
Abstract
Migrant women are under-represented as users of alcohol and other drug (AOD) services. This study examined AOD use by newly arrived women, identifying issues of concern to them. A questionnaire-based survey was conducted with 268 migrant women who had arrived in Perth, Western Australia, within the previous 5 years. Almost half were humanitarian entrants. Most women (76%) reported they did not drink alcohol. Of those who did, 10 were drinking at harmful levels and over half reported changes to their drinking patterns since arrival. One fifth of participants (20%) described distressing incidents related to alcohol or drug use by others. Migrant women are concerned by alcoholand drug-related problems, even if they do not drink themselves. Domestic violence and abuse by strangers were concerns that were aggravated by alcohol and drug use. As new migrants often lack strategies to prevent, or deal with alcohol-related misuse, provision of additional information and support is recommended.
Introduction
In recent years, Western Australia has experienced significant population growth, with overseas migrants accounting for over half of the state’s net migration in the 5 years to 2010, the highest in Australia, and approximately 5% of these arrived on humanitarian visas (refugees). In the Perth metropolitan area, almost 29% of residents migrated from another country between 2006 and 2011 (Australian Government, 2012). One non-government agency in Western Australia that works with migrant and refugee women is Women’s Health and Family Services (WHFS). WHFS provides medical services, counseling, information, community talks and workshops, advocacy, referral, and outreach to women from over 80 different ethnic groups. WHFS also has a women’s Alcohol and other Drug (AOD) service to meet the needs of women who are using AOD, as well as providing services to support their families. Although migrant and refugee women access a wide range of WHFS programs, at the time of this study few culturally and linguistically diverse (CALD) women attended the AOD service. To explore the reasons for this, a needs assessment was undertaken to better understand the barriers that prevented women from accessing AOD services and to explore the types of services and programs desired by newly arrived women, the findings of which are reported elsewhere (Lee, Sulaiman-Hill, & Thompson, 2013). This article reports on information collected as part of the larger study regarding women’s own AOD use and issues related to the impact of AOD use by others on these women. This information was used by WHFS to help design better services for CALD women experiencing AOD issues.
Background
AOD use, for both men and women, are influenced by a number of environmental factors. These can include physical access, socio-demographic characteristics such as occupation, family-related factors, peer group and cultural norms, motivation, attitudes and expectations for drug use, as well as physical health, and the impact of life events such as traumatic experiences (Jonas, Dobson, & Brown, 2000; Marsh, Towers, & O’Toole, 2012). However, a number of gender differences have been reported particularly with respect to mental health issues associated with problematic alcohol use. Women who use alcohol hazardously are more likely to experience depression and anxiety compared with men, while alcohol-related suicide attempts and fatalities are also more prevalent among women (Dale & Marsh, 2000; Marsh et al., 2012).
In addition, because of the health consequences of maternal drug use, stigmatization of pregnant women as a result of any type of drug use may occur. Even for women who are not pregnant, their role as mothers and caregivers can mean that women who drink or use drugs experience more shame, guilt, and stigma than men. The barriers of stigma, depression, and fear of removal of children in a woman’s care, can result in their reluctance to seek help; consequently women enter treatment programs at half the rate that men do (Dale & Marsh, 2000; National Centre for Education Training on Addiction [NCETA] Consortium, 2004).
Historically, AOD service delivery in Western countries was largely developed on the basis of research with Caucasian males (Sterk, 1999; Whiteside-Mansell, Crone, & Conners, 1999). As the original model of service delivery has often been applied with little specific research, consultation, or adaptation to reflect the particular needs of other populations, services are not necessarily entirely appropriate for women and/or other ethnic populations (Sterk, 1999; Whiteside-Mansell et al., 1999).
