
Abstract
Little research has described determinants and consequences of patient–provider rapport among people who inject drugs (PWIDs). This mixed-method study (a) qualitatively described facilitators, barriers, and consequences to rapport development between PWIDs and their health care providers and (b) quantitatively tested the hypothesis that quality of rapport is associated with positive patterns of service use. Two exploratory focus groups with PWIDs and care providers were conducted. Subsequently, 89 PWIDs completed a survey interview; of those, eight completed a follow-up qualitative interview. Qualitative results indicated that rapport is influenced by drug-related behaviors, addiction severity, provider expertise, patient-centered care, and perceived discrimination and that rapport then influences patient compliance, timing of care, and criminal activity. Quantitative results indicated that rapport predicted PWID satisfaction with care as well as frequency and timing of emergency department presentations. Results suggest that PWID–provider rapport has several unique determinants and is associated with positive health care outcomes.
Keywords
People who inject drugs (PWIDs) are socially marginalized and suffer a disproportionate burden of illness relative to nonusers (Cherubin & Sapira, 1993; De Alba, Samet, & Saitz, 2004; Fischer et al., 2005; Frischer, Goldberg, Rahman, & Berney, 1997; Single, Robson, Rehm, Xie, & Xi, 1999). Despite this, PWIDs delay seeking health care and underuse primary care services (Chan et al., 2004; Chitwood, McBride, French, & Comerford, 1999; De Alba et al., 2004; Fischer et al., 2005; French, McGeary, Chitwood, & McCoy, 2000; McGarry, Stein, Clarke, & Friedmann, 2002). PWIDs can experience further disadvantage due to poor rapport with health care providers (HCPs). System-level barriers to rapport include unrealistic staff expectations, confidentiality concerns, and wait times (Drumm et al., 2003; VanderWaal et al., 2001). The attitudes, knowledge, and experiences of HCPs are additional challenges (Breitbart, Kaim, & Rosenfeld, 1999; Carroll, 1995; Clarke, 1993; Ding et al., 2005). Quality of health care encounters themselves are influenced by the presence or absence of empathy, listening, shaming, discrimination, flexibility, and disclosure (Drumm et al., 2003; Merrill, Rhodes, Deyo, Marlatt, & Bradley, 2002; Regen, Murphy, & Murphy, 2002; Weiss, McCoy, Kluger, & Finkelstein, 2004).
Rapport development is integral to any clinical interaction, and may be a particularly important element of health care with marginalized PWIDs. A patient-centered approach improves satisfaction with care and adherence to medical recommendations, and fulfills patient expectations better than physical exams or prescriptions (Bass et al., 1986; Beck, Daughtridge, & Sloane, 2002; Cegala, 1997; Jackson & Kroenke, 2001; Little et al., 2001; Nutting, Goodwin, Flocke, Zyzanski, & Stange, 2003; Pelzang, 2010; Rao, Weinberger, & Kroenke, 2000; Stewart, 1984). But how is a patient-centered approach fostered in the context of health services? Self-Determination Theory (SDT) provides a useful perspective with which to understand how rapport might facilitate motivation for seeking health services. In particular, this theory addresses how social events are perceived and how those perceptions affect motivational processes (Wild & Enzle, 2002). SDT characterizes motivation to engage in activities on a continuum, ranging from activities that are completely initiated and controlled by external social forces, to activities that are fully self-determined. On this theory, all people have fundamental psychological needs for autonomy, relatedness, and competence. Social contexts that support these elements of self-determination promote interested engagement in activities and personal growth. Conversely, when social contexts promote perceptions of being controlled or coerced, intrinsic motivation (i.e., interest and engagement in activities) is undermined (Deci & Ryan, 2002). SDT suggests that rapport with patients will be maximized when HCPs support their patients’ needs for autonomy, competence, and relatedness. However, this theory has not been applied in many marginalized or cross-cultural settings, nor has it been investigated in the context of injection drug use. Consequently, the objectives of the present study were to (a) describe factors that facilitate or prevent the development of rapport between PWIDs and their HCPs; (b) describe how HCP–patient rapport relates to PWIDs’ experiences of health care and subsequent care-seeking behavior; and (c) test the hypothesis that quality of PWID rapport with a primary HCP would be associated with positive patterns of health care use.
Method
Overview
This project was facilitated by an academic–community partnership between the University of Alberta and Edmonton, Canada’s Streetworks harm reduction program (Wild et al., 2003; Wozniak, Prakash, Taylor, & Wild, 2007). Community-Based Participatory Research (CBPR) principles (Macaulay et al., 2009) guided the development, implementation, interpretation, and dissemination of the research. Streetworks and its clients provided regular input into the project to ensure it remained relevant and acceptable to the community. All PWID data collection sessions took place in private meeting rooms located within community-based agencies and separate from health care encounters. The research was also approved by the University of Alberta Health Research Ethics Board.
Three data sources were used: (a) PWID and HCP focus group interviews provided an initial exploration of how PWID–HCP rapport is developed and how rapport influences health care; (b) cross-sectional structured interviews quantitatively described associations between PWID–HCP rapport and administrative health records; and (c) semi-structured qualitative interviews with a subset of the quantitative sample further clarified rapport-related themes and quantitative associations documented in the other data sources.
Although the development of rapport in a long-term PWID–HCP relationship was of interest, we anticipated that many participants would be unattached to a regular HCP and may access a variety of health services and providers differently than the general population. Thus, rather than limit our enquiry to a specific health care setting or discipline, PWIDs were instead encouraged to discuss care-seeking patterns and rapport development, drawing on their personal experience with multiple settings and HCPs. Where setting- or discipline-specific content emerged this was taken into account during the analysis.
Eligible PWIDs were 18 years or older, English speakers, injecting drugs within 30 days preceding data collection, and not participating in treatment within the past month, Edmonton residents, and not intoxicated or experiencing a psychiatric emergency. PWID participants received CDN$20 as compensation per session for their time.
