revised by the developers of MOS-SS to assess the participant’s sleep patterns over the previous 7 days. This revised instrument was used in previous studies to track how sleep was improved by MBB (Nakamura et al., 2013; Nakamura et al., 2011). In the present study, Cronbach’s alpha coefficient for SPI-II was .77.
Mindfulness assessment (Five-Facet Mindfulness Questionnaire [FFMQ])
The FFMQ (Baer, Smith, Hopkins, Krietemeyer, & Toney, 2006) comprises 39 items to assess five distinct facets of mindfulness, including (a) observing, (b) describing, (c) acting with awareness, (d) nonjudging of inner experience, and (e) nonreactivity to inner experience. We computed a total mindfulness score, which we used to determine the degree to which treatment influenced levels of mindfulness in the participants. In the present study, Cronbach’s alpha coefficient for FFMQ was .91.
Self-Compassion Scale (SCS)
The SCS (Neff, 2003) comprises 26 items and measures self-compassion, an emotionally positive self-attitude that could protect against the negative consequences of self-judgment, isolation, and rumination. Self-compassion conceptualized in SCS entails three main components: (a) self-kindness (being kind and understanding toward oneself in instances of pain or failure rather than being harshly self-critical), (b) common humanity (perceiving one’s experiences as part of the larger human experience rather than seeing them as separating and isolating), and (c) mindfulness (holding painful thoughts and feelings in balanced awareness rather than overidentifying with them). In this study, SCS was used to assess the potential benefits induced by the interventions. In the present study, Cronbach’s alpha coefficient for SCS total score was .88.
World Health Organization Well-Being Index (WBI)
The WBI (Bech, Olsen, Kjoller, & Rasmussen, 2003) is a five-item scale developed to assess well-being and validated by the World Health Organization Collaborating Centre in Mental Health. In the present study, Cronbach’s alpha coefficient for WBI total score was .75.
Expectation for treatment benefit
We included a single-item question to assess the degree to which participants expected the treatment to be beneficial across the two intervention groups. After participants knew to which group they had been randomized and immediately before the first session, they were asked the following question: “To what extent do you think the program you are participating in will help you improve your ability to deal with your SA issues?” They recorded their responses on an 11-point Likert-type scale with two anchor points, 0 = not at all likely and 10 = highly likely. Participants completed the expectation questionnaire before the beginning of the first class.
Study Procedures
The study was open to clients attending residential and outpatient programs at the SA treatment facility who met eligibility criteria. Initially, clients at the SA facility were informed about the study and given the opportunity to participate. Those who expressed interest and were eligible signed an informed consent form witnessed by the research team members. Participants were randomized to the TAU or MBB program using a random number generator provided by a computer program. Clients only found out their treatment assignment on the day of the first session when they were directed to the room in which TAU or MBB was conducted, respectively.
Analyses
Data from the self-report outcomes measures were analyzed using mixed effects models for repeated measures, taking into account individual differences across participants. All primary and secondary self-report questionnaires were analyzed using SPSS 18.0 (IBM, Inc., NY, USA) and included the three assessment time points: Pre (baseline), Mid, and Post. We employed a mixed effects model ANCOVA with Pre as a covariate and with Treatment and Period (comprising Mid and Post assessments) as categorical factors. The ANCOVA approach ensures that groups are adjusted for baseline differences created by randomization. We retained the full Treatment-by-Period factorial for the fixed effects. The Treatment effect in this design represents the expected therapeutic difference in outcome for any two individuals with equal baseline scores. We selected the minimal value of the Bayesian Information Criterion to determine which of the alternative covariance structures of the repeated observations provided the best fit. For each of the self-report outcome measures, the ANCOVA was used to determine whether there was an overall Treatment benefit or Treatment-by-Period interaction benefit (at Mid and Post). To gain insight into the magnitudes of between- and within-group treatment effects, we examined customized contrasts between TAU and MBB at Mid and Post adjusted for Pre (baseline), and customized contrasts for TAU and MBB at Post in relation to the baseline covariate within each group, respectively. Mixed effects analyses provide an “intent-to-treat” treatment of missing data by including all observations of the dependent measure. No observations are discarded and no data are imputed, but rather, the algorithm chooses parameter estimates that generate the highest probability for all the data observed under the model’s assumptions. The maximum-likelihood effect estimates are fully correct even in the presence of systematic unequal dropout, conditional on baseline observations (Donaldson & Moinpour, 2005; Little & Rubin, 2002).