Women, Drug Use, and the Influence of Culture
Although statistics (Australian Institute of Health and Welfare, 2012) show that migrant and refugee women are under-represented among users of AOD treatment services (Macfarlane Burnet Centre for Medical Research & North Richmond Community Health Centre, 2000), this is not necessarily an indication that the use of AOD among this group of women should be of less concern (De Jong, Valentine, & Kennedy, 1998; Straussner, 2001). Low rates of access to AOD services by CALD women may have more to do with language difficulties, lack of awareness of services, stigma attached to drug use, and cultural issues regarding discussing private issues with “outsiders,” than with lack of need (Macfarlane Burnet Centre for Medical Research & North Richmond Community Health Centre, 2000; Ng, Bartu, & Sang, 1999; Working Women’s Health & Women’s Health in the North, 2000). Research conducted with such groups needs to take into consideration the heterogeneity of cultural groups and the interaction of a range of personal and group factors, which can impact on personal and family AOD consumption patterns (Ames & Rebhun, 1996). Although there has been Australian research on migrant and refugee groups and their issues and concerns regarding alcohol use (Macfarlane Burnet Centre for Medical Research & North Richmond Community Health Centre, 2000; Ng et al., 1999; Working Women’s Health & Women’s Health in the North, 2000), this area of research remains underexplored. Similarly, research on gender differences with relation to AOD use are uncommon, especially in Australia, and specific studies reporting on issues for CALD women are rare (Working Women’s Health & Women’s Health in the North, 2000).
Existing studies illustrate a complex interaction of gender, culture, and attitudes toward drug use (Chen et al., 2000; Reid, Crofts, & Beyer, 2001; Rissel, McLellan, Bauman, & Tang, 2001; Sargent, Maher, Higgs, & Crofts, 2001). Some interactions are protective, especially for women, with strong ethno-cultural, parental, and religious proscriptions against the use of illegal and even legal drugs such as alcohol, in some cases. However, with acculturation, women’s drug use patterns more closely approximate mainstream patterns of consumption (Ames & Rebhun, 1996), but the impact of acculturation on drug use is rarely measured in AOD studies with participants from CALD backgrounds as there is considerable debate as to what constitutes a valid measure of acculturation (Alegria, 2009; Thomson & Hoffman-Goetz, 2009a, 2009b). Individual users, their families, and the community groups to which they belong may demonstrate a wide range of reactions to women’s drug use. Such responses can include shame, loss of face, denial, stigma, embarrassment, and even a perceived loss of honor (Bradby & Williams, 2006; Roarty & Saggers, 2009) and these may place drug users at even greater risk by introducing significant cultural barriers around accessing services.
Method
Other projects involving consumer participation with ethnic communities have found a reference group useful as a forum for discussion, debate, decision making, and action (Karantzas-Savva & Kirwan, 2004). Therefore, as part of this study, a Consumer Reference Group was established to guide the project and to help better understand the barriers to service access (Lee, Thompson, & Amorin-Woods, 2009). Women were invited to participate based upon their capability and interest, rather than as an appointed representative of an association or an ethnic group, with the focus being on gaining consumer perspectives from a wide range of women. The group consisted of women from multicultural backgrounds who were interested in AOD issues as well as general women’s health concerns and they volunteered their time to meet regularly with staff facilitators. The purpose of the group was to assist WHFS examine the appropriateness of WHFS AOD services for CALD women, and plan education and prevention programs for migrant and refugee women and their families around smoking, alcohol, medication, and other drug issues.
The consumer reference group provided background information about the communities under study, as well as providing a forum to facilitate discussion of issues arising during the study and for validation of key research findings. Interviews with service providers from government and non-governmental agencies who worked extensively with newly arrived migrant and refugee women, as well as a number of focus group meetings and interviews with migrant women helped to guide development of the survey protocol and questionnaire format.
For the quantitative survey, 268 migrant and refugee women were recruited between October and December 2006. Women aged 18 years or older, who had arrived in Perth within the previous 5 years, were invited to participate. A purposive snowball sampling technique was adopted to recruit participants, using multiple starting points to limit bias. The heterogeneity in snowball samples can be improved by choosing a broad range of snowball initiation points and limiting each chain to a small number of links (Atkinson & Flint, 2001; Bloch, 2007; Sulaiman-Hill & Thompson, 2011), so respondents were recruited through English classes, community organizations, workplaces, community-based clubs, and groups run through WHFS.
