
Abstract
This article examines the association between drug use severity and mortality in primary care patients with substance use disorders. In 848 individuals with known vital status, severity was low in 32%, intermediate in 38%, or substantial/severe in 30%. Two-year survival was 93% in the low group, 96% in the medium group, and 92% in the high group (p = .19). The age-adjusted risk of death for the high-severity group was twice that of the medium-risk group (hazard ratio = 2.00, 95% confidence interval = [1.02, 3.93]). Individuals in the high group were more likely to die from accidents than those in the low- or medium-severity groups (50% vs. 20%, p = .021). Compared with low- and medium-severity groups, age at death was 5 years younger in the high-severity group (52 ± 9 vs. 57 ± 6, p = .017). Premature death due to accidental causes in persons with substance use disorders is a persistent yet complex problem.
Persons with psychiatric illness, including substance use disorders, die prematurely and are likely to succumb from injuries or medical causes related to the disorders (Colton & Manderscheid, 2006; Dembling, Chen, & Vachon, 1999; Druss, Zhao, Von Esenwen, Morrato, & Marcus, 2011; Maynard, Cox, Hall, Krupski, & Stark, 2004). Whether these premature deaths are preventable is a critical question. With respect to substance use disorders, the risk of premature death varies by many possible factors, including type of drug, severity of use, trajectory of drug use, co-occurring psychiatric illness, and other personal characteristics, including age, gender, race socioeconomic status, health status, or health behaviors, including tobacco and alcohol use (Bargagli et al., 2006; Kertesz et al., 2012; Smyth, Fan, & Hser, 2006). Some of these factors are not modifiable (e.g., age), or are very difficult to modify (e.g., socioeconomic status), whereas others such as drug use severity are potentially modifiable. The purpose of this article is to examine the association between drug use severity and mortality as well as cause of death in primary care patients with substance use disorders. The motivation for conducting this analysis stems from the idea that if there were an association, then intervening to reduce severity could result in lower rates of premature death.
Method
Patient Population
Between April 2009 and September 2012, 868 individuals were enrolled in a randomized clinical trial designed to examine the effects of a one-time brief intervention for problem drug use (Roy-Byrne et al., 2014). All individuals agreed to be assessed at baseline, and at 3, 6, 9, and 12 months. While some of these individuals had alcohol use disorders, the focus of the study was on problem drug use and not problem alcohol use. There were 848 (98%) individuals who gave consent for researchers to search administrative data, including arrest records, hospital discharge abstracts, chemical dependency treatment records, and Washington State death records. These individuals received medical care in seven primary care clinics affiliated with a public safety net hospital in King County, Washington. Key inclusion and exclusion criteria are listed in Table 1. Individuals enrolled in formal chemical dependency treatment programs, as well as those with high risk of imminent suicide, life-threatening medical illness, severe cognitive impairment, or active psychosis, were excluded. This study included 848 individuals with known vital status.
Study Inclusion and Exclusion Criteria for Eligibility for the Randomized Trial.

Study Variables
For this study, there was extensive information on patient characteristics including sociodemographic variables as well as assessments of drug and alcohol use in the year prior to and after study enrollment (Roy-Byrne et al., 2014). Drug use in the month prior to enrollment was assessed with the Addiction Severity Index (ASI; Cacciola, Alterman, McLellan, Lin, & Lynch, 2007). The major independent variable, the Drug Abuse Screening Test (DAST-10), was used to define problem drug severity as low (score = 1-2), intermediate (score = 3-5), or substantial/severe (score ≥ 6; Yudko, Lozhkina, & Fouts, 2007). The DAST-10 was administered only at baseline, whereas the ASI was administered at regular follow-up assessment times.
The primary dependent variable in this study was vital status determined primarily from Washington State death records provided by the Washington State Department of Health. These records are electronic versions of death certificates and include the underlying cause of death. Washington State death records from 2009 through June 2014 were available and were linked to study participants using name, date of birth, gender, and social security number if available. Death reporting for the first 6 months of 2014 was provisional and not yet complete. Other sources of vital status included obituaries, the Social Security Death Master File, and primary care clinics where patients received health care. Survival time was calculated as the number of days from enrollment to death or June 30, 2014, for survivors. Cause of death, available only from death certificates, was categorized according to International Classification of Diseases, Version 10 codes and was classified as (a) diseases of the heart; (b) malignant neoplasms; (c) external, including accidents and suicide; (d) chronic liver disease and cirrhosis; (e) infectious; and (f) other (Maynard & Boyko, 2006).
