
Abstract
The objective of this study is to determine whether different types of caregiver support services are associated with different outcomes for male and female caregivers. Information was obtained on 148 caregivers’ use of three types of support services provided by government-contracted agencies: counseling and education services, respite and supplemental services, and financial services. Five caregiver outcomes were included. Use of counseling and education services and financial services was associated with better caregiver outcomes in female caregivers, but not male caregivers. Among caregivers using respite and supplemental types of services, male caregivers showed better outcomes than did female caregivers. Female caregivers who used respite and supplemental services showed worse outcomes in caregiver mastery and caregiver satisfaction than those who did not use the services. Male and female caregivers responded differently to the caregiver support service. Providing female caregivers with counseling services along with respite services may result in added benefits for female caregivers.
Keywords
Introduction
An estimated 65.7 million Americans function as informal caregivers of ill or disabled individuals, and more than 3 in 10 U.S. households (31.2%; 36.5 million households) report being served by an unpaid family caregiver. Among these caregivers, 7 in 10 take care of someone 50 years of age or older (AARP, 2009). Caregivers are predominantly female (66%; AARP, 2004, 2009; Coleman & Pandya, 2002). Research has shown differences among populations of male and female caregivers, such as in the types of care they provide to their care recipients. For example, The National Alliance for Caregiving survey has reported that male caregivers are less likely to provide personal care (AARP, 2009). Male and female caregivers also experience caregiving differently (AARP, 2009; de Cordova et al., 2010; Kao, 2003; Kao & McHugh, 2004; Lawrence, Goodnow, Woods, & Karantzas, 2002; Navaie-Waliser, Spriggs, & Feldman, 2002; Vitaliano et al., 2002; Vitaliano, Zhang, & Scanlan, 2003; Wallsten, 2000).
One study using a cross-sectional design interviewed 1,002 randomly selected and nationally representative caregivers and found that female caregivers were significantly more likely to be better educated and unemployed; to provide more intensive and complex care; to have difficulty balancing care provision with other family and employment responsibilities; to suffer from poorer emotional health secondary to caregiving; and to cope with caregiving responsibilities by forgoing respite and by engaging in increased religious activities (Navaie-Waliser et al., 2002). Studies have also shown that female caregivers, compared with male caregivers, perceive caregiving as more burdensome (Kao, 2003; Kao & McHugh, 2004; Kramer & Kipnis, 1995; Lawrence et al., 2002; Lutzky & Knight, 1994; Nagatomo et al., 1999; Wallsten, 2000) and report higher levels of depression and anxiety and lower levels of subjective well-being (AARP, 2004; Johnson & Wiener, 2006; Yee & Schulz, 2000). Female caregivers who provide 36 or more hours per week of care to a spouse have been shown to have a dramatic increase in risk of mental health problems (Cannuscio et al., 2002). Vitaliano et al. (2002) also found that different factors may result in distress at different times for male and female caregivers. For female caregivers, distress (e.g., burden or sleep problems) resulted directly from the caregiving tasks and lack of social resources. For male caregivers, vulnerability was a factor that resulted in distress initially, while lack of social resources became more important later, resulting in higher distress (Vitaliano et al., 2002).
The older population in the United States is fast increasing, and the caregiver support ratio (The ratio of the population aged 45-64 to the population aged above 80) will plummet when the first baby boomers begin turning 80, the age at which the need for long-term care support increases. The Federal Commission on Long-Term Care has taken an important step to elevate family caregiving as a public issue that can no longer be ignored and to call for research on caregiver interventions to see what supportive services work best and for whom (Redfood, Feinberg, & Houser, 2013). Although the magnitude of effects of caregiver support interventions found in the literature is inconsistent, research studies have shown positive effects and that different interventions are associated with different outcomes for caregivers (Cassie & Sanders, 2008; Chen, Hedrick, & Young, 2009; Lopez-Hartmann, Wens, Verhoeven, & Remmen, 2012; Mason et al., 2007; Shaw et al., 2009). However, most studies have focused only on evaluating the effects of caregiver interventions and have not addressed the commission’s call to explore the usefulness of different services to different populations of caregivers. To begin to answer this call, in the aim of understanding how different characteristics among caregivers are associated with the outcomes of particular caregiver interventions, the current study explores how male and female caregivers respond to support services. We hope our study findings may be helpful to future development of caregiver support services.