The survey was administered using face-to-face interviews, and women with limited English language skills were interviewed using bilingual workers or through interpreters. Six participants chose to self-administer the survey to complete it. The questionnaire was not translated from English, as more than 40 different language groups were represented among the women interviewed and translation costs would have been prohibitive. Extensive piloting of the questionnaire ensured that the wording used in the questionnaire was understood by a broad range of women from a variety of cultural and educational backgrounds, either in English or with the help of an interpreter or bilingual worker.
In addition to a range of demographic variables, questions were included which focused on smoking, alcohol consumption, alcohol-related verbal and physical abuse, access to medical and social services, herbal and prescription medication, and illegal drugs. There was a filter question regarding alcohol so women who drank less than one standard drink of alcohol in a month did not answer the alcohol-related questions. Risk of harm from drinking was ascertained by asking participants who did drink, “Since coming to Australia, on average how often do you have an alcoholic drink of any kind?” Response choices were as follows: every day, 5 to 6 days a week, 3 to 4 days a week, 1 to 2 days a week, less often, and no answer. These questions were based on those used in the National Drug Household Survey (The Australian Institute of Health and Welfare, 2005), to allow comparison with Australian population data. Consumption patterns were then explored by asking “On a day that you have an alcoholic drink, how many standard drinks do you usually have?” Participants could refer to a pictorial guide as to what a standard drink looked like to assist them in answering the question based on the Australian Alcohol Guidelines current at the time (National Health and Medical Research Council, 2001).
Questions related to barriers to accessing services, the type of information women would like and the types of services and programs they would find helpful were also included based on previous focus group feedback. Although the majority of survey questions were in multiple choice or short answer format, one section used index cards with pictures to depict the types of services and information that women were interested in. Women were asked to select and rank their topics of most importance (Bauer, 1995), a process they described as “voting” for the various options, a technique that proved to be an effective and enjoyable method of communicating ideas to women from a wide range of cultural and socio-economic backgrounds.
Analysis of quantitative survey data was performed using SPSS statistical software. Descriptive and frequency distributions were calculated for each variable, with cross-tabulations (χ2) providing a summary of relationships between categorical variables.
The project received ethics approval from the Human Research Ethics Committee at Curtin University.
Results
The age, time in Australia and visa categories of the 268 women survey respondents is described in Table 1. Women were born in 50 different countries and spoke 48 different primary languages. Just under half (43%) were humanitarian arrivals (refugees).
Demographics of Questionnaire Respondents. a

Numbers do not equal 268 questionnaire respondents, missing data excluded.
The majority (76.1%; n = 201) of women reported that they had not drunk more than one standard drink of alcohol per month during the previous 12 months. Following further questions, three women described alcohol use other than that reported in the original filter question based on a standard drink diagram, “In the last 12 months have you drunk more than one standard drink of alcohol in any one month?” (Yes, [choices provided], No, or Refused). In total, 65 women reported drinking some alcohol.
Harmful Drinking Patterns
Three women were assessed as drinking at risky levels for short-term harm (5-6 standard drinks on 1-2 days a week), and one woman was at high risk for short-term harm (7-10 standard drinks on 3-4 days per week) based on the Australian Alcohol Guidelines current at the time (National Health and Medical Research Council, 2001).
Seven women were drinking at levels consistent with risk for long-term harm. Five women reported drinking 3 to 4 standard drinks 3 to 4 days a week, one woman was drinking 3 to 4 standard drinks every day, and one woman drank 7 to 10 standard drinks 3 to 4 days each week. Five of these women reported drinking more alcohol since coming to Australia. Six requested information and support for depression, and five wanted information and support around family violence.
Changes in Drinking Habits
For those who drank alcohol, changes in alcohol use were also explored. Women were asked to compare their current drinking habits with their drinking habits in their home country. Participants were asked, “Compared to when you drank alcohol in your own country, since coming to Australia are you drinking: about the same amount of alcohol, drinking less alcohol, drinking more alcohol or refused.” Participants were asked about possible reasons for any changes in their drinking patterns. Of those drinking alcohol, 38.3% (n = 23) reported drinking about the same amount, 28.3% (n = 17) reported drinking less, and 31.7% (n = 19) described increased alcohol consumption. Reasons for drinking more alcohol included alcohol being cheaper than back home, socializing with Australians who drank alcohol, and as a way of coping with stress. Health concerns, wishing to be a good role model for their children and having fewer occasions to socialize since arrival were reasons given for drinking less.
