
Abstract
Mathematics self-efficacy plays an important role in the performance of quantitative tasks. The objective of this study was to examine the role of mathematics self-efficacy in numeracy and health numeracy among immigrants (60 Mandarin-speaking and 60 Kikuyu-speaking immigrants to Canada) for whom English was a second language (ESL). Two French Kit numeracy tasks (the addition, and the addition and subtraction correction tasks) constituted objective measures of numeracy, and the numeracy component of a health literacy instrument (The Short Test of Functional Health Literacy for Adults [S-TOFHLA]) constituted the health numeracy measure. We measured math self-efficacy using the Mathematics Self-Efficacy Scale (MSES) and the Subjective Numeracy Scale (SNS). All measures were presented in English. Kikuyu speakers had lower math self-efficacy (p < .05) compared with Mandarin speakers (p < .05). Mandarin speakers outperformed Kikuyu speakers in numeracy (p < .001) and health numeracy (p < .023) skills. In multiple regression analyses, 32% to 57 % of the variance in objective numeracy was explained by language, residency in Canada, and self-efficacy, adjusting for the other predictor variables; self-efficacy and format of numeric health information (numbers only vs. numbers with detailed text) consistently predicted health numeracy. Mathematics self-efficacy may be an important factor in numeracy, but not as important in health numeracy for Kikuyu- and Mandarin-speaking immigrants for whom English is a second language. Factors contributing to low numeracy may differ from those explaining low health numeracy in ESL immigrants.
Introduction
Numeracy is the range of skills, strategies, and beliefs that people have or acquire to effectively interact with numbers in their daily lives (Gal, 2000). Health numeracy is a related but distinct concept that refers to the capacity to access and use numeric information in a health context (Nelson, Reyna, Fagerlin, Lipkus, & Peters, 2008; Schapira, Walker, & Sedivy, 2009). Low numeracy and low health numeracy are both associated with poor management of disease and difficulties accessing health care services (Ciampa, Osborn, Peterson, & Rothman, 2010; Huizinga et al., 2009), especially in vulnerable populations. Studies show that immigrants have low levels of numeracy and health numeracy. In the 2003 International Adult Literacy and Skills Survey, immigrants in Canada performed lower on numeracy compared with native-born Canadians (Statistics Canada, 2005); similar numeracy and health numeracy gaps exist between immigrant and non-immigrant populations in the United States (Choi, Rush, & Henry, 2013). Low levels of numeracy and health numeracy might explain immigrants’ worse health outcomes compared with the general population (Kreps & Sparks, 2008; Zanchetta & Poureslami, 2006).
An important aspect of an individual’s numeracy is self-efficacy, which is the belief in one’s capability to engage in a given task or behavior and produce a desired outcome (Bandura, 1977). Self-efficacy theory holds that an individual’s perceived self-efficacy influences and is itself influenced by affect and task performance factors (Bandura, 1982). An important source of self-efficacy is active mastery experiences, or an individual’s prior successes with similar tasks; these experiences are foundational to one’s perception of his or her ability to successfully execute a task in a specific domain (Bandura, 1997). In mathematics, self-efficacy refers specifically to an individual’s assessment of his or her ability to perform a mathematical or numeric task and produce a desired result (Hackett & Betz, 1989). Similar to general self-efficacy, mathematics self-efficacy depends on prior personal successes with numeric concepts and processes related to quantitative tasks.