Focus Groups
Eight PWIDs, purposively selected because of their extensive experience with the health care system, took part in a preliminary focus group session intended to identify key concepts for further exploration during individual interviews. To provide a complementary perspective, seven HCPs with experience caring for PWIDs participated in a separate focus group session. One researcher moderated each session using a semi-structured interview protocol, while another recorded field notes and assisted in clarifying responses. Both moderators were experienced in group interview settings, extensively reviewed and practiced the interview guides prior to the sessions, looked for consensus and explored any perceived disagreement within the group, and used participant engagement strategies where required. Questions and probes explored participant expectations of and experiences with health care, as well as perceived influences on patient–HCP rapport.
Structured Quantitative Interviews
Due to the difficulty in reaching the PWID population with traditional sampling means, a non-probability sampling approach known as chain-referral sampling was used. This method involves identification and recruitment of a small number of participants via word of mouth, who then provide contact information for other potential participants (Erickson, 1979). To minimize bias from specific social networks and settings within the PWID community, multiple chains were used for recruitment. A total of 89 participants completed the quantitative data collection.
Baseline demographic variables obtained during the structured interview included (a) age, (b) gender, (c) ethnicity, (d) education, (e) marital status, (f) parental status, (g) legal status, (h) housing stability, (i) income, and (j) employment status. Drug use data were collected on (a) ease of access to drugs, (b) duration of use, (c) cessation attempts, (d) income source for drug acquisition, (e) drug-related expenses, (f) substances used, (g) overdose risk, (h) experience of withdrawal, and (i) the Blood-Borne Virus Transmission Risk Assessment Questionnaire (BBV-TRAQ; Fry & Lintzeris, 2003), a 34-item standardized measure of injecting, sexual, and skin penetration practices that exhibits good reliability and validity (Cronbach’s α = .87, test–retest correlation = .84 in Fry & Lintzeris’ sample). Variables specific to health and health care were also collected, including (a) drug dependence treatment history, (b) self-reported physical health status, (c) self-reported mental health status, (d) ability to identify a regular physician, (e) regular physician knowledge of drug use, (f) self-reported number of visits to regular and other physicians, (g) preferred point of health care access, (h) satisfaction with care, (i) perceived hepatitis C (HCV) risk, and (j) perceived HIV risk.
The Health Care Climate Questionnaire (HCCQ) measured PWID–HCP rapport. Derived from SDT, the short form of the HCCQ is a validated six-item questionnaire assessing perceived autonomy support by physicians (Deci, Eghrari, Patrick, & Leone, 1994; University of Rochester Psychology Departments, 2006; Williams, Gagne, Ryan, & Deci, 2002) including items such as “I feel that my doctor has provided me choices and options” and “My doctor listens to how I would like to do things.” Internal consistency for the six-item scale was excellent (α = .93).
Alberta Health Care Unique Identifiers (UIs) were collected from consenting participants to link study data to health service use data. Research assistants noted that almost all participants consented in principle; however, not all participants were able to supply their UI to study staff within the allotted time period (1 month post-questionnaire). Among the participants who provided their UI (n = 42), service use was assessed in the year immediately preceding data collection, and included number of emergency department (ED) visits, ED visit date and time, and mode of transportation to ED. Frequent ED visits, late night care-seeking (night shift presentation to services), and transportation via ambulance (EMS) were measured to assess delayed care-seeking and lower continuity with a single-care provider (Brown & Goel, 1994).
Follow-Up Interviews
To clarify and confirm the focus group and quantitative findings, eight PWIDs were purposively recruited from the quantitative sample for a follow-up interview. Eligible participants exhibited divergent scores on the quantitative measure of rapport (HCCQ), satisfaction with care, identification of a regular physician, and ED use to ensure a comprehensive exploration of the patient experience. Participants provided narratives on their health care experiences, and were probed on issues brought up in earlier data collection sessions such as the locations of care, the difference between health professions, negotiation strategies, the central role of drugs, the impact of disclosure of drug use on quality of health service encounters, and the relationship between rapport and satisfaction with care. Participant recruitment ended after eight interviews because later interviews confirmed the emerging themes and did not uncover new or alternate themes.
Participant Characteristics
Limited demographics were collected for PWID focus group and qualitative interview respondents. Both qualitative participant groups were similar to the PWID quantitative sample as well as the quantitative subsample and administrative health data were available for both (Tables 1 and 2). PWID participants were predominantly male, single, unemployed, unstably housed, and living in poverty. Approximately half were Caucasian and half had a high school education. Consistent with other local data sources, the majority of participants were poly-substance users as opposed to users of a single drug or drug class. For the HCP focus group, participants were seven nurses, physicians, and a mental health counselor, ranging from 32 to 56 years of age, with 9 to 30 years’ health care experience, and reporting 5 to 100 encounters with PWIDs a week. The participants were predominantly female and community-based; however, hospital-based professionals were also present.
Characteristics of Each Sample.
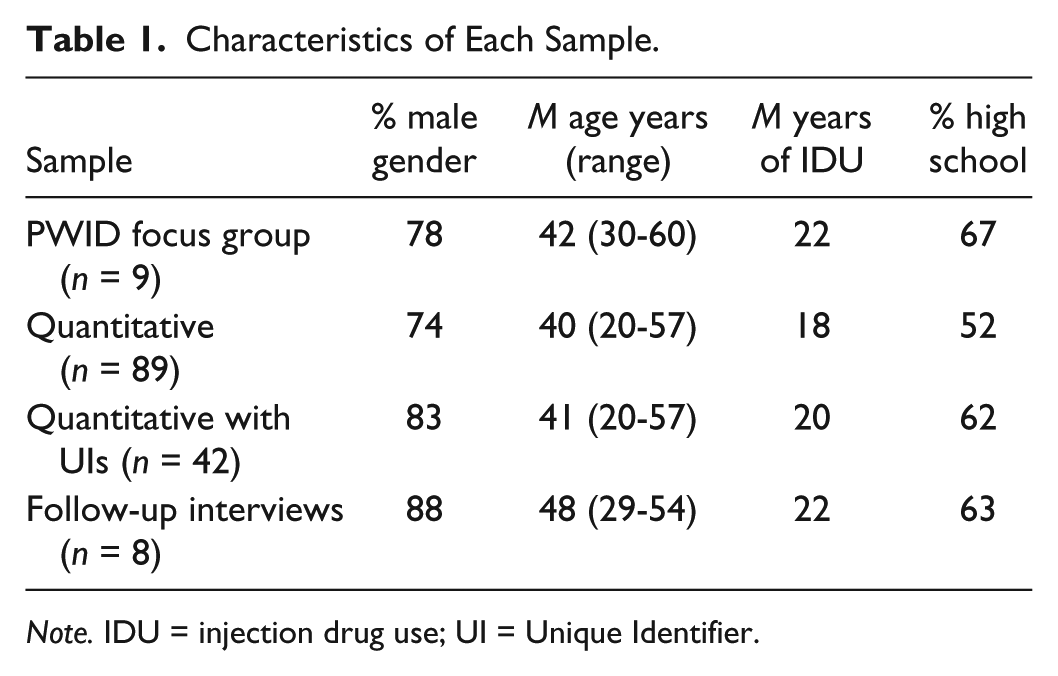
Note. IDU = injection drug use; UI = Unique Identifier.