Alcohol Use by Others
All women were asked if,
Since coming to Australia, has anyone who has been drinking alcohol or taking drugs ever: Verbally abused you (insulted you, yelled or sworn at you); Physically abused you (hit you, pushed you); Put you in fear (made you scared); Made you feel uncomfortable; or Made you have sex when you didn’t want to?
Her relationship to that person was also assessed. These results are described in Table 2.
Alcohol-Related Incidents by Strangers, Current or Ex-Partners, and Others. a
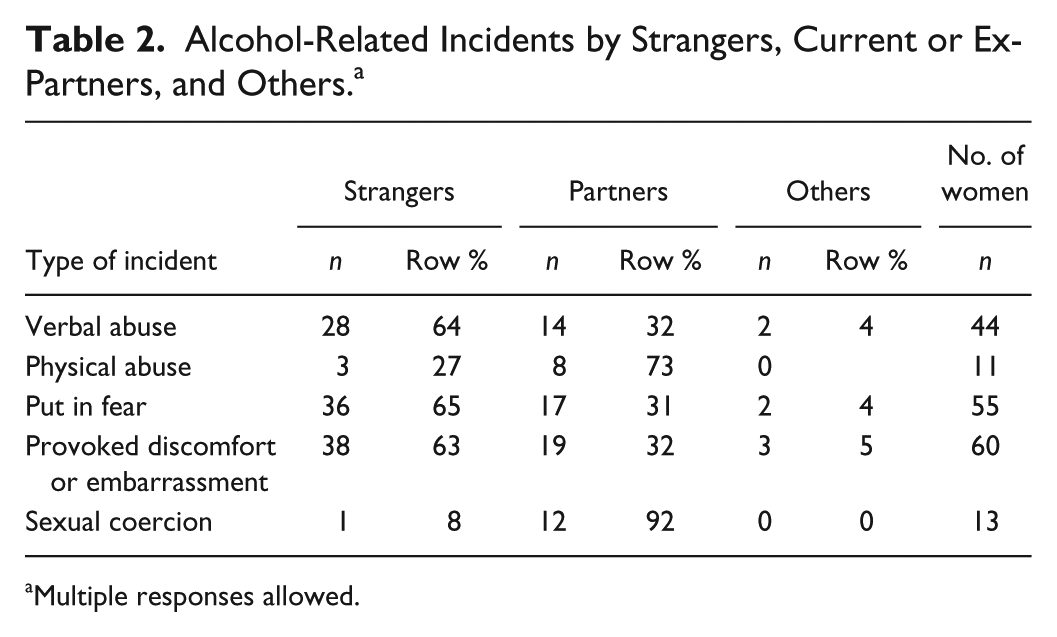
Multiple responses allowed.
Survey data were then compared with findings from the most recent National Drug Strategy Household Survey at the time (Australian Institute of Health and Welfare, 2005). Although the phrasing of some questions was slightly different, making direct comparison difficult, some general observations were noted. CALD women surveyed in this project were significantly less likely to report verbal abuse than women in the National Drug Survey, but were significantly more likely to have felt fearful. In the study group, there was no significant difference between refugee and non-refugee new arrivals regarding verbal abuse experienced by strangers; however, migrant women were more likely to experience being put in fear by a stranger than refugee women (χ2 = 5.444, df = 1, p = .020). Migrant women were also more likely to have felt uncomfortable or embarrassed by someone who had been drinking alcohol or taking drugs (χ2 = 9.99, df = 2, p = .007) and more likely to report having been made to have sex when they didn’t want to by someone who had been drinking alcohol or taking drugs (χ2 = 5.850, df = 2, p = .054). Strangers accounted for the overwhelming majority of cases where women were verbally abused, fearful, or embarrassed, while partners were more likely to be the people who physically abused them.
Incidents by a Stranger
The 46 women who had experienced one or more incidents by a stranger of verbal abuse, physical abuse, being put in fear or forced to have sex when they didn’t want to, were from 19 different countries. They had a range of English language abilities, religious affiliations and migration visa categories. Women in their twenties and thirties were significantly more likely to have experienced these incidents by strangers (χ2 = 12.478; df = 4; p = .014).