Although all human languages include the concept of quantity, the representation and meaning of numbers may differ. For example, Kikuyu, a Bantu language spoken by the Agikuyu people of Kenya, has only one numeric concept embedded in the language structure (Leakey, 1977; Zavlasky, 1973). Kikuyu does not include the concept of rational numbers (or fractions), and speakers of this language may have limited experiences with the processes and outcomes relating to these concepts. Thus, one might hypothesize that Kikuyu speakers would have low math self-efficacy when presented with a task that requires use of such numeric concepts. In contrast, speakers of languages with multiple numeric concepts in their linguistic structure (such as Mandarin; Miura, Okamoto, Vlahovic-Stetic, Kim, & Han, 1999) may have greater math self-efficacy because of prior experience, familiarity, and success with these concepts. The relationship between numeracy, health numeracy, and math self-efficacy has not been well characterized. However, a few reports suggest that mathematics self-efficacy improves health outcomes. Greater math self-efficacy was associated with better diabetes self-management among participants from diverse racial, ethnic, and literacy backgrounds (Sarkar, Fisher, & Schillinger, 2006). Other reports show that health numeracy skill and self-efficacy play important roles in glycemic control among diabetics (Osborn, Cavanaugh, Wallston, & Rothman, 2010). However, these studies did not address mathematics self-efficacy in the context of numeracy and health numeracy among people with different primary languages and for whom English is a second language. Primary language is important because of its association with arithmetic memory and linguistic representation (Campbell & Epp, 2004).
In this study, we explored the role of mathematics self-efficacy on numeracy and health numeracy among immigrants who spoke different primary languages (Mandarin and Kikuyu), and with English as their second language. We focused on these two linguistic groups for a number of reasons. First, studies show that bilingual speakers apply their primary language framework when they encounter a mathematical problem in a second language (Bernhardt, 1991). Second, these languages differ in the number of embedded numeric concepts with Kikuyu having fewer numeric concepts than Mandarin. Third, although speakers of Mandarin and Kikuyu differ in the language in which they received mathematical instruction, they may be able to retrieve and use numeric concepts and processes in the language in which they learned the numeric concepts (Spelke & Tsivkin, 2001). Kikuyu speakers received formal instruction in English from Grade 3 onward in Kenya; Mandarin speakers were instructed in Mandarin throughout their educational experience in China.
We tested the hypothesis that immigrants who spoke Mandarin would be comfortable with the numeric concepts because of the presence of such concepts in their primary language, and therefore, they would have greater math self-efficacy and better performance in numeracy and health numeracy tasks although these tasks were presented in English. In contrast, speakers of Kikuyu, a language with fewer numeric concepts, would have less math self-efficacy and low performance in numeracy and health numeracy tasks, even though the tasks were presented in English, a language with which they were familiar. Our underlying rationale was to identify factors influencing health numeracy and the uptake of numeric health information by English-as-a-second-language (ESL) immigrants.
Method
Setting and Study Participants
Kikuyu and Mandarin-speaking immigrants to Canada were recruited from Southern Ontario urban centers by posters in churches, temples, and recreational centers. Initial recruits helped to identify potential participants within their community circles (Berg, 2009). We assumed a medium effect size (f 2 = .15), an α level of .05, and a power of 0.80 (Green, 1991) resulting in a sample of 120 participants.
Participants were (a) recent immigrants to Canada (<15 years in Canada); (b) bilingual (spoke Kikuyu or Mandarin as their primary language and English as their second language); (c) able to read, speak, and write in English, and in their primary language of Kikuyu or Mandarin; and (d) 40 years or older. A small honorarium of Can$30 was provided to each participant. Full ethics approval was given by the University Research Ethics Board.
Data and Measures
Five instruments, described below, were used to collect data.
Socio-demographic questionnaire
The items included age, gender, employment, income, length of residence in Canada, first language spoken as a child, and education level, and were adapted from published reports on prose literacy of ESL immigrants to Canada (e.g., Todd & Hoffman-Goetz, 2010). Two numeracy relevant questions were added: whether participants enjoyed learning math in school (yes/no) and their preferred format for numeric health information (numbers only/numbers with detailed text).
Numeracy assessment
Participants were assessed for basic numeracy using two French Kit tasks that were administered and responded to in print form (Ekstrom, French, Harman, & Dermen, 1976): an addition task with 60 problems each with 1 or 2 digit numbers where participants provided a solution, and an addition–subtraction correction task with 60 solved problems where participants marked “X” on the letters “C” for “correct” or “I” for incorrect for each problem. Each task was timed at 2 min per page according to the developer’s instructions; to reduce test anxiety, the participants were not informed of the timed nature (Ashcraft & Moore, 2009). The French Kit has been used to assess mathematics problem-solving skills in adults (Campbell & Gunter, 2002; Thevenot, Fanget, & Fayol, 2007).