Most research studies have examined caregiver related intervention as a monolithic category or have assessed only one particular outcome, such as caregiver burden (Brodaty, Green, & Koschera, 2003; Burns, Nichols, Martindale-Adams, Graney, & Lummus, 2003; Gallagher-Thompson et al., 2003; Lee & Cameron, 2004; Maas et al., 2004; Newcomer, Yordi, DuNah, Fox, & Wilkinson, 1999; Roberts et al., 1999; Toseland, Blanchard, & McCallion, 1995; Zank & Schacke, 2002). Only a few studies have used multiple measures to examine caregiver support service outcomes. Chen and colleagues developed and tested an evaluation tool to assess multiple outcomes to evaluate different caregiver support services. Their study findings showed that different caregiver support services are associated with different caregiver outcomes (Chen et al., 2009). The current study used the multiple outcome measurements used in Chen and colleagues’ study, and further investigated whether different services were associated with different outcomes for male versus female caregivers.
Purpose of Study
The purpose of this study was to determine whether different types of caregiver support services are associated with different caregiver outcomes for male versus female caregivers. We collaborated with Aging and Disability Services (ADS), the local Area Agency on Aging (AAA) in Seattle, Washington, in a pilot study that evaluated a federally funded and state-funded project, the Family Caregiver Support Program (FCSP), in King County in Washington State. In this region, the FCSP provides various services to caregivers and their care recipients, including adult day care, in-home respite, information services, and financial assistance to caregivers (ADS, 2003).
Method
Design, Setting, and Participants
This study was a descriptive, one-time survey of caregivers living in King County who were reported as having received services from local service agencies of ADS. Four local service agencies agreed to send out an invitation letter and questionnaire to all caregivers who had received FCSP-funded services. The University of Washington Human Subjects Division approved this study.
Data Collection Method
For this study, each agency sent each of their caregiver clients a cover letter, a questionnaire, and a postage-paid return envelope addressed to ADS. To protect client confidentiality, the questionnaires were anonymous, and no follow-up occurred. A total of 866 survey packets were sent out, and 177 questionnaires (20.4%) were returned.
Measurements
The FCSP is a program with multiple components, which include various types of services, and it is likely that caregivers’ experiences with the program are multifaceted as well (Van Houtven, Voils, & Weinberger, 2011). The tool used in the current study, the Aging and Disability Services–Caregiver Appraisal Scale (ADS-CAS), assessed multiple aspects of the caregiver experience. The ADS-CAS is based on Lawton and Brody’s(1969) Caregiver Appraisal Scale (CAS) for the appropriateness of its language and its coverage of the broad scope of relevant caregiver experiences (Vitaliano, Young, & Russo, 1991). The CAS was developed on the basis of both successful scientific evidence and hands-on experience. The details of the process of developing the ADS-CAS were described in Chen (2009).
The ADS-CAS includes three subscales: Subjective Burden (e.g., “Your health has suffered because of the care you must give to care receiver” or “Very tired as a result of caring for care receiver”), Caregiving Mastery (e.g., “I can fit in most of the things I need to do in spite of the time taken by caring for care receiver”), and Caregiving Satisfaction (e.g., “Helping care receiver has made me feel closer to him/her” or “Care receiver shows real appreciation of what I do for her/him”). The ADS-CAS consists of 34 items, with 13 items, 12 items, and 9 items each for the Subjective Burden, Caregiving Mastery, and Caregiving Satisfaction subscales, respectively.
Participants responded to each item on the ADS-CAS based on a 5-point scale, from rarely or never (1) to most of the time (5). Higher total and subscale scores represent more positive appraisals, except for the Subjective Burden subscale, where higher scores indicate higher perceived subjective burden.
In addition to the three subscales, the ADS-CAS also surveys information about caregivers’ age, gender, and relationship to the care recipient; the types of care provided; and the types of caregiver support services used by the caregivers. Agencies reported providing a list of services, including (a) information about services, (b) assistance in accessing services, (c) caregiver counseling, (d) caregiver education and training, (e) financial assistance, (f) respite services/adult day care, (g) help with housework, (h) delivered meals, (i) transportation, and (j) cash support. Caregivers were asked in the survey whether they had used each of these services. These 10 types of caregiver support services were further grouped in three categories: (a) counseling and education services, (b) respite and supplemental services, and (c) financial support services. The counseling and education services category includes information about services, assistance in accessing services, caregiver counseling, and caregiver education and training. The respite and supplemental services category includes respite services/adult day care, help with housework, delivered meals, and transportation. The financial support services category includes financial assistance and cash support for caregiving. A general service satisfaction question is also included in the ADS-CAS, with a 4-point scale response: poor (1), fair (2), good (3), or excellent (4).