Results
Attendance
Following the Consolidated Standards of Reporting Trials (CONSORT) recommendations, Figure 1 depicts the number of individuals screened, qualified, and enrolled in the study, as well as retention numbers at Mid and Post, for each intervention. Of the 38 participants who enrolled in the study (18 in TAU and 20 in MBB), a total of 31 completed the interventions and postquestionnaires (17 in TAU [94.4%] and 14 in MBB [70.0%]). The higher drop-out rate in the MBB group was mainly due to four participants deciding before or during the first MBB session that they realized that they would not be able to fulfill their obligations at the SA facility if they took on the (extra) homework assignments required in the MBB group, which led to their voluntary withdrawal from the study. Most clients in both groups attended the majority of the sessions (TAU = (M; SD) 75%; 18.2%, 15 sessions; 3.6 and MBB = 79.2%; 13.8%, 15.8 sessions; 2.8). These values reflect participants who completed the intervention and postassessments. Reasons for not attending study sessions included court-ordered appearances, illness, medical appointments, child care needs, and residential requirements of the program.

Study flow, presented in accordance with the CONSORT guidelines.
Demographics and Baseline Characteristics
Table 1 shows demographics and baseline measures of the two groups, before randomization. Participants were predominantly non-Hispanic White females; two females were Hispanic and one was African American. Baseline characteristics were balanced between the two groups. The majority of women reported their first age of substance use between 11 and 25 years old.
Expectation for Treatment Benefit
We performed a t test on the postrandomization expectation scores to evaluate whether the two intervention groups differed in terms of expectations for treatment improvement at the beginning of the first session. The t test yielded t = .51 and p = .62, indicating that there was no significant difference between the two intervention groups for expectations for treatment benefit (M = 7.36 and SD = 1.91 in TAU; M = 7.76 and SD = 2.11 in MBB). At the beginning of the interventions, both groups expected the treatment program to be beneficial to similar degrees.
Primary outcomes
No transformation needed to be performed for all the variables to be reported below, as they were found to be normally distributed.
PACS
Figure 2 shows adjusted mean PACS scores representing the degree to which MBB and TAU reduced alcohol and drug cravings in participants at postrandomization (comprising Mid and Post). In both treatment groups, adjusted mean PACS scores decreased at both Mid and Post time points in comparison with Pre (baseline) value (Pre covariate is indicated by the horizontal line in the figure). While the decline in PACS in both groups was similar at Mid, the decrease in PACS scores in the MBB group was greater than that in the TAU group at Post. Based on the ANCOVA, the fixed factor Treatment × Period interaction yielded p = .04, F(1, 31.70) = 4.55. Individual customized contrasts between the two groups at each time point yielded p = .06, F(1, 60.45) = 3.84, for Post, and p = .44, F(1, 60.57) = 0.60, for Mid. Of the two groups, MBB showed stronger benefit at Post with an adjusted mean total score improvement of 4.14, p < .001, t(60.97) = 3.78, from the baseline covariate value (9.81), compared with TAU adjusted mean total score improvement of 1.23, p = .22, t(60.23) = 1.25. Table 2 presents PACS unadjusted means and standard deviations for the two treatment groups at Pre, Mid, and Post, and an effect size estimate for the difference between the two interventions (i.e., Cohen’s d) at Post of 0.88, supporting the efficacy of MBB + TAU over TAU alone. The results demonstrate that MBB + TAU was more efficacious than TAU in reducing self-reported alcohol and drug cravings, specifically at the end of the intervention period (Post).

Effects of TAU and MBB interventions on alcohol/drug cravings (PACS).
Unadjusted Means (and 95% Cis) for Self-Reported Primary Outcome Measures for Comparisons Between MBB and TAU in a Substance Abuse Program for Women.

Note. CI = confidence intervals; MBB = Mind–Body Bridging; TAU = treatment as usual; PACS = Penn Alcohol Craving Scale; SIP-AD = Short Inventory of Problems–Alcohol and Drugs.
Effect size (Cohen’s d) calculated for the difference between the two interventions at (change from baseline) Post.
For Treatment by Period interaction.
p > .05 for Treatment by Period interaction.
