
Abstract
This pilot study involved 40 adults participating in treatment through the Northern Sydney Magistrates Early Referral Into Treatment (MERIT) Program, Australia. Standardized health outcomes questionnaires such as the Severity of Dependence Scale (SDS), Kessler–10 (K-10), and Short Form (36) Health Survey (SF36), were administered to each participant on three different occasions: pre-treatment episode, post-treatment episode, and 3 months follow-up. The study aimed to determine whether any observed benefits to participants at completion of the MERIT program were continued 3 to 6 months post treatment. Although the findings indicate that some benefits achieved throughout the treatment phase were maintained at follow-up, the pilot study has a number of methodological limitations, and as such, further research is recommended.
Introduction
The Magistrates Early Referral into Treatment (MERIT) program is a 3-month pre-sentence substance use treatment program based at a Local Court level in New South Wales (NSW). As a court diversion program, MERIT operates in accordance with the principle of therapeutic jurisprudence, utilizing interactions with the legal system and increased judicial involvement to promote offender rehabilitation (Wexler, 1990).
The MERIT program operates within a harm minimization framework in accordance with drug treatment policy in Australia, and treatment plans for participants vary dependent on factors such as the type of substance used and the severity of problems. For example, participants can engage with individual counselors, support groups (e.g., “12-step” programs), treatment groups (e.g., SMART recovery), pharmacotherapy prescribers, inpatient or outpatient detoxification programs, residential rehabilitation programs, or a combination of all of the above.
To complete the MERIT program, participants are required to engage in an agreed treatment plan to achieve their substance use goal (i.e., reduction or abstinence from illicit substances). After a 3-month treatment episode, a report is submitted to the Magistrate outlining treatment outcome, and this may be considered in sentencing.
Participants in the MERIT program are recognized as having long histories of substance use, complex psychosocial issues, and extensive criminal histories (Passey, Bolitho, Scantleton, & Flaherty, 2007). The intended goals of the MERIT program are to reduce substance use and offending behavior, as well as improve health and social functioning (NSW Department of Attorney General and Justice, 2011).
MERIT program: Health outcomes report produced by the NSW Department of Health in 2007, and Martire and Larney (2009), found a significant reduction in substance use and associated risk behaviors, significant improvements in mental, physical, and social functioning, and a significant reduction in psychological distress for participants who completed the MERIT program.
Such results provide evidence that the MERIT program is beneficial to participants while they are engaged in treatment. However, as noted by the health outcomes paper “it is not possible to say to what extent improvements in the participant’s health profiles and drug use are sustained after exit” (NSW Department of Health, 2007, p. 22). Consequently, this research project aims to address that area.
The only published research into the longer term outcomes of participation in the MERIT program has focused on criminal justice outcomes. Research into the Lismore MERIT Pilot Program found that participants who completed treatment were significantly less likely to reoffend and took significantly longer to offend than those who do not complete the program even at 12 months post treatment (Passey et al., 2007). A subsequent study utilizing a larger data set across multiple courts in NSW found that compared with “standard judicial process and sanctioning” (Lulham, 2009, p. 9), people who completed the MERIT program were significantly less likely to reoffend.
The current study aimed to determine whether any observed benefits to participants at completion of the MERIT program were continued 3 to 6 months post treatment. We hypothesized that participants who completed the MERIT program would evidence improvements consistent with previous research findings and clinical observations, for example, reduced substance use, reduced severity of dependence on their substance of concern, improved mental and physical health, and reduced levels of psychological distress. We further hypothesized that at 3 months follow-up, participants would continue to demonstrate these improvements achieved in treatment.
Method
Participants
Ninety-two clients completed the MERIT program based at Royal North Shore Hospital, Sydney, Australia, between December 2008 and July 2011. Fourteen of these clients were not asked to participate in the study as they did not complete the required questionnaires at either Entry or Exit to the MERIT program. Questionnaires were not administered if it was clinically inappropriate to do so; for example, if clients were currently suicidal or acutely psychotic. Of the 78 clients who were eligible for the study, 72 provided consent and 40 participated in the follow-up study. The 40 participants were aged between 20 and 47.
Treatment
Participants received approximately 12 weeks of substance use treatment as well as assessment and treatment of common comorbid psychological disorders. Treatment predominantly involved weekly counseling and regular urinalysis testing, as well as inpatient detoxification, residential rehabilitation, and/or opioid replacement therapy.