After reverse coding and multiple imputation, Cronbach’s alphas for the ADS-CAS were .90. The power to detect statistically significant differences between male caregivers and female caregivers was .72, and the power to detect differences between caregivers who reported having used at least one service and those who reported not using any service was .51 and .57 for male and female caregivers, respectively. Details of the psychometric properties of ADS-CAS were reported in Chen (2009).
Data Analysis
Data analyses were conducted using the Statistical Package for the Social Sciences (SPSS-PC, Version 16.0). Prior to analyzing the data, all items were examined to assess the accuracy of variable calculations and missing values. If variables were missing at a rate larger than 5%, multiple imputation was applied (Rubin, 1977; Schafer, 1997, 1999, 2000).
Descriptive analyses were used to depict the characteristics of the caregivers and the support services they used. Three steps were included in the evaluation method. First, we examined the gender differences in care provided and services used using the t test. Second, we conducted MANCOVA to examine gender difference, comparing ADS-CAS scores between male and female caregivers (a) who reported using any of the 10 caregiver support services, and (b) who had used only one of the three categories of services. Third, we conducted MANCOVA to examine gender differences by stratifying male and female caregivers and comparing their appraisals in the following categories: (a) among those who reported using any of the 10 services versus those who did not; and (b) among those who used only one of the three categories of services versus those who did not use that particular service category. (For example, caregivers who had used services in the financial services category only and no services from other categories were compared with caregivers who reported they had not used any services from the financial services category. Caregivers who were “nonusers” in one category may have used services in other categories, or may have reported not using any services at all.) As recommended by Chen (2010), analysis is focused on categories of service because analyses of individual types of service and of the three service categories revealed similar findings.
Caregivers’ age and the number of caregiving activities they provided were controlled as covariates. The outcome measures were (a) the item mean of the ADS-CAS; the item means of each of the three subscales of the ADS-CAS: (b) Subjective Burden, (c) Caregiving Mastery, and (d) Caregiving Satisfaction; and (e) the caregivers’ satisfaction with the services they used.
Results
The survey response rate was 20.4% (177 questionnaires out of 866). Five of the questionnaires were returned blank, and two were returned with no information on ADS-CAS but text information regarding their suggestions for future service development only. Furthermore, six of the responding caregivers stated that they were not providing any care at this point, and 16 did not specify their gender. As a result, only 148 questionnaires were entered for quantitative data analysis. About 81.7% of the responding caregivers were female (n = 121), and 18.2% were male (n = 27). Their ages ranged from less than 20 to more than 81 years old, with an average age of 57. The average age of male caregivers (65.3 years) was significantly older than the average age of female caregivers (56.4 years). The majority of responding caregivers stated that they were caring either for a spouse/partner (48.8%) or for elderly parents (41.2%). Male caregivers were more likely to care for a spouse/partner (64.3%) than for elderly parents (32.1%), whereas a relatively equal percentage of female caregivers were caring for a spouse/partner (39.2%) and for elderly parents (40.0%; see also Table 1).