Alcohol and drug use consequences, as measured by SIP-AD
Table 2 shows unadjusted SIP-AD total score means and standard deviations for the two treatment groups at Pre, Mid, and Post. SIP-AD scores decreased at Post in both treatment groups. Based on the ANCOVA, both Treatment, p = .99, F(1, 31.42) = 0.00, and Treatment × Period interaction, p = .26, F(1, 29.80) = 1.31, were not significant. However, both groups showed benefit at Post with adjusted mean total score improvements of 5.74, p < .001, t(58.08) = 4.63, for TAU, and 7.01, p < .001, t(60.36) = 5.16, for MBB, from the baseline covariate value (9.88). Overall, the results indicate that while both programs reduced participants’ self-reported problem severity of alcohol and drug use, there was no statistically significant difference between the two interventions at the end of the treatment period (Post).
Secondary outcomes
IES-R
Figure 3a shows adjusted mean IES-R total scores, indicating effects of MBB and TAU on IES-R scores at postrandomization. In both treatment groups, adjusted mean IES-R scores decreased at both Mid and Post compared with Pre (Pre covariate indicated by the horizontal line in the figure). However, the decrease in the MBB was larger than that in the TAU at Post. Based on the ANCOVA, the fixed factor Treatment yielded p = .03, F(1, 34.07) = 5.41. Individual customized contrasts at each time point yielded p = .01, F(1, 60.63) = 6.40, for Post, and p = .36, F(1, 60.68) = 0.86, for Mid. Both groups showed benefit at Post with adjusted mean total score improvements of 14.35, p < .001, t(60.41) = 4.55, for TAU, and 26.22, p < .001, t(60.78) = 7.56, for MBB, from the baseline covariate value (46.23). Table 3 presents unadjusted IES-R means and standard deviations for the two treatment groups at Pre, Mid, and Post, and an effect size estimate (Cohen’s d) for the difference between the two interventions at Post of 0.97, supporting the efficacy of MBB + TAU over TAU at Post. These results demonstrate that MBB + TAU was more efficacious than TAU in reducing the impact of the trauma-related event, presumably related to SUM issues, specifically at the end of the treatment period (Post).
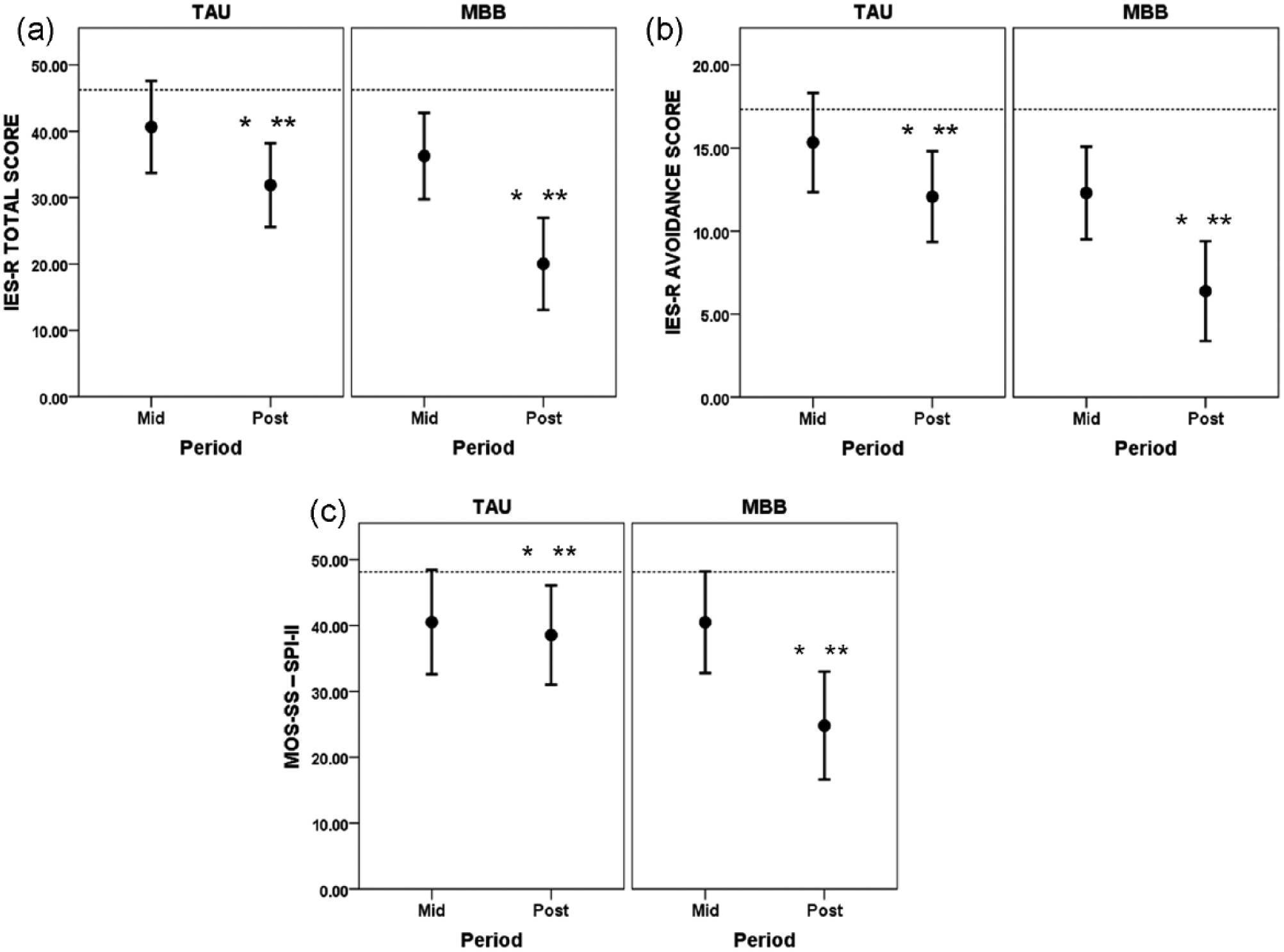
Effects of TAU and MBB interventions on (a) impact of a past traumatic event (IES-R) total score, (b) IES-R Avoidance subscale, and (c) sleep (MOS-SS–SPI-II).
Unadjusted Means (and 95% Cis) for Self-Reported Secondary Outcome Measures for Comparisons Between MBB and TAU in a Substance Abuse Program for Women.