Socio-demographic Characteristics of Quantitative Sample.

M = mean, SD = standard deviation.
Qualitative Analysis
Focus groups and interviews were audio-recorded, transcribed verbatim, and verified for accuracy. Analyses of these data used a combination of thematic analysis (Boyatzis, 1998) and paraphrasing (Wozniak et al., 2007). Thematic analysis can be applied by researchers from a variety of epistemologies, and thus, facilitate the communication of findings to a wider audience (Boyatzis, 1998). This pragmatic analytic approach (Figure 1) is particularly well suited to CBPR and has been successfully used with this target population in previous research (Wozniak et al., 2007). Initially, within-transcript analyses identified meaning units (i.e., sentences, paragraphs) expressing single and idiosyncratic topics by participants. A descriptive label and verbatim examples were written and defined for each meaning unit. Next, meaning units were compared across focus group members and individual interview transcripts to identify constituents (i.e., meaning units shared by two or more participants; Wild & Kuiken, 1992; Wozniak et al., 2007). This procedure allowed us to identify commonly shared meaning units across the sample, as opposed to idiosyncratic comments. Constituents were compiled and a thematic label and verbatim excerpts were produced. Transcripts and field notes were then reread to ensure that themes and constituents identified during analyses were consistent with the interview content. NVivo analytic software facilitated the organization of meaning units and emerging themes.

Examples of within-transcript and between-transcript analysis.
Trustworthiness of our analysis was assessed in four ways: (a) a second researcher reviewed all data analysis and independently coded two transcripts; (b) focus group participants reviewed thematic labels and constituents and provided feedback; (c) follow-up interview sessions continued, actively seeking alternative interpretations and experiences, until data saturation occurred and no further themes emerged (Kuzel, 1999); and (d) a Streetworks staff member reviewed thematic labels and constituents to ensure consistency with her observations of the local PWID scene.
Quantitative Analysis
Initially, we identified participants with a regular physician to determine a subgroup who had the opportunity to establish rapport with a primary HCP for a longer term. Student t tests and chi-square tests examined associations between the presence/absence of a regular physician and PWID characteristics that may have been influenced by this patient–HCP relationship (current legal involvement, quit attempts, withdrawal episodes, drug acquisition via crime, overdose risk, and infectious disease risk behavior). Next, Pearson correlations were calculated among participants who reported that they had a regular physician to determine associations between rapport (HCCQ scores) and three main service use outcomes chosen to reflect the quality and consistency with which participants experience a therapeutic relationship with their primary HCP: (a) disclosure of drug use (yes or no), (b) ED visits, and (c) satisfaction with care. Additional Pearson correlations were calculated for other available health care measures assessing self-reported health status, consistency of HCP, and acuity of presentation. Finally, hierarchical multiple regression was performed to determine whether rapport incrementally improved prediction of the primary service use variables, adjusting for effects of demographic covariates and PWID risk behaviors.
Results
Focus Groups
Participants’ accounts of the determinants of rapport included patient, HCP, external, and encounter-based factors.
Patient factors
Participants acknowledged that the patient contributed greatly to the development of patient–HCP rapport. For example, respondents stated that the nature of drug dependence and withdrawal is such that it exerts an inescapable influence on the PWID’s behavior during health care encounters. Participants stressed that drug dependence is an illness with potentially severe interpersonal and other consequences, over which drug dependence PWIDs had little control:
I mean it’s like you had a choice at one point but that line’s been crossed a long time ago. I mean, you can have like 50 doctors say no. It doesn’t change the fact that you have to like you have to do what’s required. I mean like you rob a drug store, rob another store or person or something to buy drugs with. And when you look at the severity of your problem and I mean you look at your entire life at something you destroyed, what you’ve lost. (IFG4, 177)
1
PWID health care encounters were often described as fundamentally social, rather than medical, in nature. Participants acknowledged that, given the nature of drug dependence, caring for PWIDs is not a straightforward task.
I mean there’s no question that some of my hardest interactions are with someone where it is mental health and addictions the complexity sometimes can feel overwhelming. And certainly I’m no master of any of it. So I feel at a loss sometimes of what to do, or how to help. (PFG4, 416)
Care avoidance was another barrier to effective rapport for many participants and was usually attributed to past experiences with health care. PWIDs related several past episodes of poor treatment by HCPs. These experiences led patients to delay, refuse, and prematurely terminate health care encounters, compromising the establishment of good rapport with HCPs. In addition, HCPs were keenly aware that typical wait times for those patients dealing with drug withdrawal and street life were unrealistic, and were prepared for crisis presentations as a result:
People can’t wait 3 or 4 hours. Or they’ll come in the morning and by the afternoon, something, things will have completely fallen apart, that sort of thing. It really frustrates me to see people come in—in crisis. (PFG6, 847)
HCP factors
HCP focus group participants emphasized that their pre-encounter attitudes, experience, and position of power had major impacts on the rapport achieved during PWID–HCP encounters. Seasoned HCPs expected patient hostility but accepted that it often had a legitimate, remediable cause:
I think sometimes people just come in feeling judged from the minute they get there and probably with great justification. And they come in and have been judged before and they’re kinda scared to tell you anything or openly hostile when they first come in. (PFG5, 280)
Recognizing their role in establishing healthy relationships, HCP participants exercised self-reflection after their PWID encounters. Participants accepted responsibility for their role in the encounter:
It’s if I don’t have that connection—they don’t come back? Then there was something wrong and I often sort of try to figure out what the heck happened here and what did I do wrong. Because those are the ones that bug me . . . (PFG4, 246)
PWID participants also remarked that HCP knowledge about illnesses associated with street life and drug dependence was a great asset to good patient care:
I think they’re um, better at the clinic too because they are more used to having drug users around and they’re used to seeing the same people and pretty well know how their habits are. (IFG8, 376)
Within-encounter factors
Participants in both focus groups devoted most of their discussion of rapport to the content and quality of the PWID–HCP interaction itself. Discrimination against PWIDs and associated trivialization of PWID concerns was a very common rapport-damaging experience.