Care Provided by Caregivers.
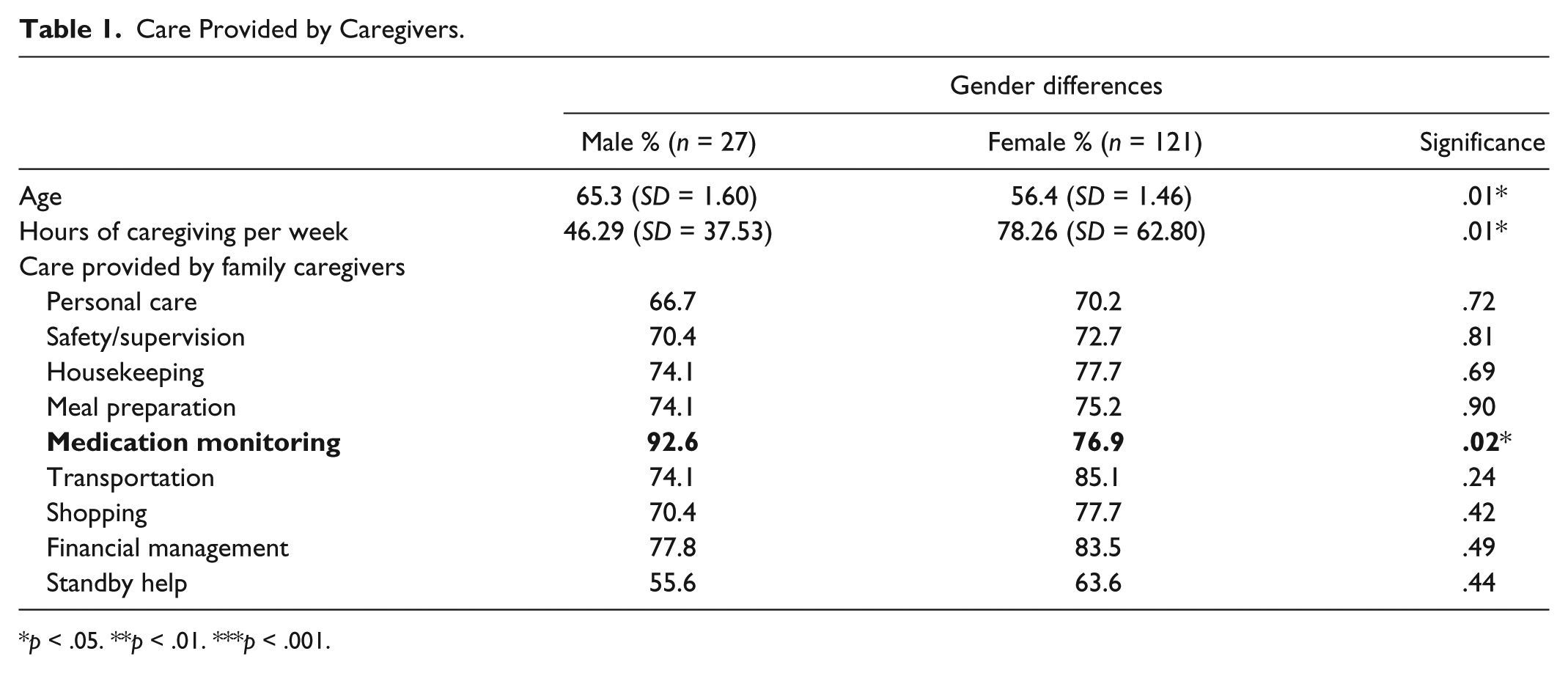
p < .05. **p < .01. ***p < .001.
About 70% of caregivers provided personal care, 98.2% provided at least one type of instrumental activities of daily living (IADL) care, and 86.6% provided at least three types of IADL care. Caregivers provided from 1 to 10 types of care to their care recipients, with an average of 6.8 (SD = 2.24). About one third provided all 10 kinds of caregiving activities listed in the questionnaire. Male and female caregivers provided an average of 6.6 (SD = 2.17) and 6.8 (SD = 2.28) types of care to their care recipients, respectively. The most common type of care provided by male and female caregivers was different. The most common types of care provided by male caregivers were medication monitoring (92%) and financial management (77.8%); the most common types of care provided by female caregivers were transportation (85.1%) and financial management (77.7%). The percentage of caregivers providing medication monitoring was significantly higher among male caregivers than female caregivers (p < .05). Among male caregivers, 92.6% provided medication monitoring, whereas only 76.9% of women provided such care to their care receivers. The average number of caregiving hours that the caregivers had spent in the previous week was 73.54 hr (SD = 60.17), with an average of 46.29 hr (SD = 37.53) for male caregivers and 78.26 hr (SD = 62.80) for female caregivers (p < .05). Forty-three percent of male caregivers provided more than 50 hr of care in the previous week, whereas almost 58% of female caregivers provided more than 50 hr of care in the week preceding the survey.
Caregivers reported using a range of zero to seven ADS caregiver support services, with an average of 1.9 (SD = 1.54). Male and female caregivers used an average of 1.8 (SD = 1.47) and 1.9 (SD = 1.46) types of support services, respectively. The services most commonly used by male and female caregivers were information services (44.4% in male caregiver vs. 54.5% in female caregivers) and respite services (33.3% in male caregivers vs. 28.1% in female caregivers). The percentage of female caregivers receiving cash to support caregiving was significantly higher than male caregivers (p < .05). Five male caregivers (18.5%) and 16 female caregivers (13.2%) stated that they had not used any services, even though all the caregivers surveyed had been identified by agencies as service recipients.
Gender Differences in the Scores of ADS-CAS
Both male and female caregivers reported moderate levels of subjective burden, caregiver mastery, caregiver satisfaction, and service satisfaction. After controlling for caregivers’ age and the number of care activities provided, there were no differences between male caregivers and female caregivers in the ADS-CAS measures or satisfaction toward services, with one exception: Male caregivers perceived a lower subjective burden than did female caregivers (p < .05; see Table 2).