Note. CIs = confidence intervals; MBB = Mind–Body Bridging; TAU = treatment as usual; IES-R = Impact of Event–Revised; CES-D = Center for Epidemiologic Studies Depression Scale; MOS-SS = Medical Outcomes Study Sleep Scale; SPI-II = Sleep Problems Index–II.
Effect size (Cohen’s d) calculated for the difference between the two interventions at (change from baseline) Post.
For Treatment.
For Treatment by Period interaction.
p > .05 for Treatment. **p > .05 for Treatment by Period interaction.
For the IES-R Avoidance subscale, Figure 3b shows adjusted mean IES-R avoidance scores at postrandomization for both groups. While mean avoidance scores decreased at Mid and Post compared with Pre in both treatment groups, the decrease in MBB was larger than that in TAU. Based on the ANCOVA, the fixed factor Treatment yielded p = .01, F(1, 32.85) = 8.20. Both groups showed benefit at Post with adjusted mean score improvements of 5.26, p < .001, t(60.33) = 3.85, for TAU, and 10.95, p < .001, t(60.74) = 7.29, for MBB, from the baseline covariate value (17.33). Table 3 shows unadjusted avoidance means and standard deviations, for the two treatment groups at Pre, Mid, and Post, and an effect size estimate (Cohen’s d) for the difference between the two interventions at Post of 1.36, supporting the efficacy of MBB + TAU over TAU alone at Post.
For the IES-R Intrusive Thoughts subscale, in both treatment groups, adjusted mean scores decreased at Post compared with Pre (see Table 3). Based on the ANCOVA, both Treatment, p = .16, F(1, 33.93) = 2.06, and Treatment × Period interaction, p = .53, F(1, 32.95) = 0.39, were not significant. However, both groups showed benefit at Post with adjusted mean score improvements of 5.41, p < .001, t(60.35) = 4.84, for TAU, and 7.90, p < .001, t(60.76) = 6.43, for MBB, from the baseline covariate value (16.03).
For the IES-R Hyperarousal subscale, in both treatment groups, adjusted mean scores decreased at Post compared with Pre (see Table 3). Based on the ANCOVA, both Treatment, p = .23, F(1, 33.98) = 1.50, and Treatment × Period interaction, p = .16, F(1, 31.86) = 2.09, were not significant. However, both groups showed benefit at Post with adjusted mean score improvements of 3.91, p < .01, t(58.10) = 3.35, for TAU, and 7.17, p < .001, t(59.72) = 5.59, for MBB, from the baseline covariate value (12.87).
The IES-R results for total score and Avoidance subscale demonstrate that MBB + TAU was more efficacious than TAU in reducing the impact of the trauma-related event, presumably related to SUM issues, which appeared most pronounced at the end of the treatment period (Post).