Statistical Method
The chi-square statistic was used to assess the association between categorical variables and DAST-10 score category, and the one way analysis of variance was used for continuous variables such as age. Survival curves were constructed according to the Kaplan–Meier method. The log rank statistic was used to determine whether unadjusted survival differed among the three DAST-10 score categories. To further examine whether DAST-10 score category was associated with vital status, we ran several Cox regression analyses. First, the unadjusted association between DAST-10 score category and survival was determined; second, given that survival decreases with increasing age, the age-adjusted association was examined; and third, forward stepwise selection was used to identify statistically significant predictors of outcome, and after all statistically significant predictors entered the model, DAST-10 score category was forced into the model. Finally, chi-square analysis was used to examine the relation between DAST-10 category score and cause of death.
Results
For the 848 participants, the DAST-10 score category was low severity in 272 patients (32%), medium in 323 (38%), and high in 253 (30%). Table 2 shows the association between baseline characteristics and DAST-10 score category. p values refer to overall association between the variable of interest and the DAST-10 score category. Age decreased with increasing severity of the drug problem, whereas gender was not associated with DAST-10 score category. Overall, there was a statistically significant association between race and DAST-10 score category (p = .005). There were 311 Black patients and 80 (26%) were in the low DAST-10 score category, whereas there were 537 individuals who were not Black and 209 (39%) were in the low category. In general, individuals in the high-severity group had socially less stable situations in that they were less likely to be married or living with a partner, had lower levels of education, and were more likely to be disabled and unable to work. Significantly, 50% of the high-severity group was homeless for at least one night in the past 3 months.
Baseline Characteristics and Drug Use Severity.

Note. DAST-10 = Drug Abuse Screening Test; ASI = Addiction Severity Index.
Not surprisingly, the high-severity group had a higher ASI drug use composite score as seen in Table 2. The high-severity group was less likely to use marijuana, but was more likely to use stimulants, opiates, sedatives, or two or more drugs. Intravenous drug use was very low in the low- and medium-severity groups, yet was much higher in the high-severity group. Overall, the majority of participants used alcohol and tobacco, although the high-severity group was most likely to use either alcohol or nicotine. In the high-severity group, 200 (79%) used nicotine in the past 30 days. While the ASI medical status composite score was similar across the three groups, a higher proportion of the high-severity group had psychiatric illness, defined as ASI psychiatric status composite score > 0.38. Notably, a higher percent of the high-severity group had a goal of total abstinence from drugs.
There were 57 deaths, and 55 appeared in Washington State Death Records. Average follow-up was 3.6 ± 1.1 years. As seen in Figure 1, overall 2-year survival was 94% and was 93% in the low DAST-10 score category, 96% in the medium group, and 92% in the high group (p = .19, by log rank statistic). Cox regression was used to further investigate the association between drug use severity and survival. Because survival was highest in the medium group, it was selected as the reference category. As seen in Table 3, the unadjusted association between DAST-10 score category was not statistically significant. In comparison with the medium-severity group, the hazard ratios were higher for the low- and high-severity groups, but the differences were not statistically different. After adjusting for age alone, the risk of death for the high-severity group was twice that of the medium risk group; this difference was statistically significant as the lower bound of the 95% confidence interval was 1.02. In the third model, age and intravenous drug use were the only two variables selected from candidate variables in Table 2. After adjustment for these two factors, the hazard of death for both low- and high-severity groups compared with the medium-severity group was higher but not statistically different as indicated by the wide confidence intervals.
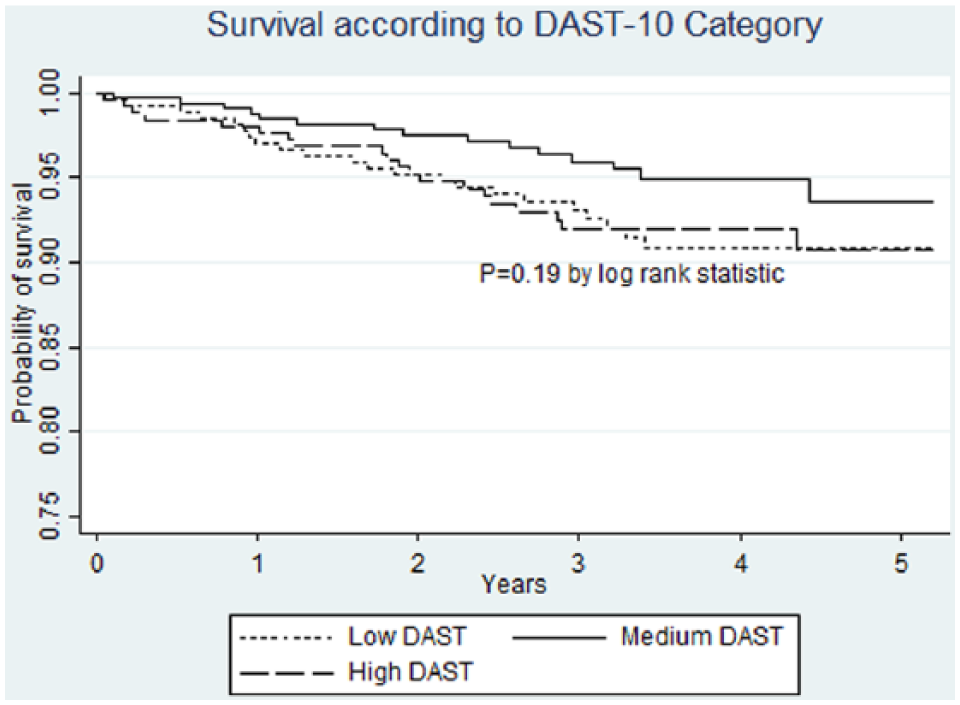
Survival according to DAST-10 category.
