
Abstract
Ghana, a lower-middle income country that is still grappling with fertility and birth rates, initiated family planning for the youth decades ago. This mainly targeted deprived communities, and the Muslim youth were also exposed to contraception. However, contraception awareness among the Muslim youth has had difficulties and repercussions. Against the social and economic challenges facing the Ghanaian Muslim youth, this article evaluates their awareness about contraception focusing on the issues and their ramification with the aim of identifying prospects for development. The findings reveal that awareness is high but not in a positive sense as the general patronage among couples is low, while among the unmarried, the awareness has negatively affected their morality. Among the issues, there is a disconnection between service providers and the community while some Muslims think that contraception can reduce the Muslim population and is un-Islamic. It was argued that contraception is permitted for Muslims provided there is ethical justification and that in view of the social and economic challenges, including school dropouts and Muslim child migration due to the poverty of parents, the Muslim youth must plan their childbirth. Hence, it was recommended that government must tackle the problem of education in Muslim communities. The Ulama should also dialogue with the service providers to create trust between the health providers and the Muslims.
Introduction
The use of family planning by Muslims has received much attention in the past (Mahmood, 2012; Mir & Shaikh, 2013; Omran, 1992; Roudi-Fahimi, 2002, 2004; Sato, 2007). Muslim population increases over the years and the concomitant worries about the socio-economic development of Muslim communities have been a major focus of Islamic scholarly discourse on contraception. Since the 19th century, populations in Muslim countries have grown progressively, although slowly, due to armed conflicts and the obvious increases in deaths (for example, in 1947, 1,000,000 Kashmiris were exterminated and between 250,000 and 300,000 in Jammu region were massacred between August and October, 1947, alone; see Chatta [2010]; meanwhile, since 2007, more than 35,000 people have died in Pakistan all due to armed violence). In sub-Saharan Africa, the situation is sometimes worrying because, due to poverty, Muslim population increases have resulted in slums in Muslim communities. Nowadays, Muslim majority countries are, generally, characterized by birth rates, which, although are still high, are falling gradually due to increase in gender education and literacy, medical services, and community health and sanitation platforms (http://islamicus.org/family-planning/). While some countries have the resources to cater for increasing populations, others with limited resources fear the impact of population increases on their ability to provide certain services adequately for their citizens.
Ghana is a Muslim minority and secular country. Due to high sexual freedom, the youth are facing many reproduction challenges. It is on record that 16% of all births in Ghana are unwanted, 40% are unplanned, and 24% are mistimed (Ghana Statistical Service [GSS], Ghana Health Services [GHS], & ICF Macro, 2009). Approximately 55% of married Ghanaian women are at risk of unintended pregnancy (Johnson & Madise, 2011). Hence, single-parenting, school dropout, and sexual and reproductive immorality are a cause for concern. According to the GHS, about 750,000 teenagers between the ages of 15 and 19 got pregnant in the past 12 months due to unprotected sex (http://www.ghanaweb.com/GhanaHomePage/NewsArchive/artikelphp?ID=292643). The Graphic Online (14 May 2013) quotes the above as an annual figure. As at 2012, with a total fertility rate of 4.15 births per woman, Ghana’s population growth was estimated at 2.2% ranking 42nd in the world (Central Intelligence Agency [CIA], 2013). This places Ghana’s population growth rate ahead of known densely populated countries like China, India, Indonesia, Pakistan, and Bangladesh (CIA, 2013). Ghana’s birth rate of 32 per 1,000 persons ranks 39th in the world, again, ahead of the above countries (CIA, 2013). In terms of death rate, however, Ghana ranks lower as 110th in the world (CIA, 2013). According to the CIA world report, birth rates beyond two children per mother indicate a growing population size. With the above birth rate, therefore, Ghana’s population is deemed to be growing beyond normally expectation. The 2010 National Population Census results depicted a population increase of 30.4% in the previous decade (GSS, 2012). With this growth rate, Ghana’s population is expected to double in the next 28 years (GSS, 2012). Urban dwellers formed 50.9% of the total population as at 2010 (GSS, 2012), with rapid urbanization projected at 60% by 2015 where this percentage of Ghanaians will be expected to live in urban settlements with over 5,000 people (Farvecque-Vitkovic, Boakye, Raghunath, & Eghoff, 2008). This implies that the number of settlements with more than 5,000 people in Ghana may increase soon because those with the above number will grow beyond this threshold to become urban centers (Adarkwa, 2012).
With the current rate of unemployment, the above trend of population growth poses a challenge (Imoro, 2009) and has many implications for the provision of social services and points to many complicated issues. In the first place, health expenditure formed 10.6% of the country’s GDP with a physician ratio of one physician per over 1,000 persons and hospital bed ratio of one bed per over 1,000 persons in 2009 (CIA, 2013). As at 2008, children under age 5 who were underweight constituted 14.3% (CIA, 2013). A huge percentage of expenditure on education is borne by the government. However, as at 2010, Ghana’s expenditure on education took only 5.52% of the country’s GDP (World Bank, 2012). This was a reduction over the 2008 figure of 5.74% and an increase over the 5.3% of 2009; yet, it is projected that the total expenditure on education will have to be on an average of 8.6% of GDP by 2015 to achieve the desired impact on education delivery in the country (Lewin, 2008, as cited in the Education Sector Performance Report 2010, Ghana, p. 94). A cost-sharing scheme introduced in public universities in 1997 has since increased parents’ responsibilities toward their wards in tertiary institutions; while graduate unemployment has resulted in the formation of many pressure groups among university and polytechnic graduates. Currently, over 50% of Ghana’s revenue is used to pay public sector workers (http://www.ghanaweb.com/GhanaHomePage/NewsArchive/artikel.php?ID=292553), what then is left for development? This has led to heavy reliance on foreign donors for development and heavy public debts by governments.
