
Abstract
The aim of this pilot study was to evaluate if the residents of psychiatry and clinical psychology from the city of Buenos Aires knew any of the existing mental health Clinical Practice and Treatment Guidelines (CPTGs). We asked residents their opinion about CPTGs and, also, if they followed their recommendations in clinical practice. We asked 59 mental health residents (28 physicians and 29 psychologists) with different years of clinical training to fill a questionnaire to know their opinion about CPTGs and also if they follow the CPTG recommendations in their clinical practice. We found that 79.31% of residents did not know any CPTG. Eighty percent of the residents who did know any CPTG have a positive opinion about CPTGs. Finally, the American Psychiatric Association Guidelines were the most known CPTGs. The authors emphasize the need for a clinical guidelines diffusion policy in Buenos Aires city and particularly as a clinical and training resource for mental health residents.
Since the 1980s, evidence-based medicine (EBM) is helping healthcare practitioners to use scientific evidence for the clinical decision making, by integrating individual clinical expertise with the best external evidence (Field & Lohr, 1992; Levant et al., 2006). In relation to this perspective, many Clinical Practice and Treatment Guidelines (CPTGs) were developed as an effort to provide a systematic, critical, and updated review of the results of research to assist physicians in clinical practice (American Psychiatric Association, n.d.; National Institute for Health and Clinical Excellence, n.d.).
The interest in CPTGs has increased in most medical specialties–including psychiatry—and with less success in the psychological field, even when the movement in favor of evidence-based psychotherapy gained momentum (Chambless & Ollendick, 2001; Pilling, 2008). One of the main benefits of CPTGs is the offer of a systematic and updated summary of evaluation and treatment data of different disorders, a task that could otherwise be overwhelming for the clinician (Forsner et al., 2010; Grimshaw et al., 2004). As a consequence, the use of CPTGs could improve the quality of care of patients by transferring recent advances in medical knowledge into everyday clinical practice and by helping in the selection of the most appropriate treatment option (Grimshaw et al., 2004; Mellman, 2001; Woolf, Grol, Hutchinson, Eccles, & Grimshaw, 1999). In addition, CPTGs could be used as an educational tool for residents by introducing essentials and authoritative recommendations for their first years of clinical practice (Yager, Docherty, & Tischler, 1997).
Nowadays, there are several CPTGs, covering a broad range of mental disorders, mainly those with higher prevalence (Gaebel, Weinmann, Sartorius, Rutz, & McIntyre, 2005; Gelenberg, 2010). A detailed consideration of differences between CPTGs largely exceeds the purpose of this article, but we would like to highlight several points concerning CPTGs in Argentina. In the first place, CPTGs developed in Argentina barely meet basic methodological standards. Usually, they are the synthesis of local expert consensus and they are not based on any statistical systematic review of randomized controlled trials (RCTs; Garay & Korman, 2008). In those cases in which empirical analyses were taken into account, the analyses were greatly limited by the lack of local data, which is attributed to the sparse development of empirical research in the country. Finally, some CPTGs are supported by a governmental authority, but their use is not mandatory, and therefore an adequate dissemination is lacking.
In Buenos Aires city, the General Direction of Mental Health published the “Orientative Procedure Guidelines for Clinical Practice in Mental Health”–Guías de Procedimientos Orientativaspara la Práctica Clínica en Salud Mental (Dirección General de Salud Mental, Ministerio de Salud, 2006a, 2006b, 2006c). The authors were mental health specialists, including service chiefs of mental health services of public hospitals, where the residents of our sample worked at the time we applied the questionnaire. These guidelines were of particular concern to us as the residents of our sample at the time we applied the questionnaire were training on those public hospitals, and consequently it was expected that residents would be familiarized with these CPTGs. These CPTGs cover several disorders, but it is worth mentioning that their therapeutic recommendations, although adapted to mental health facilities and resources of our city, closely resemble those suggested by the American Psychiatric Association (APA), and provide only slight specificities related to the idiosyncrasy and cultural background of the inhabitants of Buenos Aires.