Health numeracy assessment
The Short Test of Functional Health Literacy for Adults (S-TOFHLA) measures health literacy and health numeracy (Baker, Williams, Parker, Gazmararian, & Nurss, 1999). The health numeracy component comprises four questions (weighted score of 28). Participants read printed test items and answered orally. S-TOFHLA numeric has been used with immigrants (Shaw, Armin, Torres, Orzech, & Vivian, 2012) and seniors (Kirk et al., 2012). Although the full S-TOFHLA (prose and numeric components) was administered, we excluded the prose component from analyses because it was not directly relevant to our study hypothesis on self-efficacy and numeracy.
Math self-efficacy assessment
We used the Mathematics Self-Efficacy Scale (MSES) and the Subjective Numeracy Scale (SNS) to measure self-efficacy in performing math tasks. The MSES, a 52-item instrument (Betz & Hackett, 1983), consists of three subscales: the 18-item Mathematics Tasks subscale that measures confidence in ability to perform “every day” math tasks, the 16-item Mathematics Courses subscale that assesses confidence in performance in math courses, and the 18-item Mathematics Problems subscale that measures confidence in ability to solve mathematics problems. We used the Mathematics Tasks subscale because of its relevance for assessing functional numeracy in adults. The other subscales have been used for student performance in a classroom setting and were not used here. Participants were asked to assess their math self-efficacy using a 10-point scale (0 = no confidence; 9 = complete confidence). An example of an MSES test item is “How much confidence do you have that you could successfully: Add two large numbers in your head?” The test takes about 10 min to administer and respondent burden is low. The 8-item SNS assesses individuals’ perception of their mathematical abilities and preference for numerical information (Fagerlin et al., 2007). The test uses a Likert-type scale from 1 to 6. Questions from the SNS test include the following: “How good are you at figuring out how much a shirt will cost if it is 25% off?” and “When people tell you the chance of something happening, do you prefer that they use words (“it rarely happens”) or numbers (“there’s a 1% chance”)? SNS takes about 5 min to administer. Both the MSES and the SNS are administered and responded to in print form.
Statistical Analysis
Data were analyzed using SPSS Version 21.0. General descriptive statistics summarized socio-demographic, numeracy, and health numeracy data. The means of the self-efficacy measures (MSES and SNS), numeracy measures (French Kit), and health numeracy (numeracy component of S-TOFHLA) by the two immigrant ESL groups were examined for differences using the Mann-Whitney U test. Spearman correlation was used to test relationships between MSES and SNS. Multiple regression analyses were conducted to determine whether math self-efficacy contributed to numeracy skill after adjusting for the socio-demographic factors (age, gender, language, length of residency in Canada, income, employment, and education). Using forward and stepwise methods, all variables that had a p value of .05 were identified and forced into the final regression models. For analyses of health numeracy skill, the variables of math enjoyment and preferred numerical format were included in the initial models.
Results
Socio-Demographic Characteristics of Participants
Table 1 shows the socio-demographic characteristics of the participants. There were more women than men (61% vs. 39%) in the study. The majority of participants (73%) were between 40 and 50 years old, and more Mandarin speakers had at least a university education than did Kikuyu speakers (about 70% vs. about 40%). More Kikuyu than Mandarin speakers (about 28% vs. 15%) were recent immigrants to Canada having emigrated < 5 years ago. More Mandarin-speaking immigrants enjoyed learning math than Kikuyu-speaking immigrants (97% vs. 73%). Most participants preferred health information to be provided as numbers with detailed text explanation than as numbers alone (91% vs. 9%).
Socio-Demographic Characteristics of 120 Chinese and Kenyan ESL Immigrants.