Participants were asked if they had been drinking and/or taking drugs at the time of any of these incidents. Of the 80 women who answered the question, 15 women (18.8%) reported that they had been drinking alcohol when the incident took place.
Incidents by a Partner
Current or ex-intimate partners also accounted for a substantial number of incidents, with 20 women reporting concerns in this area. These women were aged 21 to 48 years, were from 13 different countries with varying English language abilities and religious beliefs. More women entering Australia under spousal or fiancé visas experienced these incidents (n = 9) but there was no significant difference between the different migration categories. Eight women (42.1%) reported drinking alcohol before the incident(s) took place.
Family Drinking Concerns
As one of the larger study aims was to explore topics of concern to migrant women, all 268 survey participants were asked to rank their priority issues and concerns. Responses included requests for information on illegal drugs, and for families affected by family violence and alcohol abuse. These results are presented in Table 3.
Alcohol and Other Drug-Related Information Requests.
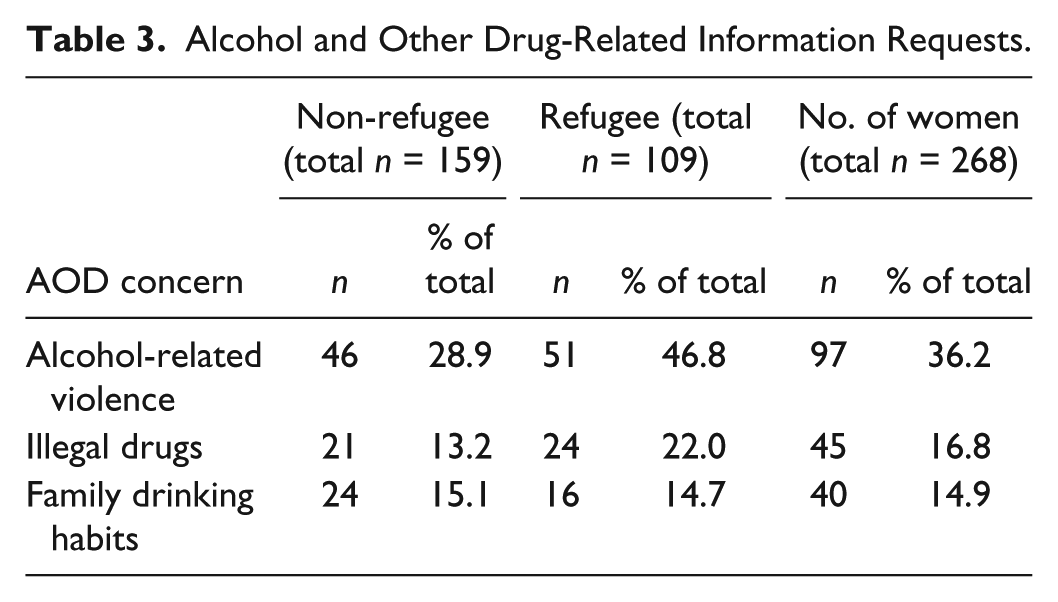
Of 40 women (14.9%) who requested support for family members drinking too much alcohol in their top five choices, six ranked this as their first or second priority. Among participants, there were indications of intimate partner violence—verbal abuse by their current partner (mentioned by 5), physical abuse by their partner (3), put in fear by their partner (5), and being forced to have sex when they didn’t want to (5), for whom two reported this as being by a former partner).
Seven women, from a range of demographic backgrounds, reported concerns or arguments with family or friends about a family member or friend’s alcohol and drug use. Two of the women who wanted support for a family member were drinking at levels considered risky or at high risk for long-term health consequences themselves.
Discussion
The majority of women in our survey (76%) did not drink alcohol. Other studies of migrant alcohol use have also reported abstinence or low drinking levels among women compared with the mainstream population and subsequent generations (Ames & Rebhun, 1996; Bradby & Williams, 2006; Caetano, 1994; Gilbert, 1991).