Ghana initiated the policy of controlling the population back in 1969 (Johnson & Madise, 2011; Stanback & Twum-Baah, 2001) through family planning. The initial response was sluggish, but by 1988 the acceptance rate had been 5% and 13% by 1998 (Stanback & Twum-Baah, 2001) and increased slowly to 25% by 2003 (Johnson & Madise, 2011). This was in recognition of the fact that fertility, mortality, and migration are the main demographic variables that interact to increase population (Asante-Sarpong, 2007). Whether low, stagnant, or high, population growth affects a country’s state of development and standard of living. With an improved fertility rate, researchers posit that Ghana is potentially high populated country (Asante-Sarpong, 2007). Currently, pressure on land resources is increasing because population density rose from 79 in 2000 to 103 persons per square kilometer in 2010 (GSS, 2012). According to the GSS (2012), the increase in population density means there is more pressure on social and infrastructural facilities in the country. As at 2010, 65.3% of Ghanaian men were breadwinners of their households, but this responsibility started shifting to the women since 1970 (cf. GSS, 1970, 2012).
The above issues have enormous implications for the Muslim youth. In many Muslim households, large family sizes have been a drain on the economic resources of the men who are unable to cater adequately for their families, especially children (George, 2007); consequently, the Ghanaian Muslim youth and for that matter the young Muslim generation are facing many social and economic challenges culminating in crimes in Zongos (a Hausa term for Muslim communities; Middleton, 1980; Schildkrout, 1978). This has obliged government’s attention. Due to limited economic resources, population growth is perceived as a hindrance to sustainable development and poverty reduction. Ghana’s current Muslim population is 4,345,723 (17.6%; GSS, 2012) and, therefore, in trying to achieve quality family planning for sustainable development, Muslims have not been neglected. The sensitization of the youth on birth-control mechanisms toward quality reproductive health and upbringing of children for quality standard of living has, thus, not excluded the youth in Zongos. Ghana’s “youth” is defined as the people of the 15 to 35 age bracket (Ministry of Youth & Sports, 2010). This definition is informed by those used by the United Nations Organization and the Commonwealth Secretariat. They are the most vulnerable age group in reproductive matters due to HIV/AIDS and sometimes unprepared parenthood. However, reproductive sexual awareness among the Muslim youth has not been without difficulties and repercussions. Against the background of the social and economic challenges facing the Ghanaian Muslim youth, this article evaluates their awareness about contraception focusing on the issues and their ramification with the aim of speculating on prospects for positive development. As sexual immorality among the present Muslim youth has been a debilitating problem in many countries (Ahmad & Akhter, 2006; Ahmad & Ezzeddine, 2009; Harun & Hasan, n.d.), in an era of HIV/AIDS, research in this direction is not untimely.
Methodology
The research is both qualitative and quantitative. According to Denzin and Lincoln (2000), quantitative approach measures causal relationships and usually involves numbers or statistics. It is an objective gathering of data and examination of social phenomena in statistical terms (A. T. Schwandt, 2005). On the other hand, qualitative research is an “empirical inquiry into meaning” (Ospina, 2004, p. 1280; Shank, 2002, p. 5). It is descriptive in nature and involves the gathering and examination of data in terms of meaning, rather than statistics (Denzin & Lincoln, 2000; Ogier, 1998, 2002; Punch, 2005). Nkwi, Nyamongo, and Gery (2001) define qualitative research as “ . . . any research that uses data that do not indicate ordinal values” (p. 1). However, the above definition of Nkwi et al. of qualitative research is a bit problematic because since the so-called “paradigm wars” of the late 1970s, 1980s, and even the 1990s (Gage, 1989), many qualitative researchers have objected to the use of numerical data in qualitative research on grounds of perceived incompatibility with constructivism in research (Patton, 1990; R. S. Weiss, 1994), yet others like Howard Becker and Martyn Hammersley have supported what Becker called “Quassi-statistics” to make expressions like “some” and “most” more precise (Becker, 1970; Denzin & Lincoln, 2000; Hammersley, 1992; Maxwell, 2010). It is, therefore, safer to say that qualitative research does not make use of complex or detailed numerical or ordinal values. This is because A. T. Schwandt (2007) indicates unambiguously that “ . . . qualitative studies can and often do make use of quantitative data” (p. 251). Conventionally, quantitative procedure is considered to be the more scientific approach to social science research which relies on specific definitions and operationalizes the meanings of specific concepts and variables (B. Berg, 2007). The mixed method (tagged “triangulation” by Denzin, 1978) in the late 1970s was used to validate the findings. It was assumed that a piece of information corroborated by two or more autonomous measurement procedures certainly reduces the uncertainty of its interpretation because the most persuasive testimony might come through a “triangulation of measurement processes” (Bryman, 2003; Webb, Campbell, Schwartz, & Sechrest, 1966) and this is in consonance with the prophetic maxim that the Ummah (community) cannot agree (i.e., have consensus) on an error (Hasan, 2003; Ibn Majah, Sunnan, hadith no. 3950; Ibn Taymiyah, 1966; Maududi, 1983).
Data were gathered from 200 married Muslim couples of the 21 to 35 age brackets and 100 unmarried Muslim females of the 15 to 35 age brackets in 17 Muslim communities in the three northern regions, Brong Ahafo, Asante, Central, and Western Regions. Due to the low level of education among Muslims in Ghana, the instrument used was interview. Random sampling was used without respect to educational level or employment choices. Their education levels, however, ranged from primary six to first degree; 45 had at least secondary school certificate. The married couples were sampled for their awareness and view on contraception, that is, the extent to which they have used it or not. Every marital home was treated as one entity. Sexual immorality is becoming a problem in Ghanaian Muslim communities. Consequently, the unmarried were sampled for the impact of contraception on this section of the society. The data were examined in both qualitative and quantitative (statistical or numerical) terms. Simple statistics were displayed to validate the arguments and authenticate the findings. Due to the sensitive nature of the issue, family planning, informants were given full assurance of anonymity, but not, I must say, at the expense of competent details of information. In terms of structure, we first looked at an Islamic view of contraception, then examined the challenges of the Muslim youth in Ghana for Islamically ethical justifications for family planning, the awareness of the youth about contraception and the challenges it poses to the unmarried, prospects for development, and conclusion.