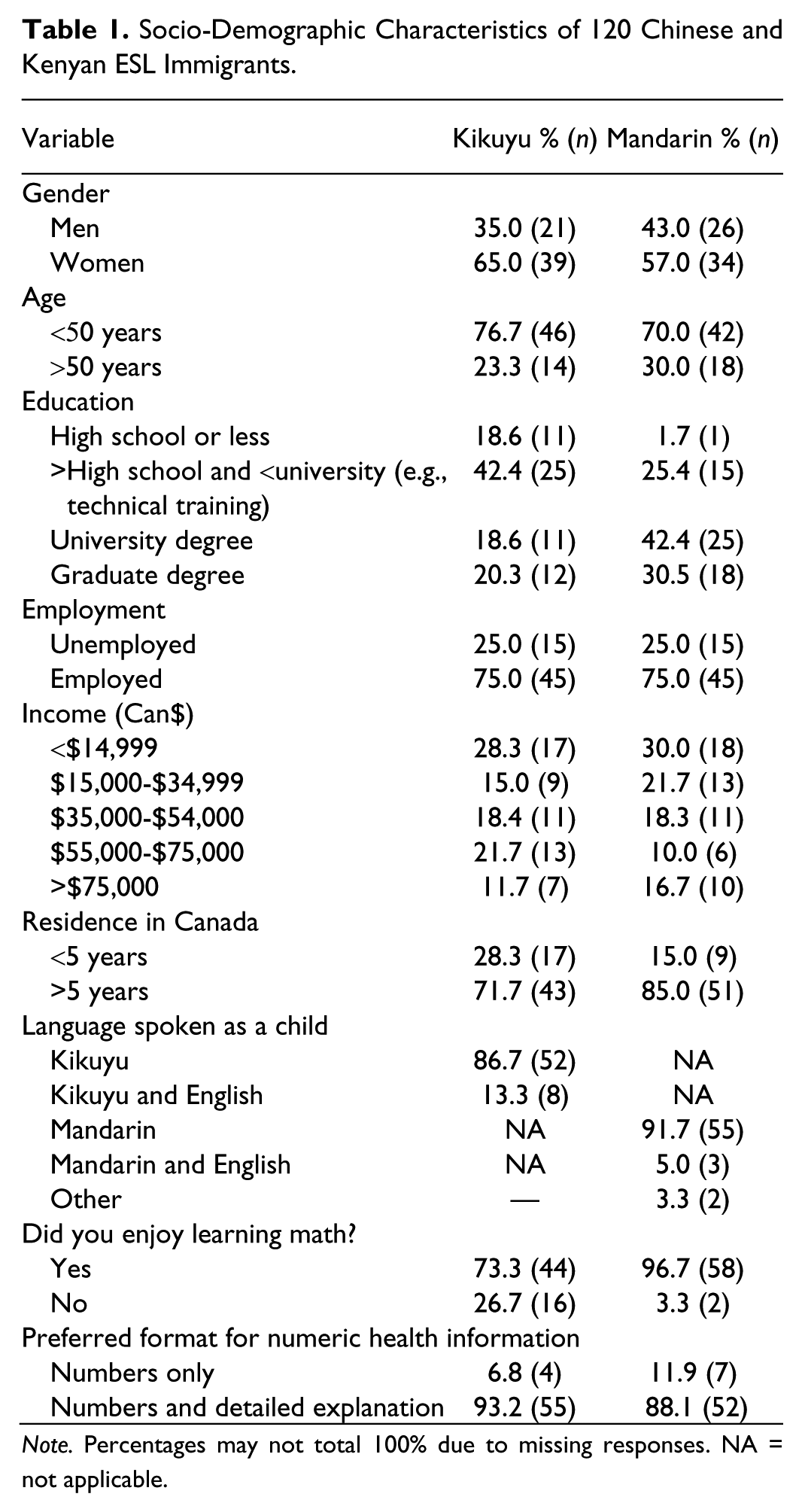
Note. Percentages may not total 100% due to missing responses. NA = not applicable.