Depression, as measured by CES-D
Table 3 shows unadjusted CES-D means and standard deviations for the two treatment groups at Pre, Mid, and Post, indicating that CES-D scores decreased at Post in both treatment groups. Baseline CES-D mean scores for TAU and MBB were 31.11 (95% confidence interval [CI] = [27.46, 34.76]; upper, lower) and 30.85 (95% CI = [27.94, 33.76]), respectively, which are considerably higher than the CES-D cutoff score of 16 that has been used for screening of clinical depression (Radloff, 1977). Based on the ANCOVA, both Treatment, p = .96, F(1, 33.70) = 0.00, and Treatment × Period interaction, p = .18, F(1, 30.88) = 1.90, were not significant. However, both groups showed benefit at Post with adjusted mean total score improvements of 6.32, p < .001, t(53.25) = 3.90, for TAU, and 8.03, p < .001, t(57.71) = 4.57, for MBB, from the baseline covariate value (30.52). Overall, the results indicate that while both programs reduced self-reported depression symptoms, there was no statistically significant difference between the two interventions at the end of the treatment period (Post).
Sleep, as measured by SPI-II from MOS-SS
Figure 3c shows adjusted mean SPI-II scores, indicating effects of MBB and TAU on sleep at postrandomization. In both treatment groups, there were decreases in adjusted mean SPI-II scores at both Mid and Post compared with Pre (Pre covariate indicated by the horizontal line in the figure). However, the decrease in SPI-II in the MBB was larger than that in the TAU at Post. Based on the ANCOVA, the Treatment × Period interaction yielded p = .04, F(1, 30.54) = 4.77. Individual customized contrasts at each time point yielded p = .02, F(1, 57.00) = 6.07, for Post, and p = .99, F(1, 56.42) = 0.00, for Mid. Both groups showed benefit at Post with adjusted mean SPI-II score improvements of 9.57, p = .01, t(54.38) = 2.55, for TAU, and 23.32, p < .001, t(58.78) = 5.70, for MBB, from the baseline covariate value (48.12). Table 3 presents SPI-II unadjusted means and standard deviations for the two treatment groups at Pre, Mid, and Post, and an effect size estimate (Cohen’s d) for the difference between the two interventions at Post of 0.81. Overall, the results demonstrate that MBB was more efficacious than TAU in reducing sleep problems indicated by SPI-II, specifically at the end of the treatment period (Post).
Mindfulness, as measured by FFMQ
Figure 4a shows adjusted mean total FFMQ scores to represent the degree to which MBB and TAU impacted mindfulness at postrandomization. In the figure, both treatment groups showed increases in adjusted mean FFMQ scores at both Mid and Post compared with Pre (Pre covariate indicated by the horizontal line in the figure). However, the increase in total FFMQ scores in the MBB was larger than that in the TAU at Post. Based on the ANCOVA, Treatment yielded p = .01, F(1, 33.34) = 7.72, and the Treatment × Period interaction yielded p = .01, F(1, 28.69) = 7.61. Individual customized contrasts at each time point yielded p = .001, F(1, 43.84) = 13.12, for Post, and p = .14, F(1, 43.68) = 2.28, for Mid. Of the two groups, only MBB showed benefit at Post with an adjusted mean total score improvement of 25.97, p < .001, t(46.39) = 6.77, from the baseline covariate value (126.12), whereas TAU adjusted mean total score improvement was 6.44, p = .10, t(41.11) = 1.70. Table 4 shows unadjusted total FFMQ means and standard deviations for the two groups at Pre, Mid, and Post, and an effect size estimate (Cohen’s d) for the difference between the two interventions at Post of 1.27. Overall, the results support that MBB was more efficacious than TAU in increasing mindfulness assessed by FFMQ, specifically at the end of the treatment period (Post).

Effects of TAU and MBB interventions on (a) mindfulness (FFMQ), (b) self-compassion (SCS), and (c) well-being (WBI).
Unadjusted Means (and 95% CIs) for Self-Reported Mindfulness, Self-Compassion, and Well-Being for Comparisons Between MBB and TAU in a Substance Abuse Program for Women.

Note. CIs = confidence intervals; MBB = Mind–Body Bridging; TAU = treatment as usual; FFMQ = Five-Facet Mindfulness Questionnaire; SCS = Self-Compassion Scale; WBI = Well-Being Index.
Effect size (Cohen’s d) calculated for the difference between the two interventions at (change from baseline) Post;
For Treatment.
For Treatment by Period interaction.
p > .05 for Treatment. **p > .05 for Treatment by Period interaction.