An Islamic View of Contraceptives
As a religion founded on ethical values, Islam places high premium on marriage which is understood as a lawful sexual relationship (intimacy and companionship) and an avenue for reproduction. A lawful marriage is compulsory (wajib) for the capable Muslim because it is a Qur’anic command (nass): And if you fear that you shall not be able to deal justly with the orphan girl then marry (other) women of your choice, two or three, or four; but if you fear that you shall not be able to deal justly (with them), then only one or (slave) that your right hands possess. That is nearer to prevent you from doing injustice. (Qur’an 4:3)
A prophetic tradition (hadith) says that he who marries fulfils half of his faith (Tirmidhi, Sunnan, hadith no. 3096). Another hadith quotes prophet as saying that marriage was his Sunnah so whoever does not marry is not of him (Al-Ghazali, 1939; Ibn Majah, Sunnan, hadith no. 1846). Thus, failure to marry when of age and can afford is disapproved (makruh) for Muslims. The objective of Islamic marriage is for sexual intimacy (Al-Ghazali, 1939; Al-Kawthari, 2006; Qur’an 30:21) and procreation (Qur’an 16:72). A hadith commands Muslims to marry women who are both loving and fertile for procreation (Abu Dawud, Sunnan, hadith no. 2043; Al-Ghazali, 1939; An-Nasai, Sunnan; hadith no. 1966; Ibn Majah, Sunnan, hadith no. 1861). While the object is not to denigrate women who for no reason of theirs cannot have children, the above hadith emphasizes the import of childbearing in Islam. The Prophet entreated Muslims in another hadith that they should multiply for him to be proud over the followers of other prophets on the Day of Judgment (Al-Ghazali, 1939; Ibn Majah, Sunnan, hadith no. 1846). In spite of this, he also indicated that “one of the two reasons of wantlessness is less number of family members. One of the two reasons of poverty is having too many persons [to take care of]” (Al-Ghazali, 1993, p. 19). This implies that having fewer numbers of offspring one can adequately cater for is a social necessity in Islam.
The word “contraception” is not mentioned in the Qur’an although it is not a modern technology. Yet, no specific verse opposes it. However, some Muslims extend the Qur’anic verses (81:8-9; 17:31) that prohibited wa’ad al-banat (female infanticide) to discourage contraception. However, the context must not be neglected. The verses specifically refer to the pre-Islamic practice of killing female children for fear of feeding “unproductive” mouths, an unfortunate response to women’s vulnerability in times of war and plunder. History attributes the origin of this practice in Arabia to an Arab chief whose daughter was taken captive after he lost a battle. The daughter refused to come back to her father after she was ransomed on account of her marriage with a man she loved. This made the chief (who obviously could not bear the embarrassment) to resolve that he would never allow his daughters to see their eighth birthday (he would bury them alive before the age of eight). As time went by, other Arab tribes copied this practice and so it became a normal ritual for those who did not want to have female children to get rid of them by burying them alive before the age of eight (Subhani, 1984). However true this story may be, it is worth noting that contraception (other than abortion) whatever form it takes does not involve killing an infant. In the view of Imam Al-Ghazali (1939), in his Ihya’ ‘Ulum-ud-Din, the male sperm alone or the female egg alone cannot be said to be human beings until they are united by fertilization in the uterus through what he calls “offer and acceptance” (ijab wa qubul). Further, there is no surety that every sperm or egg blocked through contraception would have been fertilized. At the same time, even in the days of infanticide some children still survived, and this boils down to Allah’s power to create amply referred to in Qur’an 36:82.
Many traditions refer to the practice of azl (coitus interruptus) among the companions. Some scholars use Qur’an 81:8-9 and 17:31 to prohibit azl, while others refer to a hadith in which Judamah bint Wahb said the Prophet was asked about azl and he replied as follows: “it is a minor infanticide . . . ” (Imam Bukhari), but Imam Ibn Hajar A.A.A. (n.d.), in his Al-Fath-ul-Bari bi Sharh Sahih-ul-Bukhari, reveals that some scholars consider the above hadith as da’if (weak) while others regard it as mansukh (abrogated). Also, in the Sunnan of Tirmidhi (hadith no. 1136), the prophet is reported to have denied the view of the Jew at the time that azl was a minor infanticide. Furthermore, while the Prophet in his own words prohibited infanticide (wa’ad), the wording of the above hadith does not constitute a clear command or text (nass) to be used as the basis for prohibiting azl. Again, according to Abu Baraa’, in his Al-Ma’lum min ad-Din bi-d-Darurah, the hadith “whoever castrates himself is not one of us” in Sahih-al-Muslim (also reported by Al-Bukhari) was in response to a Bedouin who disliked practicing azl as a mechanism for preventing pregnancy and so sought permission from the Prophet to go for castration (ikhtisa) as a permanent contraception. The implication is that, azl may be disliked but it is preferred to a permanent method. The classical scholars, except Ibn Hazm (1970) whose position was later questioned by Ibn Qayyim (n.d.) and others, opined that the Prophet did not prohibit it, and this represents the earliest legal reasoning of Muslims on contraception which indeed has been a useful ingredient for the legal debate on modern Islamic perspective on family planning. However, among the four schools there is some degree of dislike (makruh) which is removed when genuine need for it arises but none of them prohibits it (Al-Kawthari, 2006). In this light, the use of contraceptives is not a sin for Muslims (Al-Ghazali, 1939; Ibn Taymiyah, 1966). Using the four tools of analogy (qiyas), that is, asl (origin), far’ (the branch), ‘illa (the cause/reason), and hukm (the judgment; ref: Ambali, 1998), one observes that modern contraceptives serve the same purpose and reason as azl and so, ethically, contraception is not prohibited for Muslims. The source (asl) of reasoning about contraceptives is azl. Modern contraceptive like condom is a branch (far’) of or resulted from a technological improvement over azl. The common reason (‘illa) underlining both azl and condom, and by extension, today’s contraceptives, is to prevent pregnancy. Hence, the final decision (hukm) is that contraception is permitted for Muslims. However, avoiding conception through permanent deactivation of a reproductive organ (e.g., vasectomy and tubal ligation) is inconsistent with the prophetic sunnah (based on the hadith in which the Prophet prohibited castration [ikhtisa]; Bukhari, hadith no. 4786 & Muslim, hadith, no. 1402), hence is disapproved unless one is in the state of medical necessity (darurah). However, any other contraception, like intrauterine device, that does not alter the physical structure of the reproductive organ or does not artificially damage or expel an already formed foetus after insemination is permitted. Based on this, the Maliki School prohibits the use of medicine to prevent pregnancy (Illish, n.d.) Hence, they do not permit emergency contraceptives. Multiplying children as an act of honor to the Prophet is recommended (mandub or mustahabb) if one can afford but not duty (wajib or fard). Here too, the context is very important. During the time of the Prophet, the number of vibrant youth or young ones in the Ummah was paramount for the sustenance of the nascent Muslim community. To a very large extent, even during that time, the quality of the Muslim population overrode or was preferred over the quantity. One may try to understand this by reflecting over the event that occasioned the withdrawal of Abdullah ibn Ubayy, the Madinan hypocrite, and his 300 supporters from the camp of the Muslim army during the battle of Uhud which left only 700 Muslim soldiers to face about 3,000 soldiers of the Quraysh. Other than the above, it will be impossible to reconcile the reports in sound traditions that the prophet knew that some of his companions practiced azl which he did not prohibit them from (Al-Ghazali, 1939). Hence, if economic constraints exist or are foreseen, birth control could be a valid option because it is consistent with the section of Qur’an 2:185 that says: “ . . . Allah intents ease for you and does not want to make things difficult for you . . . ” (Qur’an 4:28 & 22:78).