Although CPTGs seem to be a useful resource to assist healthcare professionals and improve their practice (Grimshaw et al., 2004; Weinmann, Koesters, & Becker, 2007), many studies found a low degree of adherence to CPTGs, and it soon became clear that publishing a CPTG was not sufficient to guarantee its use (Bero et al., 1998; Cabana, Rand, Powe, Wu, & Wilson, 1999; Grimshaw et al., 2004; Michie et al., 2007). Obviously, a preliminary step to address this issue is to make clinicians acquainted with the existence of CPTGs (Jaffe & Yager, 1999). Then, active and complex strategies proved to be necessary for disseminating, promoting adherence, and sustaining the use of CPTGs (Caminiti, Scoditti, Diodati, & Passalacqua, 2005; Craig et al., 2012; Forsner, Wistedt, Brommels, & Forsell, 2008; Forsner et al., 2010; Weinmann et al., 2007). Continuing medical education (CME) programs, audits, manual or computerized reminders, case-based expert-supervision or institutional mandatory use, were all associated with positive effects in changing physicians’ practice and having them incorporate CPTG recommendations (Craig et al., 2012; Forsner et al., 2008; Prior, Guerin, & Grimmer-Somers, 2008). Specifically aimed at teaching APA Guidelines to residents, Garfield et al. proposed training programs based on resident/peer teaching as an effective way for this purpose (Garfield, Atre-Vaidya, & Sierles, 2002).
Lack of adherence to CPTGs has been attributed to many factors. As we mentioned, one of the most common reasons is the lack of awareness of the existence of CPTGs (Jaffe & Yager, 1999). Other limiting factors often cited include reluctancy to change the clinician’s parameters of practice, concerns about quality of CPTGs or about the probity of their authors (Cosgrove, Bursztajn, Krimsky, Anaya, & Walker, 2009), or disbeliefs about the expected benefits of applying the CPTG recommendations (Falzer, Garman, & Moore, 2009). Forsner et al. (2008) listed barriers influencing the implementation of CPTGs. The authors divided them into factors related to the organizational resources (i.e., no agreement on the need to use CPTGs, guidelines not mandatory, lack of clear intervention goals, no regular implementation meetings, lack of facilitation), factors related to healthcare professionals’ individual characteristics (i.e., negative attitudes toward CPTGs, fear of loss of autonomy and of standardization of care, concerns about relevance of evidence for own patients, lack of specialized training), and factors related to the perception of guidelines and implementation strategies (i.e., credibility of content, lack of familiarity with CPTGs).
Another limitation we can mention is that most CPTGs have a biomedical approach that may be inapplicable to some theoretical frameworks–that is, the psychoanalytic or psychodynamic theories (American Psychological Association, 2002). This fact is especially important in our area of interest, being Buenos Aires a place where psychoanalysis has developed in almost every area of mental health practice (Korman, Viotti, & Garay, 2010). Adaptation of CPTGs to a different context to that from which they were originally developed has also been found to be a limiting barrier (Fervers et al., 2006; Ruggeri, Lora, & Semisa, 2008), unless a previous evaluation of their appropriateness was conducted.
As part of a larger investigation, we conducted a survey which aimed at obtaining information about the local situation concerning the implementation of CPTGs in Buenos Aires. We focused on the knowledge and use of CPTGs by mental health residents of the city of Buenos Aires. The Mental Health Residency System is run by the Training Direction (Dirección de Capacitación) of the Ministry of Health of the city of Buenos Aires. It employs physicians (“residents of psychiatry”) and psychologists (“residents of clinical psychology”). They are distributed into 14 public hospitals, including general and psychiatric hospitals. Residents must complete a 4-year training, there are about 45 places per specialty, and it is a public program that pays salary to every resident. The training relies on lectures from annual courses organized by the Mental Health Residency Coordination (Coordinación de las Residencias de Salud Mental) and on courses organized by each of the hospitals that host a residency program. Along the 4 years, every resident must rotate between urgency and psychiatric inpatients wards, outpatient units, consultation and liaison services and primary care and rehabilitation programs. Virtually every rotation and course as well as supervision and organizational meetings, are shared by physicians and psychologists.
The aim of this study was to inquire if the residents of psychiatry and clinical psychology in the city of Buenos Aires (Argentina) know any of the existing CPTGs and their opinion about their clinical usefulness.
Materials and Method
Participants
During 2009 to 2011, 65 mental health residents were asked to voluntarily participate in this study, and their identity remained anonymous. Table 1 shows the characteristics of the sample. Fifty-nine mental health residents completed the questionnaire—29 physicians and 30 psychologists—whose training took place in four public general hospitals. According to years of clinical practice, 25 had less than 2 years of practice, 12 between 2 and 3 years, and 22 more than 3 years. The main theoretical framework indicated by physicians was “eclectic” (48.28%), which includes the answers where more than one theoretical frame was subscribed (i.e., biological and psychodynamic psychiatry) and biological psychiatry (20.69%). Among psychologists, the main theoretical framework was psychoanalysis (76.7%).