Item Means of the ADS-CAS Scale and Subscales (N = 148).
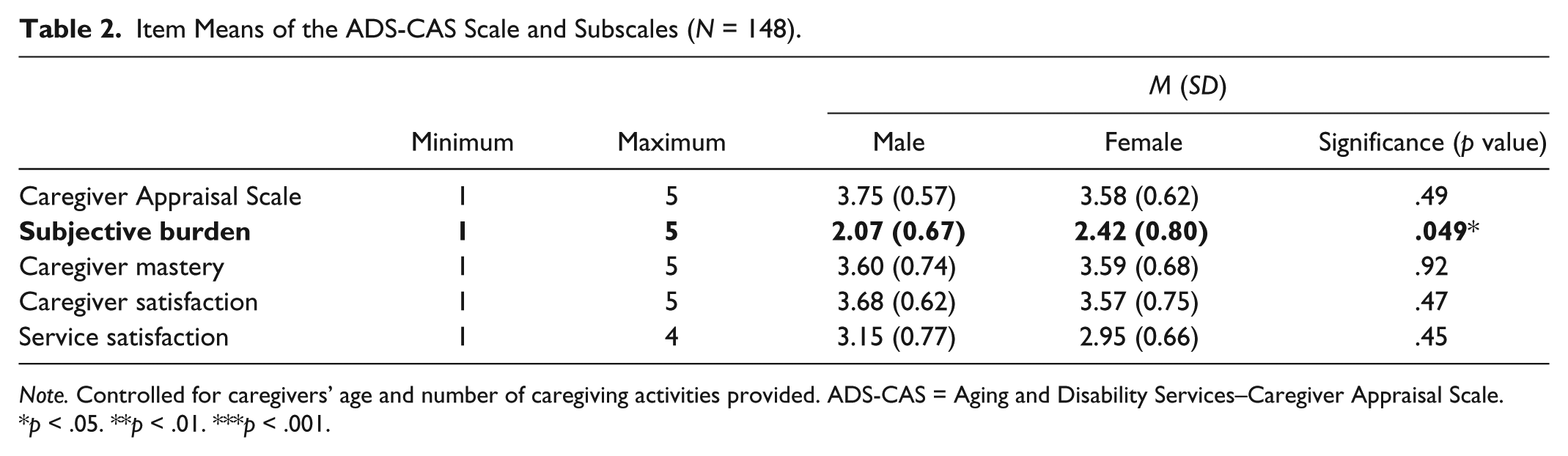
Note. Controlled for caregivers’ age and number of caregiving activities provided. ADS-CAS = Aging and Disability Services–Caregiver Appraisal Scale.
p < .05. **p < .01. ***p < .001.
Gender Differences in the Scores of ADS-CAS Among Users
A comparison of male and female caregivers’ ADS-CAS scores among those who reported using at least one type of support services (from here on referred to as caregiver users vs. nonusers) revealed similar information as findings reported above that male caregiver users, compared with female caregiver users, perceived significantly lower subjective burden (p < .05). When male and female ADS-CAS scores were compared by service category among those caregivers who used a particular category of support services, the data showed that male caregivers who used respite and supplemental services reported better outcomes than did the female caregivers who used the same service. Better outcomes for male caregivers were found in several categories, including better ADS-CAS score (p < .01), less subjective burden (p < .01), better caregiving satisfaction (p < .05), and better satisfaction toward the support services used (p < .05). For the caregivers who used counseling and education services, there were no differences between male and female caregiver users’ outcomes. No male caregivers used financial support services, so outcomes for this category of support services were not compared between male and female caregivers (see Table 3).
MANCOVA Results: Marginal Mean Differences Between Male and Female Users of a Single Service Category.