The Islamic concept of maintenance (nafaqah) is a heavy responsibility. The prophet said: “no body will meet God with a greater sin than with a sin of keeping his family members [children] uneducated” (Al-Ghazali, 1993, p. 26). According to Al-Ghazali, few people will be able to escape this danger (Al-Ghazali, 1939). The Islamic family maintenance and its implications for parents make the need to have fewer numbers of offspring one can adequately cater for a social necessity in an Islamic setting. For this reason, Muslim scholars give a catalog of what could provide halal grounds for birth control. These include maintaining the woman’s beauty, preventing the birth of many children to avoid poverty and enhance quality care, and economic difficulties (Al-Ghazali, 1939; Al-Kawthari, 2006; Omran, 1992). Consequently, the next topic exposes the challenges of the Muslim youth in Ghana with the prospect to uncover the justification for contraception or family planning for the positive development of the Muslim communities.
Social and Economic Challenges Facing the Ghanaian Muslims Youth
Marriage is a respected institution in Ghanaian culture as it is in many traditions. A married person commands respect among colleagues. It is a pride for the youth because it marks the beginning of a socially acceptable platform for the adult responsibility of childbearing in the cultural context (Ikamari, 2005). Among Muslim women, marriage is both a religious duty and a social transition from girlhood to adult womanhood. Hence, some of the young ones now prefer flamboyant marriages (to simple) ones where they can see visible symbols of marriage status including the wearing of wedding rings in public. For the men, marriage symbolizes responsibility in society. Usually childbirth is expected within the first 2 years after marriage and some new couples get worried and tongues start wagging if they are unable to get their first baby within 3 years after marriage.
Despite the lofty regard for marriage and childbirth, parental responsibility has been a problem for the Muslim communities in Ghana due to unemployment and poverty. Generally, men’s responsibility for their families began reducing since 1970 and the decline was steady in the last decade when the latest census was taken in 2010 (cf. GSS, 1970, 2012). This has implications for Ghanaian Muslim communities where many women are petty traders, subsistence farmers, or housewives. Many Muslim children of school-going age fend for themselves resulting in high school dropout (Imoro, 2009) and the female is more vulnerable (Bashiru, 2012). It is in recognition of this dropouts due to poverty that the Ghana government initiated the policy of free tuition, and quite recently, the School Feeding and Capitation Grant all initiated as part of the Free Compulsory Universal Basis Education (FCUBE) started in the late 1996 (Sottie & Awasu, 2011). The above phenomenon is dominant in the three northern regions (Figure 1) where larger numbers of Muslims reside.
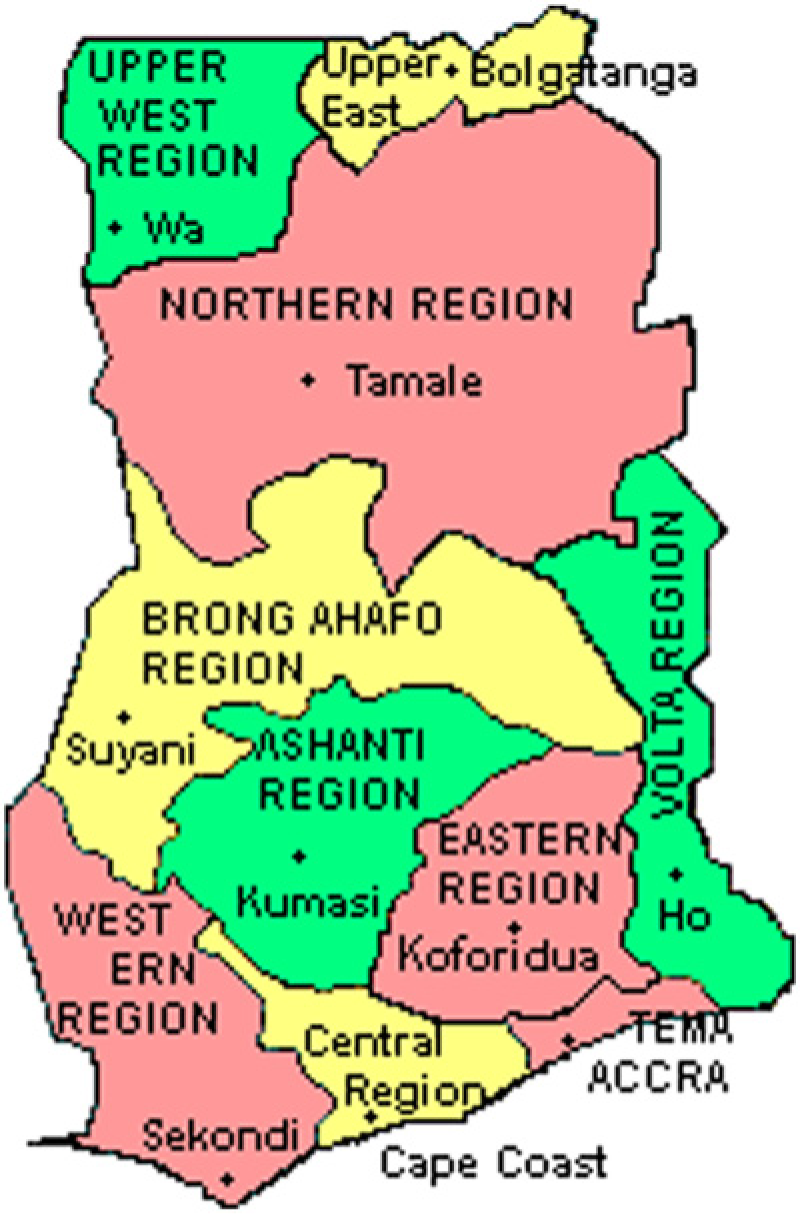
Regional map of Ghana.