I think the doctors there think you’re coming in there for drugs, even if it’s a legitimate reason. Like if you have an abscess or something like that. They’ll let you wait still. “Oh you’re an IV user. You can wait a while, you left it this long, it’s not a big thing” . . . Ya yup you’re the last stick on the totem pole. (IFG1, 383)
In contrast, rapport was strengthened by the basic principles of patient-centered care, such as time, listening, concern, confidentiality, and partnership. HCPs took the time to find common ground with their patients and share control of the encounter where possible:
I guess I expect at times sometimes a little bit of initial resistance but then I expect at the end that we will have a plan that I think will work for both parties. (PFG2, 65)
Developing trust and honesty in a PWID–HCP relationship is both complex and gradual. PWIDs acknowledged that honesty can strengthen rapport, but it can also have drawbacks:
I mean my problem is I have lie to a psychiatrist. Like thing is every single thing wrong with me to them is from drug use. I mean like every hallucination, every illness in my body is simply because you’re an IV drug user this and that. So I have to sit there and kiss ass and lie to them and if I am having trouble I can’t tell them that. (IFG4, 332)
HCPs understood that it takes time to develop this open relationship, and focused their early rapport-building efforts on remaining authentic, available, and attuned to their patients’ context. They were comfortable accepting as much honesty as was possible for the PWID:
I expect as much honesty as they are capable of giving in the context. So that I can help them . . . My other expectation when dealing with IV users, [is] of myself. I expect myself to be as open and as approachable as I can be. So expectations of openness on both parts I guess . . . (PFG6, 99)
HCPs used several culturally sensitive strategies to build this relationship, from humor to harm reduction counseling to asking patients about their context:
One of my tricks is if someone says something that I don’t understand, I’ll say, “Hang on, what’s that, what does that mean?” And that’s a very powerful way of creating a rapport. (PFG6, 333)
In all health care encounters, a negotiation process between the patient and the HCP occurs, and this negotiation has an impact on rapport and subsequent care-seeking behavior. Where the recipient of care is a PWID, the nature of the negotiation has additional unique characteristics. PWIDs focused on the need to navigate HCP-centric rules and create a legitimate argument for their health care requests:
My father-in-law had passed away, I wanted to go to the funeral you know my kids wanted me there and that. And I couldn’t get a carry. I couldn’t go to the funeral . . . There’s a lot of bull of having to get your pills every day. I’ve been getting them every day for the last year now. And it just I find like if I could get it even like every twice a week. Once a week. I would be a lot better off. I could take off for a few days. Go out of town, I could go up [north], see my kids. The way it is now, I have to be at the pharmacy. (IFG2, 599)
Given the challenges associated with drug-related PWID–HCP negotiation, consistency in a HCP’s application of rules was reassuring to participants:
The clinic, the best thing about the clinic is the consistency. I mean, even though sometimes you might not like the answer you get, I mean, the staff treats you. It’s like, basically equals respect type thing. Like as long as you’re like honest and like, fair with the staff, they’re helpful. (IFG4, 389)
Conversely, inconsistent HCP practices are frustrating to patients:
The bad thing is when one doctor. It’s almost if one doctor writes five of your friend’s prescription and you go to see the same doctor and he basically shoots you down cold. (IFG4, 764)
HCP participants described the emotion-laden nature of PWID encounters as well as their strategies for dealing with these emotions. Strong reactions to a patient can interfere with one’s ability to help that patient. When participants explained their actions and remained calm, their patients usually responded in the same way:
I know it sounds a bit odd but you tell yourself that you’re comfortable and you’re casual and that actually you see people, the other person calms down. That’s speaking slowly and softly. Great trick for calming down in a situation like that ‘cause people are often not necessarily hostile but still agitated, worried, you know. (PFG6, 338)
External factors
Participants in both groups alluded to certain system-level rapport builders and breakers. HCPs were frustrated in their attempts to comprehensively address drug dependence and social issues by the system’s time, space, and resource constraints:
Because it’s not designed to help people who are marginalized. The system isn’t set up to take care of these people while they’re in hospital and deal with the big picture. I’m sure she wasn’t getting enough pain medicine or enough drugs in hospital and she just said, “Screw you guys, I feel better, I’ve got other needs” and we’re not addressing those other needs. When we have them there, when we have the opportunity to do it. Not that we can fix everything but I think we have to at least make sure those things are addressed so they don’t feel like they have no other options but to leave. (PFG2, 654)
PWIDs mirrored this frustration with the health care system, citing bureaucratic barriers and wait times with inadequate communication to help cope with these barriers: It’s just until you put these little hoops and stuff and on top of it you are usually the 50th person to be seen. And you go into emergency and there will be 200 people in the waiting room and its daytime already and you’ve watched the whole waiting room empty twice. And they bring you in and they don’t even do anything. (IFG4, 696)
Other health care team members also influenced rapport; a negative encounter with one team member can damage the rapport built by others:
Well, we’ll have people though that everything will being going well, everything’s great, they’re being admitted and all this stuff. And then all of a sudden the next thing you see them slamming at the door and they’re angry. And they go through so many people, the nurses, the doctors, right down to the porters and one person they will have a really negative interaction with somebody where they feel judged. (PFG5, 794)
Quantitative Associations Between Rapport and Service Use
Comparisons between PWIDs who reported having access to a regular physician (as opposed to not having such access) indicated that physician accessibility was associated with lower criminal involvement (39% vs. 65%), χ2(1) = 4.61, p < .05; less reliance on criminal activity for drug acquisition (53% vs. 83%), χ2(1) = 6.79, p < .01; more attempts at cessation of drug use (four vs. two injection-free periods, t81 = 2.50, p < .05), and less frequent experience of drug withdrawal (22% vs. 53%), χ2(1) = 6.82, p < .01 (Table 3).