Measures
Severity of Dependence Scale (SDS)
This measures dependence on the principal drug of concern as identified by the participant. It focuses on psychological aspects of dependence, such as difficulty controlling use or stopping drug use. A higher score indicates a greater level of dependence (Gossop et al., 1995).
Recent drug use (frequency and amount in previous month)
Adapted from the Brief Treatment Outcome Measure (NSW Department of Health, 2004), this questionnaire provides information about frequency and amount of various drugs used in the previous month.
Kessler–10 (K-10)
The K-10 measures psychological distress (Andrews & Slade, 2001) with higher scores indicating greater levels of distress.
SF36
The SF36 scores for eight health and well-being domains: general health, mental health, bodily pain, physical functioning, role limits physical, role limits emotional, social functioning, and vitality. A higher score on a domain indicates a better state of health and well-being.
Psychiatric Diagnoses
Comorbid psychiatric diagnoses were identified through clinical interview based on the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994).
Procedure
Clinicians administered the questionnaires with participants at Entry during an individual face-to-face session. The questionnaires were repeated at Exit. Clients were then invited to take part in the post-treatment follow-up study, and written consent was obtained for those who agreed to participate. No reimbursement was offered for participation.
The questionnaires were readministered between 3 to 6 months after Exit. Participants were contacted by the MERIT staff via telephone. For 37 of the 40 participants, the questionnaires were administered over the telephone by a MERIT staff member who had not been the treating clinician. For two participants, the questionnaires were administered face-to-face, and one participant self-administered the questionnaires.
Data Analysis
Differences between scores at Entry, Exit, and Follow-Up were assessed using repeated-measures ANOVA. Two planned comparisons were used to determine whether there were significant differences between Entry and Exit, and between Exit and Follow-Up. A planned comparison between Entry and Follow-Up was not conducted as we were interested in seeing whether hypothesized changes between Entry and Exit were maintained at Follow-Up. The limited scope of this pilot study did not allow for more detailed analysis such as adjusting for participants lost at follow-up.
Participation and Attrition
Participants attended an average of 12.6 counseling sessions during their 3 month treatment episode (range = 7-20 sessions). Seven participants had between 2 and 7 further counseling sessions after completing the MERIT Program.
Out of 72 clients who had provided informed consent to be contacted after exiting the MERIT Program, 40 were successfully followed up 3 to 6 months after completing treatment, equating to a follow-up rate of 55.5% (see Figure 1). The average number of days to follow-up was 115 days (3.8 months). The period of time between Exit and Follow-Up ranged from 83 to 186 days (3-6.2 months).
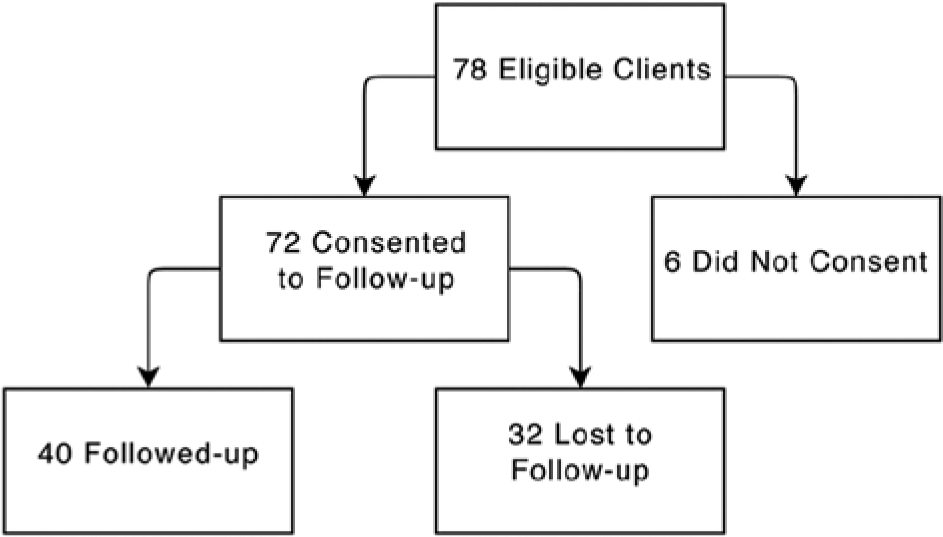
Participation in the study.