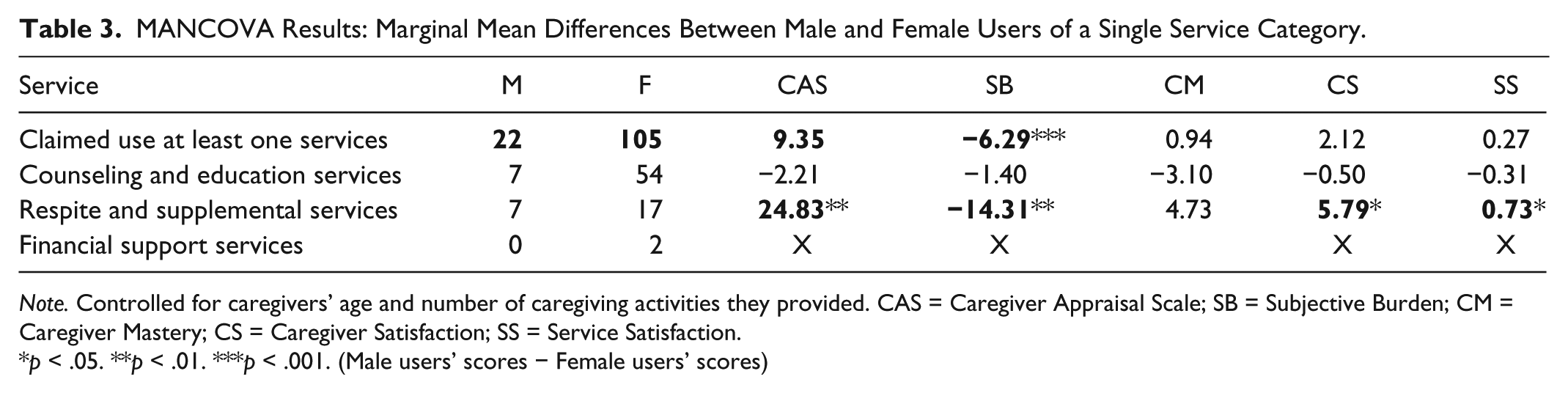
Note. Controlled for caregivers’ age and number of caregiving activities they provided. CAS = Caregiver Appraisal Scale; SB = Subjective Burden; CM = Caregiver Mastery; CS = Caregiver Satisfaction; SS = Service Satisfaction.
p < .05. **p < .01. ***p < .001. (Male users’ scores − Female users’ scores)
Gender Differences in Mean Scores of Outcome Measures (ADS-CAS) Between Users and Nonusers of Services
Further analysis of use of caregiver support services between users and nonusers of services revealed different outcomes for male and female caregivers. Use of family caregiver support services seemed to result in more significant effects for female caregivers than for male caregivers (see Table 3). After controlling for caregivers’ age and the number of care activities provided, female caregivers who used at least one type of service showed significantly lower scores in ADS-CAS (p < .01), caregiver mastery (p < .05), and caregiver satisfaction (p < .05) than did female caregivers not using any service. For male caregivers, those who used at least one type of service showed no difference in outcomes from those who did not use any service.
An analysis of service categories revealed additional statistically significant relationships. The female caregivers who used services in the counseling and education category only perceived less subjective burden (p < .05) than did other female caregivers. Female caregivers who used only respite and supplemental services showed lower caregiver mastery (p < .05) and caregiver satisfaction (p < .05) than did those not using respite services. Last, female caregivers who used only financial support services showed better appraisals (higher total scores) on the ADS-CAS (p < .01), and perceived greater caregiver mastery (p < .05) and caregiver satisfaction (p < .01) than did those caregivers not using any financial support services (Table 4). The results of our analyses are presented in Table 4 as mean score differences between users of services and nonusers, and between users of a single service category and nonusers of that same service category.
MANCOVA Results: Marginal Mean Differences Between Male and Female Caregiver Service Users of Any Services and Nonusers, and Users of a Single Service Category and Nonusers of That Service Category (Male = 27; Female = 121).

Note. Controlled for caregivers’ age and number of caregiving activities they provided. CAS = Caregiver Appraisal Scale; SB = Subjective Burden; CM = Caregiver Mastery; CS = Caregiver Satisfaction; SS = Service Satisfaction.
p < .05. **p < .01. ***p < .001. (Users’ scores − nonusers’ scores)
Discussion
The different findings reported by male and female caregivers adds to the growing body of research in caregiving support and provides suggestions for further service development for male and female caregivers. In the current study, male and female caregivers provided different types of care to their care recipients and used different types of caregiver support services. After controlling for caregivers’ age and the number of caregiving activities provided, the findings from the current study reveal that gender differences played a role in caregiver appraisals. Chen (2009) reported that use of different services was associated with different levels of caregiver appraisal, and findings from the current study provide further information regarding gender differences in caregiver appraisals. In the following sections, we further discuss the different outcomes associated with male and female caregivers’ use of different caregiving support services.