PWID Characteristics by Physician Status.

Note. IDU = injection drug user; BBV-TRAQ = Blood-Borne Virus Transmission Risk Assessment Questionnaire.
Denotes parole, probation, conditional/community sentencing, bail, pending charges, or outstanding warrants or fines.
Defined as the number of periods where injection ceased for 6+ months.
Reported in the previous 6 months.
Defined as 3+ episodes in the previous 6 months where respondents reported fixing beyond their normal limit.
Assessed by the BBV-TRAQ.
p < .05. **p < .01.
In the subgroup of PWIDs reporting regular access to a physician, rapport was associated with satisfaction with health care (r = .58, p < .0001; Table 4); this association remained significant after adjusting for socio-demographic and injection behavior covariates (F = 104.83, p < .001; Table 5). Rapport was also associated with positive secondary outcomes, including decreased night shift presentation (rho = −0.23, p < .05) and decreased EMS transportation to the ED (rho = −0.21, p = .056; Table 6). Although rapport was only marginally associated with disclosure of drug use (50% vs. 27.3%), χ2(1) = 3.06, p < .08, and not with overall ED use, the latter two were associated with each other, that is, nondisclosure of drug use was associated with more ED use (rho = −0.36, p < .05; Table 4).
Intercorrelations a Among Measures of Rapport, Health, and Health Care Use: Self-Report Data and Visits to ED.

Note. ED = emergency department.
Pearson correlation coefficients presented where both variables are continuous; point biserial correlation coefficients presented where one variable is dichotomous.
Measured using Health Care Climate Questionnaire (HCCQ), used in this study as primary rapport measure.
p < .05. ****p < .0001.
Association Between Rapport and Satisfaction With Physician Care, Adjusting for Socio-demographic and IDU-Related Variables.
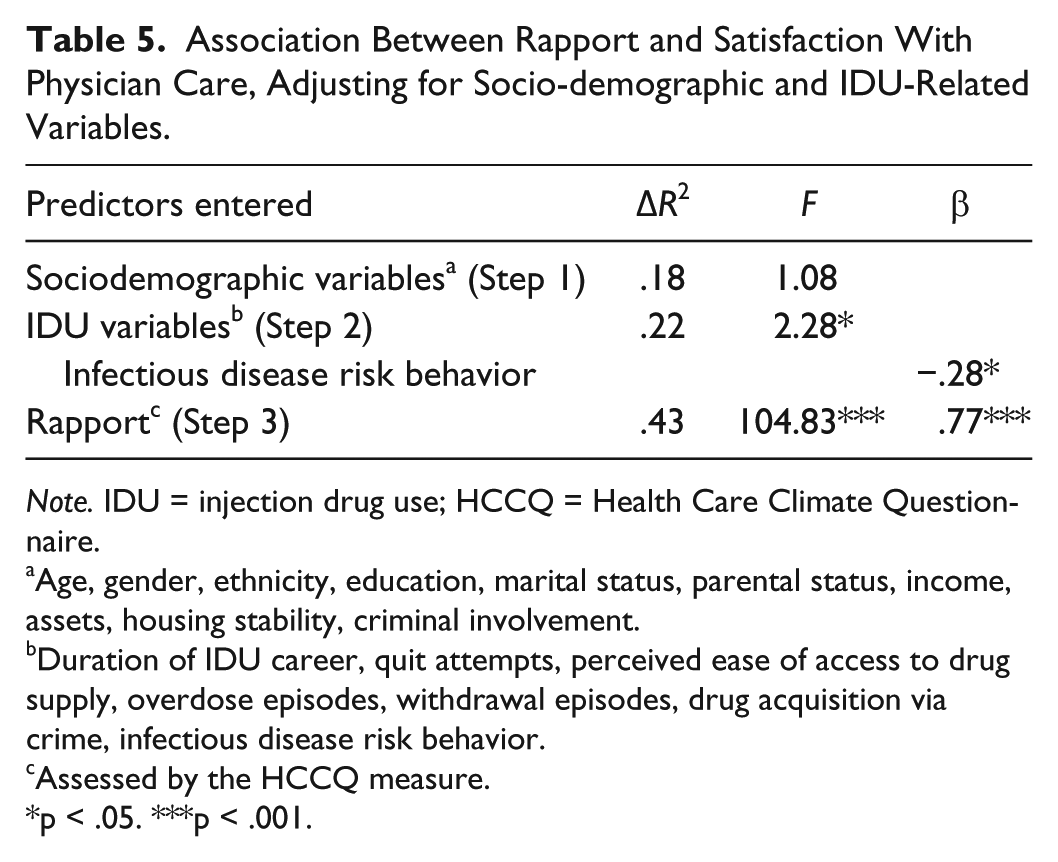
Note. IDU = injection drug use; HCCQ = Health Care Climate Questionnaire.
Age, gender, ethnicity, education, marital status, parental status, income, assets, housing stability, criminal involvement.
Duration of IDU career, quit attempts, perceived ease of access to drug supply, overdose episodes, withdrawal episodes, drug acquisition via crime, infectious disease risk behavior.
Assessed by the HCCQ measure.
p < .05. ***p < .001.
Intercorrelations a Among Measures of Rapport and Health Care Use: ED Encounter Data.