Hazard Ratios and 95% Confidence Intervals for Cox Regression Models (n = 832).

Note. DAST-10 = Drug Abuse Screening Test.
Underlying causes for the 55 deaths that appeared in Washington State death records are shown in Table 4. Overall, there was no association between cause of death and DAST-10 score category: χ2(10) = 9.86, p = .45. However, the percent of external causes of death was higher in the high-severity group than it was in the low- and medium-severity groups: 50% versus 20%, χ2(1) = 5.36, p = .021.
Cause of Death and Drug Use Severity.

Note. DAST-10 = Drug Abuse Screening Test.
Overall, there were four (two in the low group and one each in the medium and high groups) deaths due to lung cancer and another four (one each in the low- and medium-severity groups and two in the high group) due to human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS). Three individuals who succumbed to lung cancer were current smokers, and two who died of HIV/AIDS were intravenous drug users. There were an additional seven individuals who died of chronic liver disease related to alcohol use, three of whom were in the low-severity group. The age at death was 52 ± 9 years in the high-severity group and was higher in the low- (58 ± 6 years) and medium-severity (57 ± 6 years) groups. Compared with the low- and medium-severity groups, the 5-year difference in age at death for the high-severity group was statistically significant, t(53) = 2.96, p = .017.
Discussion
In this group of individuals who had substance use disorders and received primary care in clinics affiliated with a public safety net hospital, high-severity problem drug use was associated with worse survival, accidental death, and earlier age at death. The estimated death rate in this group of 848 individuals was 18.7 deaths per 1,000 per year compared with the U.S. age-adjusted death rate of 7.4 deaths per 1,000 per year in 2011 (Hoyert & Xu, 2012). While death rates were high for all individuals in the study, compared with those with medium severity, individuals with high severity had twice the risk of death after adjusting for age. The association between severity and mortality was not linear, in that those with medium severity had better survival than those with low severity. This is a little puzzling as the low-severity group had less disability and psychiatric illness, although they were slightly older and more often never married. Individuals in the high-severity group were 2 to 3 years younger than those with low- or medium-severity problem drug use, yet their average age at death was 5 to 6 years younger than their counterparts in the other two groups.
Also notable were differences in the underlying cause of death as reported on death certificates; individuals in the high-severity group had a higher proportion of accidental causes such as drug overdoses than did individuals in the other two groups. Individuals in the low- or medium-severity groups had a higher percent of deaths due to cancer or cardiovascular diseases, yet also died of conditions related to substance use disorders, including alcohol use disorders.
While these findings were not particularly unexpected, they tell a tragic story of premature death and potentially avoidable deaths due to accidents among individuals with problem drug use (Colton & Manderscheid, 2006; Dembling et al., 1999; Maynard & Boyko, 2006; Ries et al., 2015). Participants in the trial used a variety of drugs including marijuana, prescription opiates, methadone, heroin, and stimulants as well as alcohol and nicotine. In addition, a high proportion had accompanying psychiatric illness. Nationally, there are 23 million Americans who have substance use disorders, yet only 10% access treatment (Substance Abuse and Mental Health Services Administration, 2013). The stigma associated with drug addiction and alcohol addiction to a lesser extent is a major barrier to treatment of what has been called the leading cause of preventable death in the United States (Kelly, Wakeman, & Saitz, 2015).
It is beyond the scope of this study to determine whether some deaths were preventable. Although the results were striking, they are based on only 55 deaths that were reported in Washington State death records. There are the usual concerns about the validity of the underlying cause of death as stated on the death certificate as well as the difficulty of distinguishing deaths due to accidents from those that were intentional. Another limitation has to do with the measure of alcohol consumption; individuals reported the number of days per month they consumed alcohol and did not report how much they drank at a given time. Consequently, it was not possible to assess the relative contributions of drug and alcohol use to survival.
Limitations regarding the completeness of death records and accuracy of the underlying cause of death do not call into question the finding that drug use severity was associated with decreased survival and more accidental deaths. Despite being younger than their counterparts with low or medium severity, persons with high severity died at younger ages. These findings have been previously reported and are unlikely to improve without changes in the way addiction is viewed by providers, health care organizations, legislative bodies, and the larger society (Kelly et al., 2015).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was funded by National Institute on Drug Abuse Grant R01DA026014.