Characteristics of the Sample.
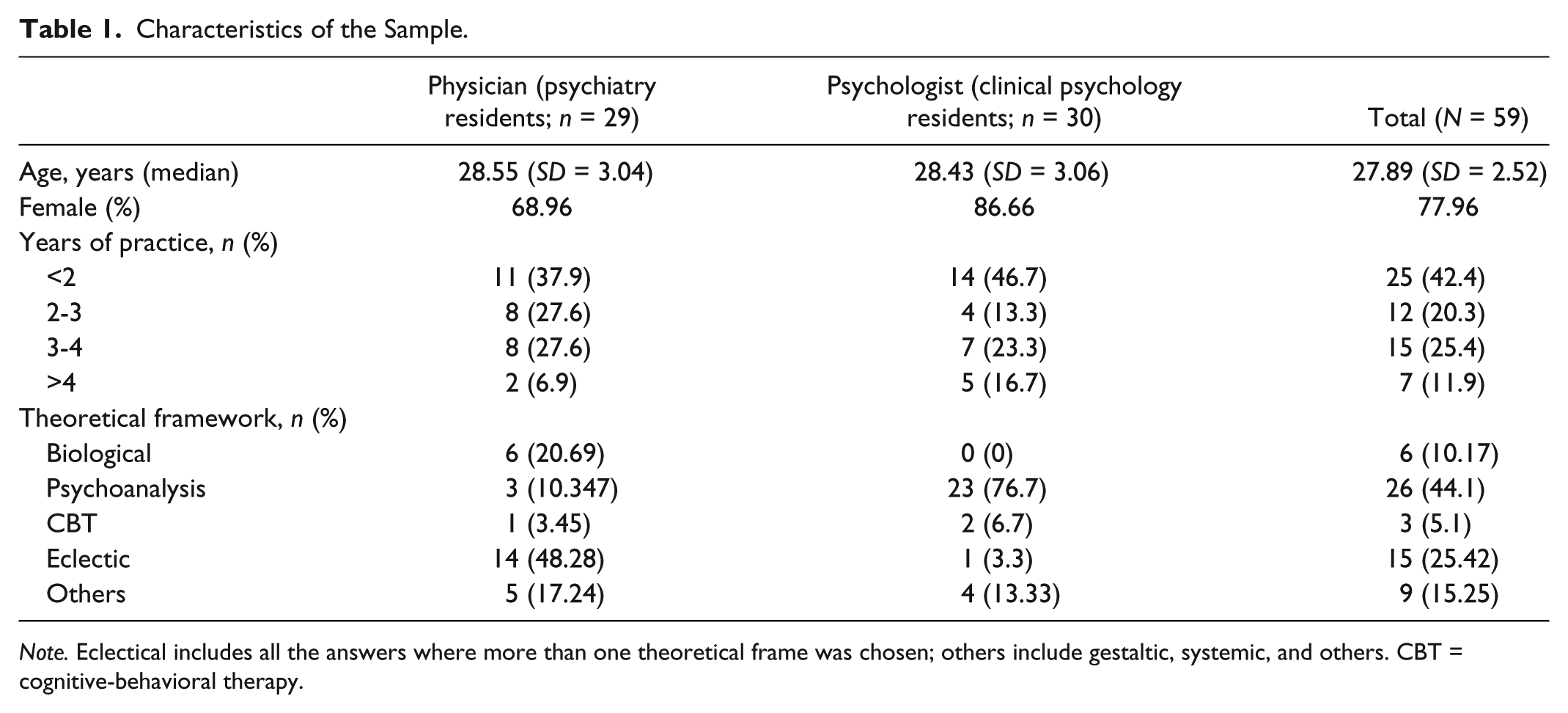
Note. Eclectical includes all the answers where more than one theoretical frame was chosen; others include gestaltic, systemic, and others. CBT = cognitive-behavioral therapy.
Measures
We elaborated a self-administered questionnaire (see appendix), which included open and closed questions based on three aspects: knowledge of CPTGs, attitude toward CPTGs, and use of CPTGs. We asked if the resident knew about CPTGs, which CPTG they knew, their opinion about CPTGs, and the impact that CPTGs had on their everyday practice. We also asked them about other characteristics, such as years in clinical practice and main theoretical framework. We chose “years in clinical practice” instead of “year of residency training” because many of them usually have previous clinical experience before entering the residency training program, which could imply a higher knowledge of CPTGs. Finally, the main theoretical framework was an essential piece of data because psychologists and psychiatrists define themselves quite rigorously as adepts of one psychological and/or psychiatric theory. The survey was financially supported by a research grant of the University of Buenos Aires (UBACyT P412 Project).