Of the 32 participants who were lost to follow-up, the majority (64%) did not answer their phone. Other reasons for attrition included the following: participants unable to complete the follow-up survey due to work commitments (7%), being in custody (2%), or not wanting to take part in the follow-up survey (2%).
Results
Sample Characteristics
Of the 40 participants, nearly all were male (87%), with an average age of 32 years (range = 20-47 years). Cannabis was the most commonly used illicit drug (80%), followed by amphetamines (33%), cocaine (25%), benzodiazepines (25%), and heroin (22%).
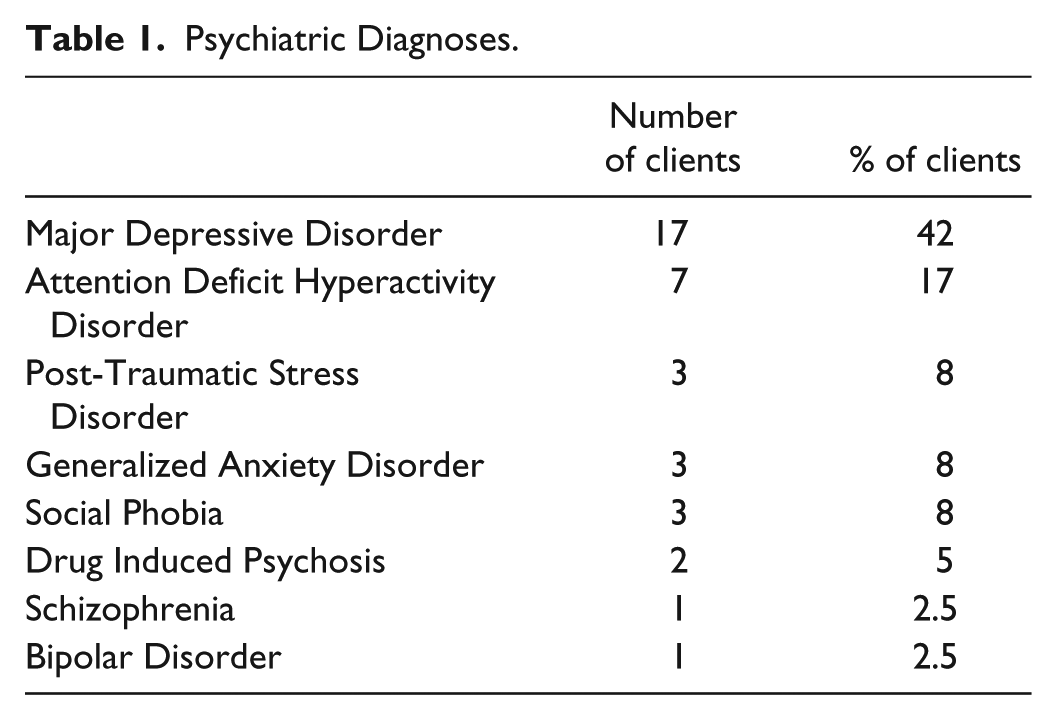
Participants were identified, through clinical interview based on DSM-IV, as having various comorbid psychological diagnoses; most commonly, major depressive disorder, attention deficit hyperactivity disorder, and anxiety disorders (see Table 1).
Psychiatric Diagnoses.
Substance Use Outcomes
Severity of Dependence
A repeated-measures ANOVA using a Greenhouse–Geisser correction determined that mean scores on the SDS differed significantly between time points, F(1.771, 39) = 18.939, p < .0005 (see Figure 2). Planned comparisons revealed that the mean score at Exit (5.8) was significantly lower than the mean score at Entry (8.2; p < .05), and the mean score at Follow-Up (3.5) was significantly lower than the mean score at Exit (5.8; p < .05). There were 19 participants (47.5%) who scored 2 or less on the SDS at Follow-Up.