Mathematics Self-Efficacy Characteristics of Participants
For measures of math self-efficacy (math self-efficacy and subjective numeracy) by language, Kikuyu-speaking immigrants expressed lower confidence compared with Mandarin-speaking immigrants. The differences in the means (Table 2) were statistically significant (p < .05). MSES and SNS scores were highly correlated (rs = .94, p < .001). Men had higher self-efficacy than women, and the differences were statistically significant (MSES: U = 878.5, p < .005; SNS: U = 941.5, p < .001). There were more Kikuyu speakers who had only a high school education or less (11 participants) compared with Mandarin speakers (1 participant). To ensure that these differences in education level between Mandarin and Kikuyu speakers did not affect the self-efficacy results, we performed a separate analysis excluding the 12 participants who had an education level at high school or below and obtained results similar to those using the full sample (Table 2). We therefore performed all subsequent analysis using the full sample.
Math Self-Efficacy and Subjective Numeracy Characteristics of Participants.

Note. CI = confidence interval; MSES = Mathematics Self-Efficacy Scale; SNS = Subjective Numeracy Scale.
Numeracy and Health Numeracy Characteristics of Participants
Virtually, all Mandarin speakers (~98%) enjoyed learning math compared with about three quarters of Kikuyu speakers (~73%). This difference was statistically significant, χ2(1, n = 120) = 12.81, p < .001. We used context-free French Kit mathematics tasks to assess participants’ numeracy skills. The means for Mandarin speakers in the addition task (M = 16.23, 95% confidence interval [CI = 14.95, 17.51]) and the addition–subtraction correction task (M = 33.85, 95% CI = [31.22, 36.48]) were significantly higher than for Kikuyu speakers (M = 11.70, 95% CI = [10.52, 12.88] and M = 19.37, 95% CI = [17.52, 21.00]; U = 918.0, p < .001 and U = 456.0, p < .001, respectively). Statistically significant differences in performance based on gender were observed only in the addition–subtraction correction task (U = 1,381.5, p = .036), with men outperforming women.
For scores on the health numeracy component of S-TOFHLA, Mandarin speakers were marginally better (M = 25.55, 95% CI = [24.56, 26.54]) than Kikuyu speakers (M = 23.33, 95% CI = [21.93, 24.73]; U = 1,413.50, p = .023). There was no gender difference in health numeracy performance.
Predictors of Numeracy and Health Numeracy
To determine whether math self-efficacy of participants predicted numeracy and health numeracy skill, multiple regression analyses were run. Predictor variables included in the final models were language (Kikuyu, Mandarin), gender (male, female), residence in Canada (<5 vs. >5 years) and age (<50 vs. >50 years). The rationale for grouping age as <50 and >50 years was because older adults have been shown to have lower numeracy skill than younger individuals. Education (in four categories: high school or less, more than high school but less than university [e.g., trade school, certificate], university, and graduate education) was also included; from these four education categories, we constructed three dummy variables (k − 1) for use in regression modeling, and with the high school or less category as the reference for the other education variables. For health numeracy (S-TOFHLA numeracy component), format of presentation of numeric information (numbers only vs. numbers with explanation) was also included in the final regression models. MSES and SNS were run in separate models because of the high collinearity between these measures.
Table 3 shows the regression models for the predictors of numeracy (French Kit addition, and addition–subtraction correction tasks) with the inclusion of MSES and SNS. Using MSES, prediction for basic numeracy skill on the addition task produced a final model, F(7, 109) = 8.64, p ≤ .001, that accounted for about 32% of the variation in the numeracy score. Adjusting for other variables, language, residency in Canada, and MSES score were significant in explaining the variation in the addition task score. Also shown is the final model, F(7, 109) = 21.71, p < .001, that accounted for about 56% of the variance in the addition–subtraction correction score. Controlling for other variables, language, residency in Canada, university education, and math self-efficacy significantly accounted for the variation in the scores. Overall, Mandarin speakers, individuals with longer residency in Canada, and those with higher mathematics self-efficacy (MSES) performed better on the two tests of basic numeracy. Table 3 provides the final regression model with the SNS measure of mathematics self-efficacy. For the addition and the addition–subtraction correction tasks about 30%, F(7,108) = 8.12, p < .001, and 57%, F(7,108) = 23.16 p < .001, of the variation in the scores were explained. Adjusting for the other variables, language, residence in Canada, and math self-efficacy were significant predictors of the variation in the addition task performance. Language, having a university education, and self-efficacy contributed significantly to the variation in performance on the addition–subtraction correction task, after controlling for other variables (e.g., gender and residency in Canada).