Procedure
The participants had to return the questionnaire on the same day they received it to assure a high response rate (90%).
Data Analysis
The data were analyzed in a descriptive statistically way.
Results
Knowledge of CPTGs
Of the total sample, only 16.95% knew CPTGs (13.3% of psychologists and 20.69% of physicians). According to their theoretical framework, CPTGs were only known by 1 out of 26 (3.33%) psychoanalysts, including physicians and psychologists, and by 2 out of 6 physicians with a biological framework (33.3%). Two out of two psychologists with cognitive-behavioral orientation reported knowing the CPTG (100%). Finally, of those physicians who defined themselves as having an eclectical approach, 3 out of 14 (21.43%) knew about CPTGs (Table 2). Considering data from the length-of-experience perspective, none of the residents with more than 4 years of clinical practice knew about CPTGs.
Results of the Questionnaire.

Note. Eclectical includes all the answers where more than one theoretical frame was chosen; others include gestaltic, systemic, and others. CG = clinical guidelines; CBT = cognitive-behavioral therapy.
Opinion about CPTGs
We only considered the answers of the 10 professionals who reported knowing CPTGs. Eight out of ten (80%) had a positive opinion, one (10%) had a negative opinion, and one did not answer this question. The one who expressed a negative opinion said that “the problem with CPTGs is they are developed in countries other than Argentina, and they do not represent the national cultural background, which limits their use”.
Which CPTG do they know?
Seven out of ten knew the APA Guidelines (70%), 1 knew the National Institute for Clinical Excellence (NICE) Guidelines (10%), and 1 knew the Orientative Procedure Guidelines, while 1 did not answer this question
Impact of the CPTG on everyday practice
Seven of the ten respondents who knew the CPTG use them on their everyday practice. Three respondents said that they do not use CPTGs, even though they have a positive opinion about them.
Discussion
The present study found a low level of knowledge of CPTGs by mental health residents from Buenos Aires City, showing that physicians and psychologists evidence a lack of knowledge of these clinical resources. These data are even more surprising if we consider the positive opinion expressed by residents who do know CPTGs and the fact that the majority of them found CPTGs useful in their everyday practice. This finding suggests that the underlying reasons for this ignorance may not be attributed to a critical attitude to CPTGs or to its poor clinical utility but to the insufficient and inadequate diffusion of CPTGs in our city. This is particularly true for the “local” CPTGs, as only one resident reported he knew local CPTGs.
The level of unawareness that the residents of our sample have about CPTGs is higher than what 10 years ago was reported by Jaffe and Yager in a survey made to psychiatrists who were attending an educational meeting in the United States (Jaffe & Yager, 1999). They evaluated awareness of APA Practice Guidelines and found that 16% of the psychiatrists ignored the existence of APA CPTGs. In our sample, 79.31% of physicians did not know any CPTG (83.05% from the total sample). They also found a rate of acceptance of 83% between those who had already read the CPTG, which was comparable with the 80% of positive opinion pointed out by residents in the present study. Another study (Udomratn & Srisurapanont, 2002) evaluated psychiatrists’ prescribing attitudes toward treatment-resistant schizophrenia after a passive dissemination of a specific CPTG. The authors found that 68.75% of the 80 respondents knew CPTGs although the acceptance and clinical impact were slightly lower: 70.9% and 58%, respectively. Perlis (2007) evaluated the use of Bipolar Disorder CPTGs by psychiatrist. He found that 64.1% of respondents utilize them routinely, an acceptance that was comparable with studies previously mentioned.
Forsner et al. (2010) and Forsner et al. (2008) conducted a study to evaluate compliance to Depression and Suicide Care CPTGs with an active implementation of CPTGs (which included implementation teams, seminars, regular feedback, and academic detailing) in four psychiatric clinics, compared with a passive implementation based on simply sending CPTGs to two other clinics that served as controls. They found that compliance to CPTG increased after the active implementation of different strategies, a finding already suggested in several reviews (Francke, Smit, De Veer, & Mistiaen, 2008; Weinmann et al., 2007), and in addition, it improved quality of care. Also, they reported that compliance with CPTG was sustained over the 2-year follow-up period, which could indicate certain degree of incorporation of CPTG.