Self-compassion, as measured by SCS
Figure 4b shows adjusted mean total SCS scores representing the degree to which MBB and TAU impacted self-compassion at postrandomization. In the figure, both treatment groups showed increases in adjusted mean total SCS scores at both Mid and Post compared with Pre (Pre covariate indicated by the horizontal line in the figure). Furthermore, the increase in total SCS scores in the MBB was larger than that in the TAU at Post. Based on the ANCOVA, Treatment yielded p = .07, F(1, 34.33) = 3.65, and the Treatment × Period interaction yielded p = .02, F(1, 29.84) = 6.08. Individual customized contrasts at each time point yielded p = .01, F(1,45.51) = 7.37, for Post, and p = .43, F(1, 45.28) = 0.64, for Mid. Both groups showed benefit at Post with adjusted mean total score improvements of 2.18, p = .002, t(42.74) = 3.29, for TAU, and 4.78, p < .001, t(48.09) = 6.88, for MBB, from the baseline covariate value (16.07). Table 4 shows unadjusted total SCS means and standard deviations for the two treatment groups at Pre, Mid, and Post, and an effect size estimate (Cohen’s d) for the difference between the two interventions at Post of 0.76. Overall, the results support that MBB + TAU was more efficacious than TAU in increasing self-compassion, specifically at the end of the treatment period (Post).
Well-being, as measured by WBI
Figure 4c shows adjusted mean WBI scores, representing the degree to which MBB and TAU impacted well-being at postrandomization. In the figure, both treatment groups showed increases in adjusted mean WBI scores at both Mid and Post compared with Pre (Pre covariate indicated by the horizontal line in the figure). Furthermore, the increase in the WBI score in the MBB was larger than that in the TAU at Post. Based on the ANCOVA, Treatment yielded p = .13, F(1, 34.94) = 2.36, and Treatment × Period interaction yielded p = .05, F(1, 31.42) = 4.01. Individual customized contrasts at each time point yielded p = .03, F(1, 51.58) = 5.31, for Post, and p = .7, F(1, 51.36) = 0.15, for Mid. Of the two groups, only MBB showed benefit at Post with an adjusted mean total score improvement of 5.44, p < .001, t(54.09) = 4.38, from the baseline covariate value (12.08), whereas TAU’s adjusted mean total score improvement was 1.52, p = .20, t(48.68) = 1.30. Table 4 shows unadjusted WBI means and standard deviations for the two treatment groups at Pre, Mid, and Post, and an effect size estimate (Cohen’s d) for the difference between the two interventions at Post of 0.73. The results support that MBB + TAU was more efficacious than TAU in increasing well-being assessed by WBI, specifically at the end of the treatment period (Post).
Discussion
This exploratory study evaluated the efficacy of a mind–body intervention program for SUM (MBB for SUM), which was implemented as a 20-session course over 10 weeks. In comparison with the TAU offered at the study site, the addition of the new MBB program to TAU decreased the primary outcome measure of drug and alcohol cravings in comparison with the TAU group. In addition, in comparison with TAU, the addition of MBB to TAU decreased the impact of past trauma (especially with respect to avoidance) and disturbed sleep in a group of women who were recruited from a local SA treatment facility. Furthermore, in comparison with TAU, the addition of MBB to a standard treatment program increased mindfulness, self-compassion, and well-being. While MBB was effective in decreasing self-reported depressive symptoms, there was no statistically significant difference between the two groups, as both intervention programs led to a decrease in depression symptoms as measured by CES-D. Overall, these findings are encouraging in supporting the value of the MBB program as a complementary adjuvant intervention for SUM. An MBB for SUM program may serve as an additional module that can be incorporated into a comprehensive residential and outpatient SUM treatment program implemented in a community setting.
Reduction of cravings associated with MBB at Post is the main finding, and this is consistent with findings from other MBIs for SUM reported in the literature (Bowen et al., 2009; Bowen et al., 2014; Bowen et al., 2006; Brewer et al., 2011; Brewer et al., 2009; Davis et al., 2007; Davis, Goldberg, et al., 2014; Davis, Manley, et al., 2014; Garland et al., 2010; Garland et al., 2014; Garland, Schwarz, Kelly, Whitt, & Howard, 2012; Witkiewitz, Bowen, Douglas, & Hsu, 2013; Zgierska et al., 2009). The convergence of these findings can increase our confidence in the usefulness of MBIs for SUM treatment in general, and below, we wish to discuss some notable features that may be specific to MBB.