Predictors of Basic Numeracy (French Kit Addition Task and Addition–Subtraction Correction Task).

Note. MSES = Mathematics Self-Efficacy Scale; SNS = Subjective Numeracy Scale.
High school or less education category was the reference for these education levels.
The results of the regression models to predict health numeracy skill (S-TOFHLA numeracy) are shown in Table 4. The variables of gender, language, education, residency in Canada, self-efficacy, and preferred format for numeric health information were included. Analysis with MSES resulted in a final model, F(8, 106) = 2.62, p = .012, that accounted for about 10% of the variation. Adjusting for other variables, only format (numbers vs. numbers with explanation) was a significant predictor of health numeracy. The final model with SNS, F(8, 105) = 3.20, p = .003, accounted for 14% of the variance. Adjusting for other variables, preferred format for numeric health information, and math self-efficacy were the only significant predictors of health numeracy.
Predictors of Health Numeracy (S-TOFHLA Numeracy Component).

Note. S-TOFHLA = Short Test of Functional Health Literacy for Adults; MSES = Mathematics Self-Efficacy Scale; SNS = Subjective Numeracy Scale.
High school or less education category was the reference for these education levels.
Preferred format of numeric health information.
Discussion
We tested the role of math self-efficacy in the performance of basic numeracy and health numeracy tasks among ESL immigrants to Canada. We found that self-efficacy predicted numeracy performance and, to a lesser extent, health numeracy performance. Other factors associated with some of the differences in participant skill on numeracy tests were language and duration of residence in Canada. Gender did not contribute to performance for numeracy and health numeracy. Preference for numeric information format was significantly associated with variation in health numeracy scores.
Self-efficacy in one’s ability to perform basic mathematical tasks, measured by the MSES and SNS, consistently predicted performance on basic numeracy tests (addition, and addition–subtraction correction) among Chinese and Kenyan immigrants who were non-native speakers of English. These results were not surprising given the role of self-efficacy and mathematical problem solving (Hackett & Betz, 1989). A person’s self-efficacy beliefs influence his or her motivation, disposition, and behavior (Bandura, 1989), and provide the interest, the needed attention, and the tenacity to complete a task (Pajares & Kranzler, 1995). Studies show that prior performance and success in a given domain are important predictors of math self-efficacy (Lent, Lopez, & Bieschke, 1991; Rosenstock, Strecher, & Becker, 1988). High math self-efficacy is associated with low anxiety and better performance in situations involving numbers. Indeed, perceived high mathematics self-efficacy among university students was found to be inversely associated with statistics anxiety (Bandalos, Yates, & Thorndike-Christ, 1995)
In our sample of Kikuyu and Mandarin-speaking immigrants, language contributed to performance on basic numeracy tasks (addition, and addition–subtraction correction). Studies show that East Asian students perform better in mathematics than Western students (Geary, Bow-Thomas, Fan, & Siegler, 1993; Stevenson, Lee, & Stigler, 1986). This is attributed in part, to East Asian languages having more numeric concepts embedded in their structure (Miura, Okamoto, Kim, & Chang, 1994). Familiarity with these numeric concepts through regular use and repeated practice may contribute as well. Lefevre and Liu (1997) compared mathematics performance of adults educated in China and Canada and found that adults educated in China performed better in mathematical assessments than adults educated in Canada; one factor appeared to be early exposure to, practice of, and success with mathematical concepts in the primary language. A review of linguistic and cultural factors that influence performance in mathematics across nations showed that number words in Mandarin gave advantage to children in learning and performing mathematical tasks (Ng & Rao, 2010). Another perspective is that teaching mathematics at the primary level in East Asian countries stresses mastery of content and rote learning (Leung, Ko, Chan, Chi, & Chow, 2007) that could potentially allow for easier retrieval of numeric concepts and processes stored in long-term memory (Campbell & Epp, 2004). However, other cultural and system factors that were beyond the scope of this study could also contribute to this superior performance in mathematics (Leung, 2001).