Counseling and Education Services
Female caregivers seemed to benefit more than male caregivers from using counseling and education services. In the current study, female caregivers’ subjective burden tended to be higher than that reported by male caregivers, consistent with reports from other studies that female caregivers perceived greater strain and burden from caregiving than did male caregivers (Kao, 2003; Kao & McHugh, 2004; Kramer & Kipnis, 1995; Lawrence et al., 2002; Nagatomo et al., 1999; Wallsten, 2000; Zahid & Ohaeri, 2010). This trend remained among the caregivers in the current study who used at least one type of support service and among those who used respite and supplemental services but not any other type of service. However, the discrepancy between male and female caregivers’ perceived subjective burden becomes nonsignificant among caregivers who used counseling and education category only. Further analysis revealed that female users of counseling and education category only reported a significantly lower subjective burden (p < .05) than female nonusers, but no differences were found between male users and nonusers. These findings could indicate that use of counseling and education services is beneficial for female caregivers, while the effect of using such services for male caregivers is less obvious. Research findings have shown that counseling and education services are effective in helping caregivers deal with their own psychological needs and improve their relationships with care recipients (Brodaty et al., 2003; Burns et al., 2003; Coon, Thompson, Steffen, Sorocco, & Gallagher-Thompson, 2003). The findings in the current study support this previous research and further indicate gender differences in outcomes of using counseling and education services with further empirical evidences.
It is also important to note the possibility that female caregivers who already perceive less burden may be more likely to use this type of service. Those caring for a recipient with more severe disabilities and those who have fewer sources of caregiving help may perceive a higher burden and therefore have less energy to use counseling and education services (Markle-Reid & Browne, 2001; Toseland, McCallion, Gerber, & Banks, 2002). However, a recent caregiver report (AARP, 2009) showed that female caregivers who provided care for more than 21 hr a week and who perceived a higher caregiver burden were more likely to use counseling and education services. The report also pointed out that female caregivers are more likely than male caregivers to provide intensive care and provide many hours of care (AARP, 2009). Therefore, the findings from the current study may indicate that female caregivers, more than male caregivers, become more aware of their needs and seek counseling and education services to support themselves to survive as caregivers. Further study to establish a stronger causal inference is merited.
Respite and Supplemental Services
Although male caregivers did not seem to benefit as much as female caregivers from using counseling and education services, they did seem to benefit from using respite and supplemental services. Among caregivers using respite and supplemental services, male caregivers had higher scores on the ADS-CAS, lower subjective burden, higher caregiver satisfaction, and higher satisfaction toward the services they used than female caregivers. In addition, male caregiver users of respite and supplemental services showed better caregiver mastery than male caregivers who did not use these services. What we did not expect was that female caregiver users of respite and supplemental services showed worse caregiver mastery and caregiver satisfaction than did female caregivers not using these services.
These findings could indicate that male caregivers enjoy using respite services as a means of recharging themselves, whereas female caregivers do not. If this is true, it could be due to traditional role expectations for female caregivers. Female caregivers are expected to be able to provide care and comfort to their families (Navaie-Waliser et al., 2002). Using respite services might make female caregivers perceive themselves as incompetent. Providing female caregivers with extra counseling services along with respite services may result in added benefits for female caregivers (Cox, 1997). Chen (2010) reported that caregivers who used respite and supplemental services did not report any more positive caregiver appraisals than nonusers did. The current study’s findings further indicate that male caregivers, but not female caregivers, who use respite and supplemental services do report more positive caregiver appraisals.
Financial Support Services
Female caregiver users of financial support services reported higher scores on the ADS-CAS, higher caregiver mastery, and higher service satisfaction than nonusers of such services. There were no male caregivers in this study who used this type of service. It could be that male caregivers are more likely than female caregivers to be employed (AARP, 2004). The Organisation for Economic Co-Operation and Development (2011) reported evidence that caregiving leads to lower wages, especially for female caregivers (Organisation for Economic Co-Operation and Development, 2011). Therefore, male caregivers may be more financially stable; they may not need financial support services or may not even be eligible to receive it. However, female caregivers are more likely to need financial support services and may, therefore, benefit more from this type of service. Providing financial services to caregivers is likely to offer them the opportunity to focus on their caregiving activities and to develop higher confidence and satisfaction.
Feminist theory suggests that women have traditionally been cast in the role of caregiver, as a result of traditional gender roles and rigid family structures in which women have been socialized to be responsible for various tasks (Baines, Evans, & Neysmnith, 1991). From a feminist point of view, providing financial support to caregivers could further encourage women to fulfill their role as caregivers, and thus perpetuate women’s oppression (Mackinnon, 2009). Our findings, showing better caregiver outcomes among female caregivers who received financial support services, provide empirical evidence that female caregivers perceive higher confidence and satisfaction rather than oppression when receiving financial support.