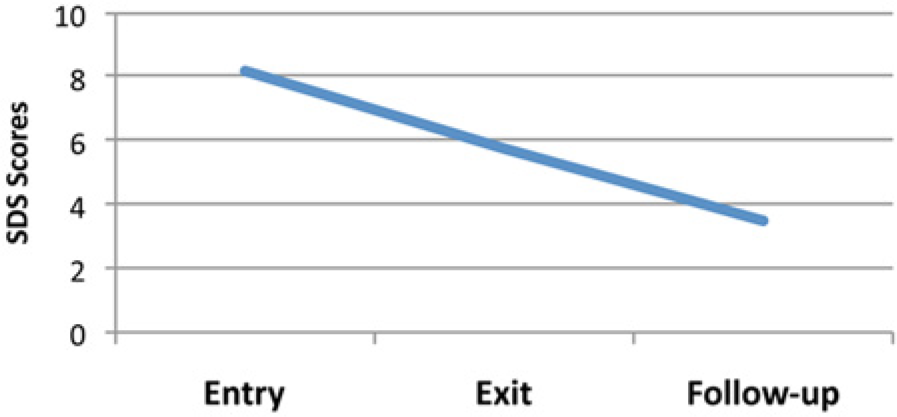
Mean scores on the Severity of Dependence Scale at Entry, Exit, and Follow-Up.
Recent Average Drug Use
The only significant difference between means for drug use at Entry and Exit was for cannabis (see Table 2). Analysis revealed that the difference between average cannabis use at Exit was significantly lower than at Entry, F(1.25, 39) = 14.058, p < .0005. At Entry, 32 participants reported using cannabis an average of 291 times per month, compared with 31 times per month at Exit and 46 times per month at Follow-Up. For the remaining illicit substances, the average number of times that they were reportedly used per month decreased between Entry and Exit, although these differences did not reach statistical significance. No significant differences were found for average drug use between Exit and Follow-Up.
Average Number of Times a Drug Was Used in the Month Prior to Entry, Exit, and Follow-Up.

Statistically significant reduction in average cannabis use between Program Entry and Program Exit.
Other Clinical Outcomes
SF36
As represented in Table 3, there were significant differences (p < .05) between average scores at Entry and Exit for six of the domains, namely, general health (54.7 increased to 66.8), mental health (49.0 increased to 62.2), role limits (physical; 55.9 increased to 78.3), role limits (emotional; 38.5 increased to 64.0), social functioning (54.9 increased to 67.4), and vitality (42.4 increased to 55.7). Furthermore, there were significant differences (p < .05) between Exit and Follow-Up for mental health (62.2 increased to 73.3) and social functioning (67.4 to 79.6).
Results of ANOVA for the Eight Domains of the SF36.
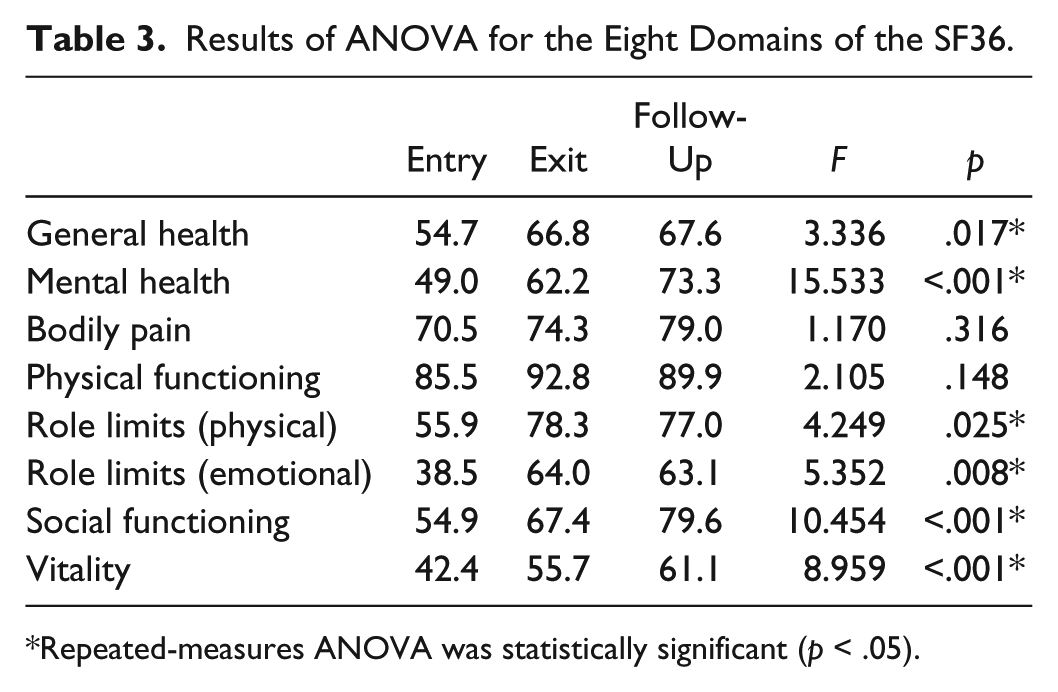
Repeated-measures ANOVA was statistically significant (p < .05).