Conversely, local CPTGs were only available at the official website of the city government and had little or no diffusion at all. It is somehow expected that residents would not be familiar with these CPTGs if no effort had been made to promote them. Indeed, we must state that by the time this article was written, the local Orientative Procedure Guidelines were no longer available on the website where they were originally published but remain as archives.
Specific issues of EBM and clinical decision making are barely taught in the courses organized by the Mental Health Residency Coordination. It is possible, especially in the case of physicians, that knowledge about empirically supported treatments may be covered in part by recommendations given by supervisors (supervisions are mandatory and frequent) and by resident-to-resident lectures. However, these educational strategies are not likely to be effective enough for influencing residents’ incorporation of CPTG recommendations (Forsetlund et al., 2009).
One respondent from our sample had a negative opinion of CPTGs and their implementation because “[CPTGs] are developed in other countries than Argentina and do not represent the national cultural background.” We believe that this perception is true if we consider the use of foreign guidelines without any further adaptation to our clinical context, a task that has never been performed in Argentina but underway in other countries (Ruggeri et al., 2008). The strongest objection to using treatment guidelines in Perlis’s (2007) study was that guidelines did not apply to the patients treated by the sampled professionals, suggesting that clinicians may perceive CPTGs do not actually address issues concerning everyday practice. The negative viewpoint about CPTGs of the respondent of our sample may arise from the lack of an aggressive dissemination policy by their own developers. As a result, mental health professionals are more acquainted with foreign CPTGs due to their higher availability from journals, books, and websites. Also, it is worth noting that Argentina does not have a strong, established tradition of research in psychopharmacology or psychotherapy research. In fact, Argentinean CPTGs do not include data from any RCT conducted in our country.
Another reason for the low level of knowledge of CPTGs could be evidence-based practice has little tradition in our mental health field. This could be due in part to the main theoretical framework of respondents. In our sample, 44.1% of respondents (including psychologists and physicians) defined themselves as psychoanalysts, which was the psychopathological theory associated with the lowest level of knowledge of CPTGs (3.85%). Psychoanalysis has a long tradition in our country, and it is established as the leading psychological theory for psychologists and, to a lesser extent, for physicians. It was somehow expected that psychoanalytically oriented professionals would be less familiar with CPTGs, as this theory does not favor the systematization of criteria for clinical decision making. In addition, psychoanalysis in Argentina is mainly influenced by Jacques Lacan’s perspective, and it has a crucial influence on psychologists in residency training.
However, we were highly surprised by the lack of knowledge of CPTGs among physicians, as medical training proposes a decision-making process related to the CPTG approach of diagnosing and then choosing a therapeutic option. However, respondents with a cognitive-behavioral orientation, although too few in our sample (n = 3) to draw any strong conclusion, were most familiarized with CPTGs (66% of knowledge), and this was especially true for psychologists (100% of knowledge). A possible explanation is that Cognitive-Behavioral Therapy (CBT) is more linked with the idea of standardized diagnostic and therapeutic criteria to guide clinical decisions.
The main limitation of the study is the small size of the sample. Although representative of demographic characteristics of residents of the mental health from the city of Buenos Aires (Torricelli, López, & Leibovich de Duarte, 2007), it does not allow us to obtain statistical significance. Nevertheless, this is the first study aimed at evaluating the knowledge and use of CPTGs by residents of the city of Buenos Aires. These results strongly alert about the low knowledge of CPTGs and the associated waste of a potentially valid and useful tool for everyday clinical practice. Also, we can think over the deficiency of specific training in this issue and in evidence-based clinical decisions in general. This is particularly relevant for residents as they are involved in a training program designed to develop clinical decision-making skills for which CPTGs are useful resources. They could also be used to teach the essentials of psychiatric and psychological treatment to trainees at all levels of experience (Garfield et al., 2002; Prior et al., 2008; Weinmann et al., 2007). Our results suggest the relevance of starting as soon as possible with a process of disseminating and implementing CPTGs in Argentina, in keeping with this growing world trend. But, most importantly, we emphasize the need to launch a culture of evidence-based practice in mental health, which should include research trials as well as the development of local guidelines.
Footnotes
Appendix
The present questionnaire is aimed to explore the knowledge mental health residents have of the clinical guidelines.
The spontaneous answer is the most valuable. We appreciate your kind contribution.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This investigation is supported by the UBACyT P412 project (2008-2010) and by the National Council of Scientific and Technological Researches (CONICET, Argentina). .