However, our findings do suggest that some newly arrived women may be acculturating to Australian alcohol use patterns much more quickly than previously anticipated as a result of prevailing host society attitudes. New arrivals to any country come with their own traditions and values about alcohol. Some beliefs and customs will be similar to those of the host country, while others will be quite different and necessitate ongoing negotiation of the host country’s drinking culture (Allan, Clifford, Ball, Alston, & Meister, 2012). The adoption of behavior patterns, attitudes, beliefs, and customs of the host population by newcomers has been theorized to take place over decades, or even generations (Caetano, 1994; Gilbert, 1991). Even though the drinking habits of the group remained the same or even decreased in some cases, one third of participants reported drinking more and this was primarily due to social interaction with Australians, availability of alcohol, and related acculturative pressures as highlighted elsewhere (Arfken, Arnetz, Fakhouri, Ventimiglia, & Jamil, 2011; Szaflarski, Cubbins, & Ying, 2011). However, unlike some countries, drinking is seen as a positive or even essential social practice and an integral component of Australian culture (Allan et al., 2012) and there is considerable pressure for non-drinkers to conform. Several non-drinking women in the study encountered pressure to drink, or drink more, due to these expectations. The interaction between acculturation and drinking patterns could be explored in future studies. Four women in the survey did report drinking more alcohol as a way of coping with stress. Although an increase in alcohol use has been linked to stressful conditions (Szaflarski et al., 2011) and trauma (Arfken et al., 2011), in many situations this may be underreported or not publicly acknowledged. Although population data and risk group behaviors are known in some cases, relatively little information has been reported on new arrivals and this is another area for future study.
Although for the majority of participants, their current drinking levels posed no short- or long-term risk to health, a small number of women were drinking at harmful levels. While an increase in alcohol consumption and problematic use by a few does not imply a serious problem for the group overall, as the total alcohol consumption of a given population increases, the risk for a concurrent increase in problematic drinking will also increase (Ames & Rebhun, 1996). Cultural and religious beliefs may offer some protection against alcohol problems, but these factors do not provide total protection against problematic alcohol use, as risk factors such as poverty, discrimination, targeted alcohol advertising, and alcohol availability may prove more powerful than such protective beliefs (Ames & Rebhun, 1996). High drinking frequency has been associated with high host culture competence and social interaction in other studies (Amundsen, 2012), so as new arrivals acculturate the risk of alcohol-related issues is likely to increase over time. All new CALD arrivals should therefore be provided with appropriate information regarding alcohol consumption and how to access information or services if needed. Forty women (14.9%) requested support and information for family members drinking too much alcohol as a priority topic. Although a minority, the findings suggest these women may have found it difficult to access services or get the information and support they require.
Alcohol-Related Violence
The results of the survey confirmed the views of service providers and newly arrived women in the development phase of the research that alcohol use by partners often played a role in domestic violence, even though it was not the direct cause of the violence (Lee, 2008). This also concurs with previous reports (Leonard, 2001). Around 20% of questionnaire respondents reported incidents of either verbal abuse or being put in fear by a family member drinking alcohol or taking drugs since their arrival in Australia. Although incidents of physical abuse (4.3%) and sexual assault (5.2%) were less common, members of the project’s Consumer Reference Group felt that there may have been a tendency to underreport such incidents, based on their own experiences and anecdotal reports within their communities. While the questionnaire gave examples of verbal abuse (being insulted, yelled, or sworn at) and physical abuse (being hit or pushed), cultural and individual differences in what is regarded as abuse could potentially account for some discrepancies (Allimant & Ostapiej-Piatkowski, 2011). The impact of social desirability bias certainly needs to be considered when discussing sensitive issues such as domestic violence. Although the majority of surveys were completed by interview, six respondents asked to self-complete the survey form. During this process, several of these women disclosed information about family violence and alcohol abuse by a partner, details that may have been less forthcoming if discussed during interview.