The rate of school dropout in Muslim dominated communities is unacceptable (http://gbcghana.com/?id=1.1393204). A brief presentation of available statistics here will help to appreciate this point. In 2008, the national dropout rate was 4% after previous year’s enrollment in Primary 1-6. This was more than 3% increase on the dropout rate in 2003 (Government of Ghana, UNICEF, 2012). In the 2008 Ghana Demographic and Health Survey, 850,000 Ghanaian children between 6 and 11 years were out of school. This increased to 1,000,000 for the 6 to 14 year bracket (Government of Ghana, UNICEF, 2012). Other research quoted 863,524 for the 12 to 14 age group alone in 2005 and 2006, while 1,989,910 was quoted for the 6 to 12 brackets (Casely-Hayford, Ghartey, & SfL Internal Impact Assessment Team, 2007). The three northern regions alone took up to 20% of the out-of-school population in the 6 to 11 brackets while the Northern (predominantly Muslim; GSS, 2012) Region alone took 10.6% of the national out-of-school population (Casely-Hayford et al., 2007). The Upper East and Upper West took 5.4% and 3.36% respectively. The Northern Region alone had 50% of the out-of-school children in the three northern regions (Casely-Hayford et al., 2007). Research statistics gathered in this period indicated that there were more children out of school than were in school in the north and this increased for the out-of-school population in the Junior Secondary School age bracket (Casely-Hayford et al., 2007).
The relevance of school dropout in the three northern regions in this discussion is the fact that no reliable statistics on out-of-school or dropout in Muslim communities are available now. However, these regions host a huge percentage of the entire Muslim population in Ghana (i.e., 47%; GSS, 2012). Hence, this gives us a reliable picture of the situation. Muslims form 60% of the population in the Northern Region (which is, territorially, the biggest region in Ghana and the most populous of the three northern regions) and top the chart in Upper West, while in the Upper East, they are the second largest religious group outnumbered marginally by traditional religionists (GSS, 2012). It could be observed that in the Upper West and East regions where the Muslim population is lower (compared with the Northern Region), the out-of-school populations are as well lower, while the out of school population in the Northern Region is very high. This is due to poverty which is endemic in the three regions. According to the GSS, poverty reached 84% in Upper West, 64% in Upper East, and 42% in Northern Region (Naami & Mikey-Iddrisu, 2013). Apparently, the Northern Region is a bit urbanized; nonetheless, only 4% of children in the poor quintile from this region complete basic education (Wumbee, 2007). In 2001, the GSS indicated that of 2,314 street children aged 5 to 17 years interviewed in a survey, more than a third (38.1%) came from Northern Region alone (Kwankye, Anarfi, Tagoe, & Castaldo, 2009). In Asante Region, the activities of school dropouts in the dominant Muslim Zongos of Aboabo and Alabar in Kumasi are well known (Child Research for Action and Development Agency [CRADA], n.d.), while those of Nima and Mamobi in Accra, the capital city, need no emphasis. The burglary activities of unemployed youth have tainted the image of the Zongos (Effah, 1991), and Muslim clerics including Alhajj Ahmad Sadat and the National Chief Imam Shehu Usman Nuhu Sharubutu have expressed serious concerns (H. Weiss, 2007). This must have also informed the late Vice-President Alhaji Aliu Mahama’s famous campaign against indiscipline and the heading of the 7th September 2005 edition of The Ghanaian Chronicle (an authoritative news paper in Ghana) titled “Veep Worried About Islamic Names in Crimes,” a report on a speech delivered on his behalf by Alhaji Mambila at the 13th Annual Celebration of the 105th birthday of Sheikh Ibrahim Inyass by the Tijaniyyah Muslim Community in Kumasi. Quality education guarantees a sound livelihood and the need to adequately educate one’s children is a duty of all Muslims.
Unemployment has increased rural–urban migration of teenagers particularly from the Muslim northern Ghana (Kwankye et al., 2009; Wouterse, 2010). There have been incidents in which Muslim girls from northern Ghana are raped in Kumasi and Accra and also the market of Kasoa where they migrate to sleep on the streets, uncompleted buildings, and kiosks to work as kayayei (market load-carriers; Kwankye et al., 2009; Salome, 2010) and “iced-water”(cold water) sellers. These Kayayei are mostly Muslims girls (C. Berg, 2007). Pick-pocketing, begging (H. Weiss, 2007), and other nefarious juvenile activities have become rampant in Zongos. Others resort to prostitution to make a living and end up with teenage pregnancy to increase the burden of the society (Kwankye et al., 2009). The quality of caring for children is a chain: When one is properly catered for at infancy, the chances are that one may become productive to be able to also cater for one’s offspring. Conversely, if one is neglected at infancy due to “opportunity cost” over the scramble over limited family resources, one might possibly become poor and hence perpetuate the existing poverty in the family and the society at large in the long run. Unfortunately, this phenomenon is having negative impact on Muslim communities in Ghana due to large numbers of dependents on individual families leading to increase in poverty.
This invariably affects both the qualitative and quantitative development of the Muslims and misplaces the objective of multiple childbirth and marriage in Islam which is to increase the Muslim population without losing the core objective of marriage (i.e., quality number of offspring). In this era of terrorism, the concentration of poor, underprivileged, and unemployed population is a challenge to every government. The problem of young, unemployed Muslim youth causing mayhem in Zongos has already been a source of worry. Having fewer children to adequately cater for thereby contributing to quality population that will develop and make Muslim communities attractive instead of quantity that has been retrogressive will reduce the above socio-economic challenges. This justifies the need for the vulnerable reproductive youth to effectively plan their families. However, the question is “what is the extent of awareness of this vulnerable group on or their readiness to adopt family planning mechanisms?” The next topic assesses the Muslim youth’s awareness about and attitude toward contraceptives with the prospect to revisiting the challenges for positive development.