K-10
Analysis revealed a significant difference (p < .05) between average K-10 scores at Entry and Exit, with lower scores at Exit (22) compared with Entry (27; indicating a lower level of distress), see Figure 3. There was no significant difference found for K-10 scores between Exit (22) and Follow-Up (19).

Mean Kessler–10 scores at Entry, Exit, and Follow-Up.
Discussion
Consistent with previous research, this study demonstrated that on completion of the MERIT Program, participants reported improvements across a number of health and well-being domains, as well as reduced levels of dependence on illicit drug use, compared with what was reported at entry into the program. In addition, our results supported the hypothesis that improvements gained throughout treatment would be evident 3 months following program completion.
Drug Use and Dependence
Participants reported significantly lower levels of psychological dependence on their principal drug of concern at completion of the MERIT Program, and levels of dependence on principal drug of concern continued to reduce in the months following completion of the MERIT Program.
A standard diagnostic cutoff using the SDS does not exist. Some researchers have found that a score of 3 or more indicates the presence of a DSM-IV diagnosis of substance dependence (Kaye & Darke, 2002; Lawrinson, Copeland, Gerber & Gilmour, 2007), whereas others have suggested a score of 4 or more (González-Sáiz et al., 2009., Martin, Chung, Kirisci, & Langenbucher, 2006). In our study, 19 participants scored 2 or less at follow-up, suggesting that almost 50% of participants no longer met diagnostic criteria for substance dependence.
The average number of times a drug was used in the month prior to each interview decreased between Entry and Exit for all illicit substances; this difference was found to be significant for cannabis use.
Other Clinical Outcomes
Psychometric indicators taken at both Entry and Exit reflected significant improvements in participants’ general health, mental health, physical role limits, emotional role limits, social functioning, and vitality over the course of the program. For mental health and social functioning, significant improvements were also found between Exit and Follow-Up, indicating that the benefits gained in these areas continued to rise after completing MERIT. All other health domains were not significantly different between Exit and Follow-Up, indicating that the improvements gained during the MERIT Program were maintained following program completion.
The only health domains that were not found to significantly improve were physical functioning and bodily pain. It is worth noting that scores on these two domains were relatively high at Entry, with higher scores reflecting higher physical functioning and lower levels of pain.
Levels of psychological distress were also shown to be significantly lower at Exit compared with Entry, and lower at Follow-Up compared with Exit (although the latter difference was not significant), again indicating that the positive effects on psychological well-being gained during treatment were not lost in the 3 to 6 months following program completion.
Limitations and Suggestions for Future Research
There are several limitations of this study that should be taken into account, including reliance on participants’ self-report, the absence of a comparison or control group, the small sample size of 40 participants, and potential for non-response bias.
Self-Report
Outcomes in this study were based on self-report measures. Therefore, the information obtained may have been unreliable due to inaccurate recollection and/or social desirability bias. Social desirability bias occurs when people are motivated to over-report or under-report a particular behavior to create a positive impression on others and can be measured through questionnaires such as the Balanced Inventory of Desirable Responding (BIDR; Paulhus, 1991). It could be beneficial for future follow-up studies to measure social desirability bias through the addition of another questionnaire such as the Impression Management subscale of the BIDR, which has been widely used in the scientific community (Stober, Dette, & Musch, 2002). However, having to administer an extra questionnaire would be more time-consuming for both researchers and participants, and may actually lower the response rate as participants are less likely to agree to answer a longer survey.
Despite the limitation of self-report, it is worth noting that during the treatment phase, participants’ reported substance use was consistent with random urinalysis. As participants had demonstrated reliable self-report of drug use while on the MERIT Program, this suggests that their self-report was likely to have been reliable at follow-up as well. During the MERIT Program, participants’ answers could influence their MERIT completion status, the content of their MERIT court report, and possibly, their sentencing outcome for pending court matters; there were no such consequences at follow-up.