In this study, in addition to reducing cravings, participants in the MBB group also showed a significant reduction of IES-R scores (especially Avoidance subscale scores), possibly reflecting that MBB participants might be able to confront and resolve some past traumas associated with their SUM. These MBB participants also reported a reduction of disturbed sleep. Furthermore, this study produced some additional findings concerning positive qualities associated with potential recovery from SUM. MBB participants reported increased mindfulness, increased self-compassion, and increased well-being. To our knowledge, our study may be one of the few MBI studies that have produced this consistent pattern of findings in all these different indicators of negative symptoms (cravings, impact of trauma, disturbed sleep) and positive qualities (mindfulness, self-compassion, well-being). The pattern of findings in this study is generally consistent with those patterns observed in previous MBB studies (Nakamura et al., 2013; Nakamura et al., 2011), strengthening the evidence that MBB can bring about additional beneficial improvements in other indicators of psychosocial functioning, even though the domains assessed by these indicators may not be explicitly targeted in the MBB program itself. Finally, it may be of interest to note that mindfulness increased following MBB in this and previous MBB studies, in contrast to other MBI studies that did not show a significant increase of mindfulness in comparison with control intervention conditions (Chiesa & Serretti, 2013). In the present study, TAU was used as an active control group that produced improvements and reductions in many indicators assessed in the study, but TAU did not significantly increase mindfulness per se. The critical question of what to use as a control intervention condition will need to be considered carefully in future studies.
The present study has a number of limitations. First, owing to logistical difficulties inherent in conducting the present study in a community-based setting, we could not include study-specific clinical evaluation of women who had enrolled to receive care at a local SA treatment facility. Because of this, little information was available in the study in terms of types and durations of SUD conditions that participating women were suffering from, although some related information was recovered and presented in Table 1. Despite this shortcoming, it should be noted that the two groups of women had comparable ASAM placement levels at baseline (see Table 1), reflecting the severity of their SUDs. Although our study did not use a strict inclusion and exclusion criteria in selecting potential study participants, our strategic decision not to exclude anyone based on stable coexisting symptoms may have rendered our study sample more generalizable to women receiving SUM treatment at typical community-based SA facilities. Second, the study did not include a follow-up assessment to evaluate whether treatment gains were maintained over time. This was a major shortcoming of the present study. Given the turnaround times usually observed at the study site and the general failure of the facility to recontact their clients, we strategically determined that it was not feasible to include a follow-up assessment. We strongly believe that inclusion of follow-up assessment will be critical to assess impacts of the MBB program on relapse in SUM in future studies. Another weakness was lack of assessment of treatment fidelity, especially for MBB. Although the MBB instructor was a senior MBB teacher who had been involved in certifying newly trained MBB practitioners, inclusion of treatment fidelity assessment would have increased the potential value of the study findings. There were more participants who dropped out from the MBB program after they were informed about the amount of home exercises required in the program. Given the already demanding nature of the comprehensive program in which these women were participating, it will be desirable to find a way to decrease homework initially and to increase homework gradually after core techniques are mastered sufficiently. Our sample was limited to women with SUM treated at a local SA treatment center. Inclusion of men with SUM in future studies would be necessary to determine whether the addition of MBB would be effective for men as well. Finally, MBB consisted of both cognitive and experiential (i.e., sensory) techniques that are designed to develop present-focused, nonjudgmental awareness of one’s body, emotions, and thoughts. Because of this multicomponent nature of the MBB program, it remains to be seen which MBB component was associated with observed changes in MBB participants. These shortcomings should be addressed in future research.
The MBB program evaluated in the study consisted of 20 sessions over 10 weeks, so it was a much longer program than the ones used in previous studies of MBB focused on improving sleep (these sleep-focused studies used 2 or 3 sessions over 2 or 3 weeks). There are some recent studies of mindfulness demonstrating that even a brief training in mindful attention (Westbrook et al., 2013) or mindfulness meditation (Zeidan, Gordon, Merchant, & Goolkasian, 2010; Zeidan et al., 2011) can significantly reduce self-reported and neural reactivity to cue-induced craving or painful stimulation, respectively. Previous studies of MBB are in line with the findings from these studies. However, before we undertook the study, we reasoned that the conditions of those women who enrolled in the present study might be substantially more difficult than those evaluated in previously published studies of MBB. While previous studies of MBB focused on sleep disturbance as a focal point of the program in the context of other possible coexisting symptoms, the present MBB program was specifically geared toward addressing many relevant issues frequently associated with treatment of SUD, especially those concerning the impact of past trauma. It is encouraging that MBB was able to reduce the impact of previous trauma, especially with respect to avoidance-related items in the present study. Overall, the patterns of findings based on the MBB program for SUM are consistent with those patterns from earlier MBB studies targeting disturbed sleep. This suggests that MBB can be specifically tailored for a particular mental health condition, such as SUM, in a productive manner.