Awareness of the Muslim Youth, Issues, and Challenges: Findings and Discussion
In spite of the numerous challenges enumerated, some Muslims view contraception as a technology of the Western secular world, which is inconsistent with the Islamic tradition (M. Y. T. Tanko & M. Suhair-Hasan, Kumasi, Asante Region; Y. Armiyau, H. Fusseini, & A. Yusuf-Arhin, Cape Coast; O. Abu Bakr & S. Zakariau, Kasoa, Central Region; T. H. Salifu, Wa, Upper West Region; F. Oyibi-Lantei, M. Mamudu, S. A. Sumaila, & L. Safura, Accra, Greater Accra Region: personal communication, February 11-27, 2013) and could possibly reduce the Muslim population, a fundamental view which affirms Muslim women’s role as child bearers (Mazrui, 1994, as cited by Gyimah, Adjei, & Takyi, 2011) and caretakers. Apparently, the above describes an upset expressed over the provision of birth-control services, by organizations, some of which receive financial support from foreign or Western-based agencies.
Contraception is known to virtually all Ghanaian adults. However, in Muslim communities, contraception has not been received by many couples with ultimate priority. Based on the natural desire of some Muslims to beget many children and the fear of its impact on the Muslim population together with inadequate knowledge, contraception and its use for birth control are low on the scale of priorities for many Muslim couples. However, it is known to an overwhelming majority. In a random sample of 200 Muslim couples aged between 21 and 35 years in 17 Muslim communities (Zongos) in the three Northern Regions, Central Region, Western Region, Brong Ahafo Region, and Asante Region on their latent awareness on contraceptives, the results provided in Table 1 were recorded.
Couples’ Awareness of the Existence of Contraceptives in Ghana.

From Table 1, it can be noted that contraceptive awareness among the married Muslims is high. A huge percentage of 93.5 is aware of contraception as a facility for reproductive health. This partly confirms the existing demographic finding that awareness about contraception in Ghana is almost applicable to all-and-sundry (GHS, 2009; GSS et al., 2009; GSS, Noguchi Memorial Institute for Medical Research, & ORC Micro, 2004; Opoku, 2010; Opoku & Kwaununu, 2011; H. M. Schwandt, 2013). Of the 13 who responded “not aware,” 10 were unwilling to express an opinion on contraceptives seeing it as a private issue. However, it was not surprising because for many people, discussion on sexual and reproductive issues, particularly contraception, is not desired (Glover et al., 2003). Of the 187 couples who expressed awareness about contraceptive mechanisms, 134 had between 3 and 6 children. Of these, 57 representing 42.5% are in polygamous marriage. They fell within the age bracket 21 to 35. Again, of the 187, only 37 representing 19.8% who were mostly educated were known to be on contraception. Asked about whether contraception is Islamic, some of them said it is un-Islamic but they have no choice. This means that they are using it out of necessity and not religious merit. Of the 37, 29 representing 78% live in Zongos in Accra, Kumasi, Cape Coast, Takoradi, and Tamale which are all urban and education centers.
It is, therefore, probable that Muslim couples residing in urban communities like Nima, Madina, Taifa, and Accra New Town all in Accra; Kotokuraba and Abora in Cape Coast; Afiakuma in Takoradi; Aboabo, Alabar, and Asawase in Kumasi; and those in Tamale and the adjoining urban or education centers are more likely to have better knowledge and access to reproductive health care than their colleagues in remote and rural areas. Table 2 provides data on access to reproductive health facilities.
Couples Accessing Health Professionals on Reproductive (Contraception) Issues.
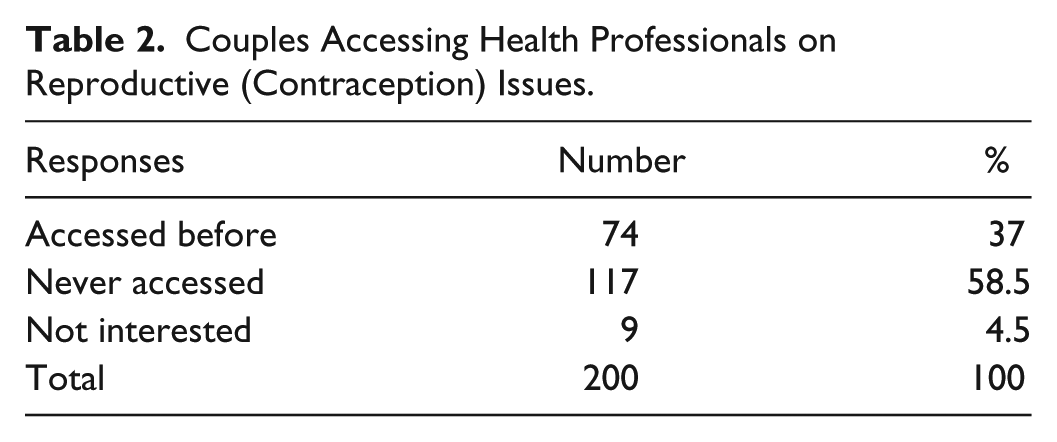
Table 2 gives a picture of the access of reproductive health personnel by Muslim couples in Ghana; although they have the awareness, they do not access professional reproductive health personnel for briefing. Only 74 couples representing 37% indicated having encountered health professionals on reproductive issues. Most of the couples who have ever accessed health professionals live in urban Zongos; 4.5% were not interested in such a venture. However, in some cases, the women were interested but their husbands did not cooperate with them. The majority (58.5%) have not consulted health professionals on contraceptive issues before. This response confirms the existing finding that the patronage of contraceptives among Ghanaians is generally low (Asante-Sarpong, 2007; GSS et al., 2004; Opoku, 2010; Opoku & Kwaununu, 2011). Strangely, some women do not even deliver their babies in hospitals but in herbal centers. The cultural orientation cannot be disconnected from these idiosyncrasies; however, the health authorities are also blameworthy due to their approach in reaching-out to the general populace. In spite of the increasing talks on family planning and contraceptives, there is a distance between the health care providers and the people (Stanback & Twum-Baah, 2001).