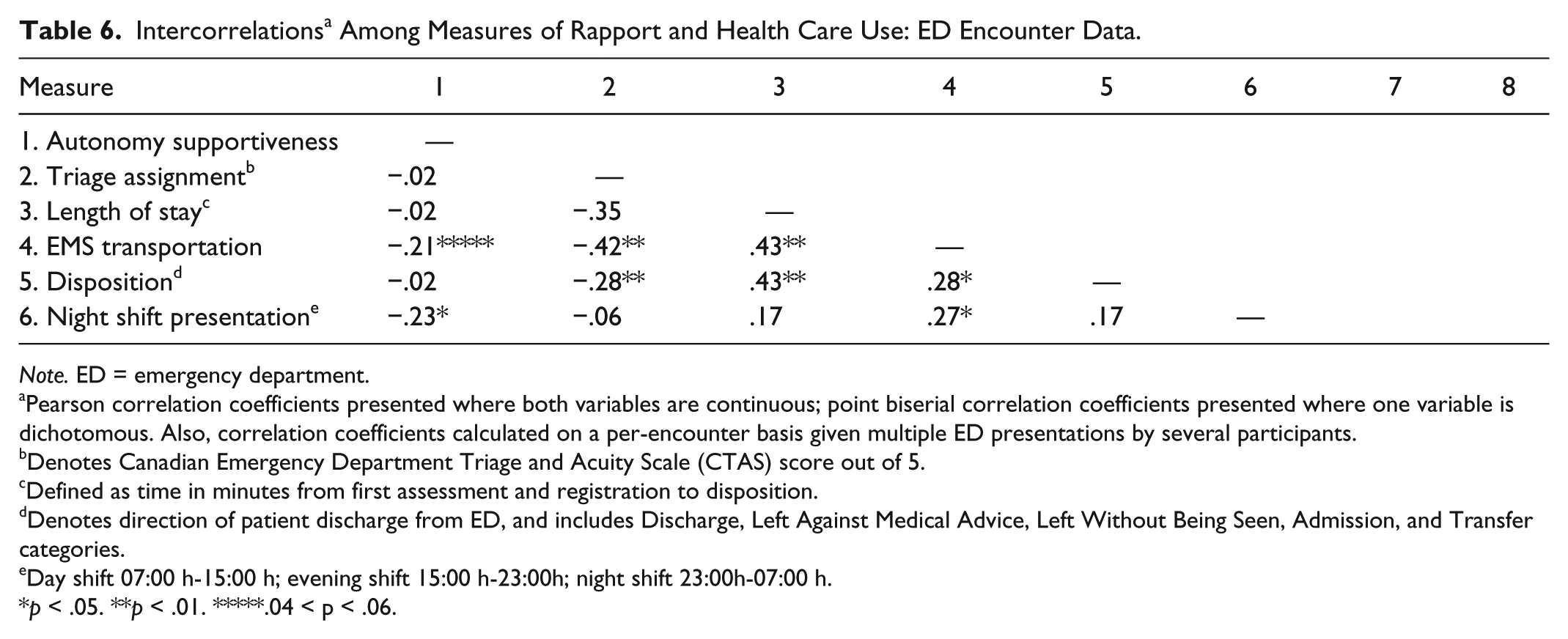
Note. ED = emergency department.
Pearson correlation coefficients presented where both variables are continuous; point biserial correlation coefficients presented where one variable is dichotomous. Also, correlation coefficients calculated on a per-encounter basis given multiple ED presentations by several participants.
Denotes Canadian Emergency Department Triage and Acuity Scale (CTAS) score out of 5.
Defined as time in minutes from first assessment and registration to disposition.
Denotes direction of patient discharge from ED, and includes Discharge, Left Against Medical Advice, Left Without Being Seen, Admission, and Transfer categories.
Day shift 07:00 h-15:00 h; evening shift 15:00 h-23:00h; night shift 23:00h-07:00 h.
p < .05. **p < .01. *****.04 < p < .06.
Follow-Up Qualitative Interviews
Interview participants confirmed many of the themes which surfaced during the earlier focus group sessions about the preexisting patient and HCP factors, the external context, and the encounter-based factors, which contributed to PWID–HCP rapport. Participants stressed the importance of HCPs acknowledging that drug dependence is a complex illness. They also noted that people living with drug dependence tended to behave in ways that shaped the HCP’s expectations:
Well it’s so hard you know ‘cause you, you know, you’re abusive, you’re loud . . . you just walked 30, 40 blocks, three or four different places probably and finally you get to this point and at some point you’re trying to get to see him to help you out you know and so they go you know they interrogate you and you know “You’re double doctoring” you’re this or you’re that. (I3, 343)
Drug dependence not only affects the behavior and overall health of PWIDs, it also changes users’ priorities. Drugs play a central role in active users’ lives, and all other pursuits, including health care, take a back seat until the need for drugs is met.
You don’t got no dope after a while, how you gonna get more dope so you gotta do other things to get more dope. Right? And then you gotta do crime or you go to work or whatever you gotta do right, it’s a habit. (I5, 110)
Focus group themes of HCP familiarity, values, attitudes, experience, and expertise were equally brought up in the individual interviews as being key HCP attributes necessary for rapport. Many participants were grateful when they had HCP continuity. Participants were much more comfortable with a HCP who showed expertise in drug dependence, drug-related injury, pain management, and other conditions commonly experienced by street-involved people.
I’ve shopped around a lot to find the right doctor and finding a doctor who is knowledgeable about the street illnesses, you know, there’s no point in me going to see a doctor who deals with the upper echelon, you know, with their illness because those aren’t the illnesses I get and they understand it, and they see more patients like myself with the same background so they don’t have the bias. (I1, 49)
As for influences at the level of the Canadian health care system, participants confirmed that bureaucracy, legislation, and health care teams exerted an important influence on rapport. Though participants usually wanted to see a doctor as part of their visit, they often interacted with nurses, counselors, reception staff, security, and ambulance personnel first. Physicians function within this team setting and their decisions are under the influence of these team members. Having valid identification to access public health care was not a given. Furthermore, participants felt that HCPs were unconcerned that their patients’ medical conditions were not addressed more expediently:
You set an appointment and you wait and wait for months down the road to go to see the doctor and they lost your paperwork or “I don’t know where it could be, try again next week.” You know? And I just waited 3 weeks or 4 weeks, they don’t care, they don’t understand that, there’s no compassion. (I3, 395)
Regardless of whether participants had a regular HCP or where they accessed health services, most participants alluded to frustrating wait times. The longer the participants waited, the more sick from withdrawal and belligerent they often became, further damaging their opportunity to establish rapport. Participants were upset that the unpleasantness of withdrawal and pain, though not life-threatening, were not treated with the same priority as other medical conditions:
You go into the emergency and you’ve got an OD or you’ve done too much of something you sit and wait there for 4, 5, 6 hours before anybody sees you and you see people that come in after you getting treatment while you’re sitting there and if you raise a ruckus then the security runs you out. (I1, 55)
Similar to our focus group results, individual interviews gravitated overwhelmingly to a discussion of the PWID–HCP interaction itself during health care encounters. Non-discrimination and patient-centered care were confirmed by all participants to be key determinants of effective rapport. The HCP use of humor and harm reduction helped to make communication appropriate to the PWID context:
He started laughing and said “why not?”