However, we should not ignore another possible explanation—that the caregivers who were able to gain access to financial support funds were competent users of the system who already had higher caregiving mastery and total ADS-CAS scores. Financial support for caregivers is a relatively new service that has been developed in the last 15 years (Doty, Jackson, & Crown, 1998). A limited number of research studies have examined the effect of financial support services for caregivers, and none has looked how gender differences influence use of these services (Eckert, Morgan, & Swamy, 2004; Mahoney, Simon-Rusinowitz, Loughlin, Desmond, & Squillace, 2004). The findings of this study encourage further investigation of the cost-effectiveness of providing financial support services to caregivers.
Furthermore, although eligibility criteria may prevent male caregivers from using financial support services, both the current study and a national caregiver survey report showed that male caregivers are more likely than female caregivers to help their care recipients with financial management (AARP, 2009). Exploring the possibility that factors other than financial eligibility prevent male caregivers from receiving financial support services could be important for future research studies.
Limitations
Several methodological issues limit the findings in this study. The cross-sectional design made it impossible to draw causal inferences. The long and variable time between the time caregivers received services and the time they responded to the ADS-CAS is a threat to validity. We recommend that future studies add a variable to assess the time between service use and survey response. Moreover, past research has found that caregivers’ perceptions of distress may be influenced by different factors at different stages of caregiving (Vitaliano et al., 2002). Therefore, a longitudinal follow-up would help to determine the optimal time to provide certain kinds of services, and this information would be valuable for future policy making.
Another limitation of this study was the low response rate of 20.4%. We have explored potential reasons for the low response rate. The first challenge is the fact that many caregivers do not self-identify with the term caregiver. That is possibly why five questionnaires were returned blank. Self-identification has been a recurring theme and challenge for implementing and evaluating family caregiver supports in the United States (Feinberg & Newman, 2006). The low response rate may also have to do with the substantial length of the ADS-CAS questionnaire. Jepson and colleagues (2005) studied the correlation between response rates and questionnaire length and suggested that questionnaires above a threshold of 1,000 words have lower response rates. Our survey questionnaire was over 5,000 words, even after we removed two subscales from the CAS.
Detailed information about care recipients was not collected for the length of our questionnaire. This may limit the generalizability of the study findings. We believe that the characteristics of caregivers in the current study may be close to the general caregiver population; the caregiver demographics in the current study show similar composition of age, gender, and number of services provided and received compared with caregiver demographics in the National Family Caregiver Study (AARP, 2004). There may well be differences in other variables, of course. Increasing the response rate in future work will be important and can be addressed by further decreasing the length of the questionnaire. Other methods that might increase the response rate in future studies include offering incentive payments, or performing follow-up.
Finally, the power to detect statistically significant differences between male caregivers and female caregivers in this study was lower than .80. This could be due to the limited number of male caregivers who responded to our survey. With further analysis, we found that if the number of male caregivers who claimed to receive services increased from 27 to 30, the statistical power to detect gender differences in caregivers’ experiences of using caregiver support service would reach .81. Also, if the number of male and female service nonusers increased to 17 and 36, the power to detect differences between service users and nonusers would increase and exceed .80 for both male and female caregivers. The number of male caregivers who responded to our survey was only about one fifth of our total study sample, which is a little less than the proportion of male caregivers surveyed in the AARP (2004) family caregiver survey. Although information from male caregivers was limited, the message conveyed through our study findings are still valuable for future family caregiver support services, especially for developing gender-sensitive services. For future studies, oversampling of male caregivers is recommended.
Conclusion
This study found gender differences in caregiver appraisal scores that add to the growing body of research in caregiver support and provide suggestions for further service development. Not only did male and female caregivers report differences in caregiving activities and use of support services but also responded differently to the support services they used. The current study findings could shed some light on future service development for caregivers of different genders. The study’s findings can also serve as a basis for more rigorous future evaluations of caregiver support services.
Footnotes
Acknowledgements
The author greatly appreciates the support and advice of Rosemary Cunningham, Margaret Casey, and all of the team members on the Family Caregiver Support Program at Aging and Disability Services. The author would also like to extend her gratitude to Senior Services, the Evergreen Healthcare-Geriatric Regional Assessment Team, the Northshore Senior Center, and the Kin on Community Caregiver Network-Caregiver Support; their gracious help made this study possible. The author is also very grateful for having great support from Dr. Health Young and Dr. Susan Hedrick.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.