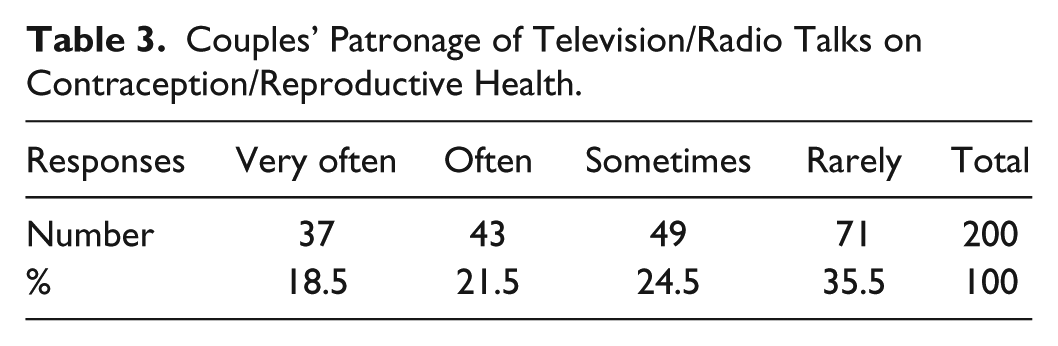
The health care providers sometimes use the media to reach-out to the public. There are numerous health talks on both FM and TV stations. The role of TV and radio in disseminating messages to the public cannot be underestimated. However, the use of these media as the main avenues for the education on family planning and reproductive health issues has not been very effective for some Muslim couples.
From Table 3, 35.5% rarely show interest in TV/radio health talks. While only 18.5% constantly listen to health talks on TV and radio, 24.5% probably watch only in their free times or probably when they are available. In the first place, how many couples in the Zongos have access to TV as individuals? On the other hand, some also indicated that they have lost interest in media health talks. Possibly, the TV and radio stations must revisit their health programs and be more particular with the professional expertise of the people they host in their talks. Herbal practitioners have overtaken the professional health authorities in exploiting the media to their own advantage. Some herbal practitioners are called “doctors” on Ghanaian radio and TV health programs when they are not qualified medical doctors. According to some of the respondents, such programs rather predispose viewers to health dangers (M. Abdul-Fatah, B. Abdullah, & M. M. Abu Bakr, Kumasi, Asante Region; H. Issa, Tamale, Northern Region; R. Kasim, M. Lukuman, & A. Lukuman, Takoradi, Western Region; M. M. Sani & I. Munkaila, Upper East Region: personal communication, May 16-18, 2013). Others argued that some of the sexual and reproductive health talks for the youth on TV and radio are fraught with obscene language and visuals. Some of the respondents specifically mentioned radio programs like “wo ba ada anaa” on “Peace FM” and “odo ahomaso” on “Adom FM” which are all nationwide FM stations as very informative on sexual reproduction but are fraught with very obscene languages. In sexual and reproductive matters, it appears that the secular Ghanaian society has slipped-off the ethical boundaries due to the fashion of secularism and globalization. For the Muslims, and for that matter, the typical Ghanaian, reproductive issues have a moral language of their own and that the improper use of sexual language is seen as moral depravity. However, it seems this traditional philosophy has been overlooked due to the increasing sexual and reproductive challenges facing the youth. This poses a challenge because the Islamic concept of taqwa (fear of God) is deeply grounded in ethical values. The Qur’an calls on Muslims to withdraw from fasad (immorality): But as for him who feared standing before his Lord, and retrains himself from impure evil desires and lusts; surely, paradise will be his abode. (Qur’an 79:40-41)
Couples’ Patronage of Television/Radio Talks on Contraception/Reproductive Health.
Muslims are to avoid vulgar talks. A tradition of the prophet said: “Let him who believes in God and the Last Day say what is good or be silent” (An-Nawawi, Arba’in al Hadith, hadith no. 13, related by Bukhari and Muslim) and withdrawing from such scenes is symbol of nobility.
For they have been guided (in this life) to the purest of speeches; they have been guided to the Path of Him Who is Worthy of (all) Praise. (Qur’an 22:24)
This seems to make the conscientious Muslims to withdraw, which invariably impacts on their reproductive life. Interestingly, 127 of them indicated that they like listening to health talks involving Muslims where the health talks of the owner of the Ameen Scientific Herbal Clinic, Sheikh Ameen Bonsu, were constantly mentioned.
Contraception as Immoral Stimuli for the Muslim Youth: The Other Side of the Coin
Among the Ghanaian Muslim youth, sexual immorality has been a functional reaction to the technology of contraception, and this has constituted, perhaps, the greatest challenge. In this era of sexually transmitted diseases (STDs) like HIV/AIDS, reckless heterosexual relationships should have been on the farther side of the youth. However, the existence of condom has lured the youth into a sense of security in sexual and reproductive matters (Kitissou, 2012). The implication is that people feel sexually unrestricted by the scare of STDs provided they could consistently use this device (Fiaveh, 2012). As a result, while condom provides a means for delaying pregnancy to ensure quality upbringing of children and help couples living with untreatable STDs, it has also facilitated promiscuity among some married and unmarried Muslim youth. Condom promotes promiscuity, predisposing one to intercourse with even infected people (Green, 2003). Kitissou was therefore aptly right in intimating that “ . . . condom use is positively and significantly related to promiscuity, . . . ” (Kitissou, 2012, p. 3) as it is rather used by the unmarried youth although that should not have been the case. Hence, the improper use of this device could put the Muslim community in many dangers, including HIV/AIDs and teenage pregnancy as some of these condoms, which are often imported from China, have been reported as substandard (ref: http://www.ghanaweb.com/GhanaHomePage/NewsArchive/artikel.php?ID=289186; Zheng, 2010).
In this regard, abortion drugs become the main supplements to condoms (Glover et al. 2003). Conspicuously, perhaps, under such circumstances, the perception of its impact on the Muslim population is null and void. Of a total of 100 unmarried Muslim females across those regions interviewed, 77%, aged 15 to 35 years, indicated that they have used some tablets to prevent pregnancy after unsafe sex (due to condom failures). Of this figure, more than 50% indicated that they have used emergency contraceptives more than once and this indicates in minute details the extent of reproductive immorality among the present Ghanaian Muslim youth. Asked about whether in this era of HIV/AIDS they would consider having premarital or extra-marital sexual relations if contraceptives were not present, 59% indicated that they would not have sexual affairs outside marriage while others indicated that they will never like to have children before or outside marriage. This implies that the existence of contraception, particularly condom, as a protection against pregnancy and STDs has impacted negatively on the reproductive morality of the young sexually active Muslims in Ghana. The state of premarital affairs of the youth in Zongos called for the involvement of some Imams and Zongo Chiefs in the fight against HIV/AIDS and teenage pregnancy in the Eastern Region (Parkes, 2001). Hence, for the health security of the unmarried youth, the government and the health authorities should reappraise the content of health education on contraception and reproduction. This is important at this time when some of the condoms are adjudged to be substandard.