[Laughter]
He just jokes around stuff.
Ya?
Ya, he’s pretty good ya. (117)
Participants were more satisfied with visits during which they were treated as equals worthy of the same dignity as HCPs themselves:
I go in to see my family doctor, when he comes through the door he’s got a smile on his face “How you doing [Bob]?” You go in through the emergency, it’s “What’s the problem?” it’s not a person thing it’s an object thing. (I1, 91)
Negotiation tactics
Patient–HCP interaction in the context of injection drug use is unique in that drug dependence plays a central role. Disclosure of drug use has several rapport-related consequences and PWIDs need to decide to what extent they can be honest with HCPs. The need for patients to obtain drug prescriptions often dominates encounters, and without addressing this issue, the opportunity to further develop rapport or explore other health care needs may be lost. It is within this context that HCPs and PWID patients have set up certain rules of negotiation to ensure that their respective expectations are satisfied. First, participants could not perceive a consistent HCP standard for dealing with patient requests. The specific negotiation strategies used by participants to procure a prescription, for example, varied significantly according to the HCP involved. As some participants put it, this system or lack of a system essentially forced patients to “play games” and shop around:
Depending on how much they give you, I mean, or what you need will probably determine who you’re going to go and see. (I6, 483)
At one end of the spectrum, some HCPs were known for their blanket refusal to prescribe narcotics, often accompanied by prominent signage at clinic doors. At the same time, participants described multiple physician practices with a seemingly greater interest in patient volume than individual assessment. Many of these practices were known for their tendency to prescribe narcotics rather easily without first assessing the patient’s actual condition. This perceived lack of interest on the part of the HCP also impeded rapport development. In this unpredictable environment, participants had learned to read each HCP’s behavior and observe their management patterns for other PWIDs, and present their case in a fashion consistent with the HCP’s usual practice.
As a general rule of negotiation, PWIDs were careful to disclose only the minimal information necessary to procure their medication. Disclosure of injection, drug diversion, or other forms of prescription misuse usually led to abrupt discontinuation of existing prescription, and in some cases, termination of the HCP–patient relationship itself. Participants also acknowledged that they needed to be honest enough with their HCP to relate what they needed if they expected to have their needs addressed. Some disclosure was also necessary to garner a HCP’s trust:
If I don’t say what I need I’m not going to get it you know like, but if I [don’t] show them what it is and what I need to get it done to fix it then they really can’t really help me right? (I6, 264)
Participants also described having to deal with numerous HCP-centric rules of negotiation, such as routine questions about drug use patterns, urine drug screens, restricted drug amounts and dispensing frequencies, and limited treatment of chronic pain or issues related to drug dependence (e.g., mental health, infectious diseases). They felt that HCPs abided by such rules, not to maximize patient safety and well-being or comply with professional standards of care, but rather to protect themselves. These stringent rules, combined with the HCP’s powerful position, ultimately left many participants feeling like they had very little autonomy over their health care. Several participants spoke of the desperation and punishment inherent to their position in this power differential, invoking religious, military, and other metaphors:
I honestly feel like a prisoner of war. (I7, 458)
Faced with these rules, participants had developed various counter-tactics to advance their agenda in addition to the selective disclosure patterns described above. Some participants believed that it was too difficult to keep track of a constructed narrative, and preferred to be straightforward with their health care requests and hope for an understanding professional. Other participants felt that it was best to compromise, if necessary, and meet a HCP’s expectations to justify to the HCP that their own requests were also worthy of being met:
I just want to be treated with respect, but to be treated with respect, you’ve got to earn respect.
And how do you earn respect?
Well I think by this time when I go see him and show him my clean arms and I’ll tell him, “Look anywhere you want, you will see no holes.” And I said now you know “I’m doing what you want doc and I’m not only doing it for you I’m doing it for me too.” (278)
Regardless of the specific negotiation strategies used, most participants relied on their street-honed instincts to guide them in their assessment of each health care encounter and its likely outcome. Though verbal and nonverbal language and indirect observations of peer-provider encounters provided important clues, participants also alluded to a less tangible “sense” of whether or not things were going well:
You can tell. Just this or this or for example when they say someone’s a racist you can’t see it but you can tell so it’s the same notion here. You just can tell if they’re a human being, it’s just a certain sense of, you know, a sixth sense of you can tell who’s treating you right or who’s not. (I8, 37)
Outcomes of rapport
The quality of the HCP–PWID relationship leads to varying degrees of trust, patient satisfaction, HCP continuity, criminal activity, and compliance with recommendations. PWIDs may also decide where to access health care or whether to access health care at all based on their interpersonal experiences.
Quantitative associations between PWID–HCP rapport and patient satisfaction with care were confirmed in follow-up interviews, with all participants agreeing that a positive rapport experience made them happier with their encounter. This association appeared to be moderated by the patient’s prescription expectations, but once prescription needs were addressed, rapport was an important determinant of overall satisfaction:
Would you say it’s associated with feeling more satisfied with the visit? More satisfied with your care in general?
Ya, ya, you feel like you’re getting help right from someone that cares about you. (784)
The influence of location was specifically explored in individual interviews because no consensus was reached on its effect during focus groups sessions. It became clear that location is not a key determinant of rapport, but rather an outcome of rapport. Participants felt that it was more the HCPs in a location as opposed to the location itself, which established good or bad rapport. For example, PWIDs shared positive experiences with certain HCPs in locations otherwise perceived as negative:
Well last time I had pneumonia, and I was down for about 2 weeks . . . I stayed there for a night and day, and whatever, and then they [found me a shelter bed] and slept there for 4 or 5 days about, they took care of me, they made sure I was warm and they got rid of my cold, they gave me my medications. (I6, 305)
However, a participant and his peers’ negative experiences with one or more HCPs in a given facility shaped the overall reputation of the facility and influenced their decision as to whether they would go back, if given a choice:
What’s really sad, is the [hospital] has a very bad reputation.