Issues related to AOD use by others impacting on the safety of ethnic women in public places are not often reported in the literature, although two Australian projects with CALD women in Victoria (Working Women’s Health & Women’s Health in the North, 2000) and the Vietnamese community in Perth (Ng et al., 1999) have reported findings consistent with the present study. Just under half of our study participants reported one or more abusive incidents by a stranger, often citing traumatic events that may well have been reported to the police by other people had they experienced the same abuse. Refugee women did not experience more abuse, sexual assault, or fear than other migrants, or in comparison with women in the National Drug survey (Australian Institute of Health and Welfare, 2005), although refugees have been identified as a vulnerable subgroup for alcohol misuse (Arfken et al., 2011). Given their often traumatic histories and because they may lack strategies to deal with such incidents in the early period after settlement, they are potentially at higher risk for re-traumatization, posttraumatic stress disorder (PTSD), and other mental health problems (Sowey, 2005; Sulaiman-Hill & Thompson, 2012). Although it is possible that insults and abuse may sometimes go unheeded due to language barriers, it is also likely that the problem may be underreported due to a lack of trust in authorities or unfamiliarity of the system in Australia. Women described incidents that impacted on their confidence and feelings of safety and they appeared to lack strategies to deal with these either at the time or afterward. Sometimes this is due to uncertainty regarding what they should do or where to seek assistance, revealing a need to discuss prevention strategies and provide all new arrivals with the tools and knowledge to deal with such incidents.
Limitations
The sample size of this study is relatively small (268 migrant and refugee women) in comparison with population surveys but these often fail to adequately identify and provide facilities for collecting and reporting data for CALD women who may have challenges with the English language. Notwithstanding, the study provides evidence that alcohol-related problems among newly arrived women may be of greater concern than the literature suggests. More research in this area is needed.
Although it was assumed that limiting the research to women who had been in Australia 5 years or less would reduce the effects of acculturation, an acculturation scale could have clarified whether reported changes in behavior were due to women acculturating faster than previously assumed, or to other factors.
Another limitation of the study was that the questionnaires were not translated but instead administered by bilingual/bicultural workers or by the principle researcher with the assistance of an interpreter. It is possible that measurement errors may have occurred during the data collection and may have affected the findings, although supervision and debriefing of interviewers occurred frequently during data collection. While in a perfect research environment validated translations would have been used, this was impractical for logistical and financial reasons. Moreover, at the time of the research there was a lack of accredited translators and interpreters for some of the languages spoken by participants. The processes, advantages, and disadvantages of using bilingual workers, interpreters, and translated instruments in this study will be explored in detail elsewhere (article currently under review).
Some notable differences were also observed between self-reported and interviewer data, revealing the impact of social desirability factors. It is likely that some sensitive material around family violence and physical abuse may have been withheld from interviewers due to embarrassment or shame. Measurement limitations such as recall bias of pre-migration drinking patterns combined with the transitional nature of the migration process also need to be considered. In addition, although participants had the opportunity to have the questionnaire administered using an interpreter or bilingual worker, the questionnaire format was in English. It is possible that inconsistencies in interpretation, especially for women with little or no understanding of English, could have impacted on some results. Using a validated, translated instrument could have overcome some of these issues.
At the time of the study, WHFS was only funded for women clients, so the focus of the research was AOD issues specifically relating to women. The questionnaire did not expressly investigate the drinking habits of partners or children of the women respondents, or how these had changed since coming to Australia and this would be an important focus for future research.
Conclusion
Although cultural and religious imperatives underpin the drinking habits of many migrant women resulting in low levels of alcohol use or abstinence, this study has highlighted the vicarious impact of alcohol use by others on newly arrived women in Australia, an issue not well documented in the literature. Concerns related to alcohol and drug use by others include domestic violence and verbal and physical abuse by strangers, which impact on CALD women’s feelings of safety in public places. Many migrant women lack strategies to prevent or deal with the consequences of family or stranger alcohol misuse, so health and settlement service providers are encouraged to provide new arrivals with appropriate information and support.
Footnotes
Authors’ Note
The project was a joint endeavor between Women’s Health and Family Services and Curtin University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Susan Lee received support of an Australian Postgraduate Award administered through Curtin University, the Office Multicultural of Interests to assist with costs associated with focus groups, interviews and the survey; the West Australian Network of Alcohol and Other Drug Agencies to pay for interpreters used during the project; and Women’s Health and Family Services for time to undertake and report on this research. Dr. Sandra Thompson and Dr. Sulaiman-Hill received support for their time from the Combined Universities Centre for Rural Health at the University of Western Australia.