Prospects for Positive Development
As Ghana’s developmental agenda aims toward upper middle income status and beyond in the 21st century, collaboration and cooperation from all are necessary for achieving this national goal. With the current sexual and reproductive attitude of the youth (of which the Muslim youth are no exception) and its social, economic, moral, or health implications, such a goal cannot be achieved without diligent collective effort and a revisit of our viewpoint. Where are the possible directions to face in harnessing these challenges for development? Five issues come up from the above discussion.
Secular education has an impact on the Muslim’s attitude toward contraceptives and positive awareness of sexual and reproductive issues. The respondents who are currently on contraception are secularly educated. As a primary step toward positive reproduction awareness, the government should invest in education in Zongos as poverty is responsible for the low level of education in Ghanaian Muslim communities. Educational incentives can help in tackling the issue from the roots. This requires the government empowering and resourcing the Islamic Education Unit of the Ghana Education Service (GES) to make it more relevant to the communities in which it operates.
Sexual and reproduction education in the media could continue, but to make positive impact, health authorities should not concentrate their effort in the media alone but should push it into the domain of the society itself. To whatever degree, this cannot be achieved by educating Muslim women at the Market alone while neglecting the men, but by, for example, creating mini-youth centers with relevant personnel in the Zongos. The media must also be circumspect in their reportage. In some cases, cautiousness in media reporting about community issues, in general, is seriously compromised. Expressions like “ . . . will soon be a thing of the past” are everyday expression in media report on social issues; when in some cases they are only a step. Such reports make the agencies swollen-headed and feel they have done enough when in reality very little effect is reaped.
It was also noted that many of the respondents prefer watching or listening to reproductive health programs involving Muslim medical teams. In this case, the health authorities must leave no stone unturned in reaching out to the Zongos and the guests must include Muslim medical or resource persons. These personnel can attend to the religious issues which often come up in discussions relating to family planning.
Some Muslims have misconceptions concerning contraception in general. Hence, within the Muslim community itself, the Sarikis (Hausa name for the Muslim community Chief) and the Ulama must be involved. The need to factor religion into the contraception debate has already been emphasized in previous research (Gyimah et al., 2011). To understand this dimension, one might refer to Mbiti and Parrinder when they concurred that the African is notoriously and incurably religious (Mbiti, 1989; Parrinder, 1962). To this end, for intervention programs to be fruitful, apart from Islam, the religious dimension must not be overlooked. In this regard, an internal dialogue is necessary. The Ulama have different views about contraception in Islam just like the ordinary Muslims. Hence, there is the need for internal dialogue facilitated by a committee of Ulama to revisit the opposing views and reconcile them to dispel the notion that Islam opposes contraceptives. In 2012, Ethiopia made magnificent success when a national fatwa asserting that family planning is not prohibited in Islam was declared by the Ethiopian Islamic Affairs Supreme Council (EIASC)/Ethiopian Ulama Council (https://www.xcdsystem.com/icfp2013/program_FD/index.cfm?aID=2119&;seID=415). The Ulama and the Islamic organizations must be major intervention partners in this regard. The advocacy and peer-education training packages produced by service providers should be evaluated from Islamic perspectives, contextualized, and adapted to the Ghanaian Islamic social context. The outcome of this discussion by the Ulama should be adopted, printed, and translated into the major ethnic languages, disseminated and discussed at both the regional and local levels. In implementing social intervention programs in Muslim communities, ethical trust is very important for Muslims. Hence, it was not for no reason that three predominant northern Muslim states in Nigeria boycotted polio vaccination in 2003, which created a global health crisis (Kaufmann & Feldbaum, 2009). Muslim intellectuals and religious and community leaders should be represented in health discussion both on TV and radio and should be major partners in both the design and implementation of such programs. Furthermore, there should be health forums in Muslim communities so that people without access to radio and TV can also be reached. The National Commission for Civic Education could be resourced to take this responsibility in collaboration with the health authorities and the Ulama.
To allay the undesired consequences of contraception among the unmarried, parents should show concern about the sexual misconduct of their children and counsel them till they marry. The Muslim organizations must also initiate da’wah programs to tackle the negative impact of condoms on the unmarried section of the community.
The above steps could contain the issues and challenges concerning contraceptives and sexual awareness among the Ghanaian Muslim youth and help to ensure a good planning of Muslim families to contribute quality and morally upright population that will contribute to Ghana’s positive development in the 21st century.
Conclusion
This article examined the awareness of the Ghanaian Muslim youth about contraception and reproductive matters against the social and economic challenges they are facing with the aim of identifying prospects for development. The findings show that awareness is high but not in a positive sense because the general patronage among couples is low while among the unmarried, the awareness has negatively affected the morality of some of the youth. Issues identified include the fact that there is a disconnection between the service providers and the community while some Muslims perceive contraception as something that could reduce the Muslim population and are, therefore, unsure of its ethical legitimacy. It was argued that, certainly, the perception for the survival of the human person is central to Islamic marriage, and indeed, the whole human thought in Islam and producing many children is an ultimate expression of this instinct (Lari, n.d.) and indeed an affirmation of the need to increase the Muslim population amply recommended by the prophetic traditions. However, the necessity to qualitatively cater for these numbers places a certain obligation on Muslim parents that overrides any other consideration and reaffirms the core objective of marriage and childbirth in Islam (i.e., quality and developed community). Hence, it was upheld that contraception is permitted for Muslims provided there is ethical justification, and in view of the social and economic challenges Ghanaian Muslims youth are facing resulting in unacceptable numbers of out-of-school Muslim children population, hazardous migration of Muslim children in search of non-existent decent livelihood, begging, among others, due to poverty and unemployment of Muslim parents, there is the need for the present Muslim youth to effectively plan their childbirth to give attractive and adequate livelihood to their offspring. Formal education was seen to have positive impact on attitude to contraceptive and reproductive issues, hence, it was recommended, among others, that the government must tackle the problem of education in the Zongos. The Ulama must also dialogue with the service providers to reconcile the religious and secular divergences to create the ethical trust between the health providers and the Muslims while safeguarding the community’s ethical standards.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.