Really?
Extremely bad.
Will you avoid going there even if you’re close?
Oh ya. Yup.
Ok, how come?
Why? Bad experiences. (98)
Some participants believed that HCP unwillingness to negotiate with patients living with drug dependence set the stage for drug-related criminal activity, HCP discontinuity and “doctor shopping.”
I don’t know, just I guess different days different docs right? Like I know a lot of people here that do that too right, they switch doctors, right, all over the city just everywhere, and there’s no really there’s no really favoritism, it’s just the way drug dependence is [Inaudible word] it just makes it go here there and like the . . . (I6, 469)
A HCP’s commitment to rapport development also encouraged some participants to commit to a long-term relationship and comply with a HCP’s recommendations:
I OD’d and I woke up 3 days later in intensive care . . . and one of the social workers there came through and asked the right questions and she got one of the [community health workers] . . . to come to see me ‘cause I was suicidal, I wanted to check out. I’d had enough trying to beat this and . . . she came over 3 days in a row to see me and just she got me off [to treatment], spent 3 years out there, got my head back together, my life back together . . . but that was because I was being treated as an individual. And I felt cared for. (I1, 166)
Discussion
In contrast to the general population, rapport is defined by PWIDs in a distinctly different way, including such elements as disclosure, nondiscrimination, and consistency. In keeping with scholarly work on rapport between HCPs and patients in more general settings, study participants confirmed that rapport involves many of the central tenets of the patient-centered clinical approach, such as HCP–patient communication, partnership, empathy, and continuity. Similarly, rapport is fostered when HCPs adopt autonomy supportive strategies identified in SDT, such as providing information exchange in a non-controlling way, shared decision making, and empathy. Whereas HCP-controlled encounters limit PWIDs’ engagement in their care, shared-control encounters foster such engagement. These findings are consistent with a large body of research using SDT that consistently demonstrates that that autonomy supportive styles facilitate rapport and engagement in social relationships that exhibit power differentials (e.g., between managers and employees or teachers and students; see Deci & Ryan, 2002). In addition to autonomy support, qualitative interview participants also equated rapport with disclosure of drug use to a HCP; this is, perhaps, a PWID-specific manifestation of patient-HCP trust. Nondiscrimination is another key concern; perceived bias against PWIDs damages rapport, whereas the acknowledgment of a PWID’s personhood improves it. Finally, drug dependence holds overwhelming priority for many PWIDs; failure to address drug use in a consistent fashion undermines rapport development.
Although the PWID–HCP literature on rapport identifies many of these influences (Breitbart et al., 1999; Carroll, 1995; Clarke, 1993; Ding et al., 2005; Drumm et al., 2003; Merrill et al., 2002; Regen et al., 2002; VanderWaal et al., 2001; Weiss et al., 2004), our results broaden this literature to provide evidence for the roles of selective disclosure, proof of legitimacy, and other PWID negotiation strategies developed as a response to perceived HCP inconsistencies during health care encounters. These negotiation strategies are used by highly marginalized individuals whose experience with powerlessness is entrenched in health care and social structures and who, ultimately, have no other means to exert some control over their health care encounters. HCPs would do well to be mindful of their position of power relative to PWIDs and encourage greater partnership in decision making. Furthermore, punitive and abstinence-based approaches to drug policy may reinforce this power differential and have the unintended consequence of reducing PWID’s intrinsic motivation to change; pragmatic approaches to policy, such as harm reduction, may afford a greater sense of autonomy for PWIDs and be more effective in engaging people toward better health choices.
PWID–HCP rapport supports positive health experiences, including trust, satisfaction with care, follow-through with HCP recommendations, continuity with one HCP, and timely care-seeking. Conversely, a lack of rapport plays a role in HCP discontinuity and avoidance of care, and criminal activity may also be escalated. Participant responses to specific probes during follow-up interviews suggest that poor rapport is an upstream influence on these negative outcomes. HCPs may want to accordingly adopt a broader view of the health and social impact of rapport for this population, seek out learning opportunities to better understand the PWID context, and incorporate consistent, relationship-based care as an important potential form of harm reduction for their patients who live with drug dependence.
The study findings point to the need for policy development regarding good clinical practice in PWID care. Mandating a clinical practice model in a physician environment that is built on autonomous practice is difficult. Practice change is more likely to be a gradual process, whereby the practice setting is first influenced through translation of the research findings into practice guidelines and other educational activities relevant to the clinical context, then providing incentives for the behavior to evolve into common clinical practice. This along with integration of best practices in the care of vulnerable populations at the level of health professional schools will drive the emergence of patient-centered PWID care as a common practice in the system.
Limitations
The research described here was exploratory in nature. Purposive groups with fewer than 10 participants are common in qualitative research, where the objective is not to generalize findings to larger populations but rather to deepen understanding of observed phenomena in a homogeneous subpopulation (Kuzel, 1999). Though our quantitative sample was small, quantitative findings were intended primarily for data source triangulation with qualitative findings. The use of mixed methods and our results showing that similar findings were obtained across all samples strengthens the likelihood that our observations reflect this population’s experience.
Quantitative sampling was nonrandom. Truly random sampling was impossible with a population known for its mobility and limited telephone access. Female, younger, incarcerated, or severely ill individuals were underrepresented in this sample.
Further Study
The association between PWID–HCP rapport and health care use warrants examination in a larger, prospective cohort study. New recruitment strategies may need to be used to determine whether these research findings apply to less well-connected PWIDs. Knowledge sharing and other potential solutions to documented rapport-related problems require additional consultation with PWIDs, front line HCPs, health promotion experts, and policy makers prior to implementation.
Conclusion
Multiple patient, HCP, and system characteristics influence PWID–HCP rapport, including the level of perceived discrimination and autonomy support as well as the success of negotiation strategies used by both parties to fulfill their expectations. Drug dependence is a health issue central to the lives of patients, and it influences HCP and patient behavior. HCPs and health care policy makers are encouraged to foster strong, long-term patient–HCP relationships to improve PWID adherence to HCP recommendations, timing of health care, HCP continuity, avoidance of criminal activity, and satisfaction with care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This research was supported by a grant from the Canadian Institutes for Health Research.