The issue of relapse is critical in future studies of MBB for SUM. After recognizing that they have an SA problem, or following conviction for an SA offense, many individuals undergo treatment to help them abstain from engaging in these high-risk behaviors. However, up to 60% of substance users revert back to SA within a year after receiving treatment (McLellan, Lewis, O’Brien, & Kleber, 2000). Attempts to diminish these high rates of recidivism led to the development of cognitive-behavioral treatment such as Relapse Prevention(RP) (Witkiewitz & Marlatt, 2004). While relapse prevention has empirical support from previous studies, up to 70% of clients may still relapse (Heyman, 2013). These high rates of recidivism clearly indicate the pressing need to develop other complementary effective treatments that might enhance or supplant currently available treatments. Recently, Bowen et al. (2014) reported results from a large-scale RCT of a Mindfulness-Based Relapse Prevention (MBRP) program and cognitive-behavioral RP program in comparison with the control intervention program (TAU = 12-step program). Compared with TAU, participants assigned to MBRP and RP reported significantly lower risk of relapse to substance use and heavy drinking and, among those who used substances, significantly fewer days of substance use and heavy drinking at the 6-month follow-up. Cognitive-behavioral RP initially showed an advantage over MBRP in time to first drug use, but at the 12-month follow-up, MBRP participants reported significantly fewer days of substance use and significantly decreased heavy drinking compared with RP and TAU. Interestingly, impacts of the MBRP program on mindfulness as measured by FFMQ did not clearly show up in this impressive study.
The relationship among mindfulness, craving, and behavior (e.g., drug use behavior) remains to be clarified (Grossman, 2008). Two recent studies report findings that may shed new light on this particular issue (Bowen & Enkema, 2014; Moore et al., 2014). After reviewing research in both nontreatment seeking college students and in clinical samples, and examining the relationship between trait mindfulness and substance dependence in a clinical sample, Bowen and Enkema (2014) identified and assessed the moderating effect of avoidant coping that might explain the disparate findings in the clinical versus nonclinical samples. In another recent study, Moore and colleagues (2014) used Ecological Momentary Assessment (EMA) to collect data on how cravings and affect were related to subsequent relapse in a sample of patients entering outpatient treatment for SA. They found that individuals who reported an increase in cravings on a given moment were 14 times more likely to relapse on the subsequent prompt than individuals who did not experience an increase in cravings. Furthermore, they also found that individuals who reported lower average cravings were more likely to relapse following a sudden increase in cravings than were individuals who reported higher average cravings. (Unfortunately, mindfulness was not assessed in this EMA study, making it impossible to clarify the role of mindfulness in modulating impacts of cravings on relapse.) It is clear that findings from these two studies point to the complex dynamic relationships among drug cravings, mindfulness, and relapse that may be unfolding over time, as modulated by other mediating variables such as coping strategies. Clearly, more attention will need to be directed to clarify this clinically important issue. Nonetheless, the present study provided preliminary evidence showing that the reduction of both cravings and drug use consequences can occur together with increased mindfulness following the completion of an MBB program.
Developing a novel effective treatment of SUM/SUD and its associated coexisting conditions is extremely challenging. Recent years have seen an increased interest in the use of MBIs (as described in recent systematic reviews - Chiesa & Serretti, 2013; Zgierska et al., 2009) to manage clinically challenging configurations of symptoms and conditions associated with SUM. A transdiagnostic orientation embodied in MBB, in particular, and in MBIs, in general, might open up a space of possibility in which an integrative treatment of the whole individual person will take center stage from a conceptually unified perspective. The continued development of MBB designed to address multiple coexisting conditions within the single person (such as persons with SUM and other coexisting symptoms) may be potentially useful and urgently needed for SUM/SUD treatment in particular and mental health care in general. Preliminary initial evidence from the present study may serve to encourage this line of future research.
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the sponsors. The sponsors had no role in the conduct of the study, collection, management, analysis and interpretation of the data, and preparation, review, or approval of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The study reported was in part supported by the Mind–Body Research Program through the University of Utah Health Sciences Development Office.