Lack of Comparison or Control Group
As there was no comparison or control group in this follow-up study, it is not possible to evaluate how MERIT participants may have differed from non-participants, or to assume that non-participants did not also show similar improvements after having their court matters finalized. Even if it could be established that improved clinical outcomes and lower levels of drug dependence were only evident in those who completed MERIT, the issue of selection bias cannot be ignored. The MERIT Program is a voluntary program and defendants who are accepted into the program and complete it must be motivated to reduce or abstain from illicit drug use; therefore, it could be argued that changes in drug use, dependence, and health were due to participants’ motivation to address drug use and make changes in their lives rather than simply being a result of treatment itself. Ideally, in future research, participants in the MERIT Program would be compared with non-participants in a randomized controlled trial to eliminate selection bias; however, the addition of a control group was beyond the scope of the present study.
Unable to Generalize Due to Small Sample
There were 40 participants in this study, mostly male, all of whom were residing in the Northern Sydney area. Results cannot necessarily be generalized to other populations, including females, older adults, people from various ethnic and cultural backgrounds, and those living in other areas. It would be useful to conduct further follow-up studies involving a higher number of participants and to investigate outcomes for people who have been treated by other MERIT teams based in different locations.
Response Rate and Non-Response Bias
Another limitation of this study was that approximately half of potential participants (32 out of 72, equating to 44.4%) were lost at follow-up. In an ideal situation, missing data resulting from non-responders would be missing completely at random (Johnson, Cho, Campbell, & Holbrook, 2006). However, low response rates create the problem of non-response bias that occurs when there are important differences between participants and non-participants that are relevant to a study (Delgado-Rodriguez & Llorca, 2004). The higher the percentage of non-respondents, the greater the potential for bias, and this makes it difficult to determine whether a sample is actually representative of the population of interest (Barclay, Todd, Finlay, Grande, & Wyatt, 2002).
In this study, participants who were successfully followed-up may have been more stable and healthy than those who were either not contactable or no longer willing to participate in the follow-up study. Attrition at follow-up was largely due to phones not being answered or no longer belonging to previous participants (84.4%), and it is possible that reluctance to answer the phone or changing one’s phone number within a relatively short time period of 3 to 6 months could indicate a lack of stability or lower social functioning. However, a small proportion of potential participants stated that they were unable to complete the follow-up questionnaires due to work commitments; this suggests that they were functioning at a more optimal level than those who were not in full-time employment. One could also argue that some of the non-respondents who did not answer their phone were also engaged in work duties at the times they were called (typically between 9:30 a.m. and 4:30 p.m.).
Conclusions and Future Directions
Overall, the findings of this follow-up evaluation suggest that people who complete the MERIT Program experience a number of benefits over the 3-month period during which they participate in the program, including lower levels of dependence on illicit substances, better state of health and well-being, as well as lower levels of psychological distress. Furthermore, these self-reported improvements were shown to be maintained 3 to 6 months following completion of the program. For mental health and social functioning, improvements were found to actually increase significantly in the period from Exit to Follow-Up 3 to 6 months later. Severity of dependence on participants’ main drug of concern was also shown to further reduce significantly 3 to 6 months after program completion.
Court defendants who report problematic illicit drug use often have considerable treatment needs; yet there are challenges involved for legal representatives and probation and parole officers when attempting to refer defendants to appropriate treatment services (Passey et al., 2007). This study extends on research by Passey et al. (2007) by investigating the subjective health outcomes, drug use, and severity of drug dependence in MERIT participants, and by demonstrating that reductions in drug dependence and improvements in health on completion of the MERIT program can, for some participants, be maintained after 3 to 6 months following program completion. This study therefore adds to our understanding of the value of early referral into treatment programs such as MERIT for defendants who are dependent on illicit substances and highlights the potential for these programs to have long-lasting positive effects beyond the period of time that it takes participants to complete them.
Future research could expand on these preliminary findings; for example, studies could be conducted on MERIT participants from other locations across NSW, and efforts could be made to increase response rates and to perhaps add a comparison group or control group to eliminate selection bias. Other longitudinal studies could analyze clinical outcomes and drug use/dependence after longer periods between MERIT Program completion and Follow-Up than the 3 to 6 month time frame used in the present study.
Given the growing evidence that the MERIT program can effect longer term change on health and criminal justice outcomes, strategies to engage more people in the program could be explored—such as relaxing eligibility criteria and ensuring services are adequately funded to meet demand.
Footnotes
Authors’ Contribution
All four researchers were significantly involved in the design, collection of data, analysis, and writing of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.