Duration of residence in Canada predicted basic numeracy, with shorter duration predicting lower numeracy skills. Duration of residence in the host country is a complex variable signaling not only how long a person has lived in the new country but also, albeit not exclusively, the degree of acculturation. Acculturation has been shown to have a role in immigrants’ health literacy through exposure, interest, and interaction in various aspects of the new culture, interaction with health information in English, and opportunities to practice English prose skills (Ciampa et al., 2010). Despite the concern that temporal measures are an inaccurate proxy for acculturation, the length of residency in the host country has been shown to play a role in the acculturative process (Bharmal, 2013). Regarding numeracy, Driessen and Merry (2011) found that long periods of residence by immigrants to the Netherlands were associated with higher numeracy levels. It is not known why duration of residence was associated with greater numeracy skills of immigrants in our study. Several factors may contribute to this association, including interactions with more people who are numerate (Ciampa et al., 2013) and increased opportunities to utilize numeracy skills, such as filing tax returns, paying bills, and adding receipts (Charette & Meng, 1998). Programs existing to help immigrants integrate into the community could also provide opportunities to improve numeracy skills (McHugh & Challinor, 2011)
Gender was not a predictive factor for numeracy or health numeracy skill in our study. Gender is a controversial variable in quantitative literacy skill. Some studies have failed to find important differences in math performance by gender (Devine, Fawcett, Szucs, & Dowker, 2012), whereas others have shown differences. For example, in a study comparing Chinese female and male children’s performance in arithmetic, girls outperformed boys in arithmetic, whereas boys outperformed girls on spatial processing (Wei et al., 2012). Other studies have shown men outperforming women in mathematic tasks (Gallagher & De Lisi, 1994; Royer, Tronsky, Chan, Jackson, & Marchant, 1999), whereas still others report the opposite with women outperforming men (Hyde, Fennema, & Lamon, 1990). Recent studies have questioned the traditional (North American) view of males possessing superior mathematical skills to those of females. In a multinational review of mathematical competence, the gap between men and women in mathematics performance in the United States, Iceland, Thailand, the United Kingdom, and Indonesia disappeared, with females performing at par with males in a variety of basic mathematical tasks (Hyde & Mertz, 2009). A reason for these findings may be the changing gender equality expectations resulting in an increasing enrolment by girls in the educational system (Guiso, Monte, Sapienza, & Zingales, 2008).
Mathematics self-efficacy was not a consistent predictor of health numeracy performance of ESL immigrants (only weakly so in the SNS and not at all in the MSES measure). This finding was surprising: We expected the strong math self-efficacy effects observed for basic numeracy performance would carry over to health numeracy. Yet, it can be argued that health numeracy involves different skills from basic numeracy. Basic numeracy requires individuals to identify numbers and perform simple operations (such as addition) in a context-free setting (Ginsburg, Bickerton, Southwood, & Hinds, 2011). Health numeracy requires individuals to not only have number recognition and perform simple operations but also engage in complex processing, interpreting, and sense-making of quantitative information in a health-specific setting (Golbeck, Ahlers-Schmidt, Paschal, & Dismuke, 2005). Thus, basic numeracy is a necessary but not a sufficient factor for health numeracy. Familiarity with the health context, judgment about risks, and other non-numeracy factors likely contribute to health numeracy.
Our findings imply that these other factors are not captured by the MSES measure and only weakly so by the SNS.
The finding that preferred format for numeric health information contributed to variation in health numeracy performance supports a role for factors other than math self-efficacy. Participants indicated a preference for numeric health information presented as numbers with detailed explanations. The S-TOFHLA numeracy test comprises four questions that combine text and numerical information. For all questions, participants first read the instructions and then answered oral questions. Participants who stated they preferred numeric health information as a combination of numbers with detailed explanation outperformed those who preferred information as numbers only. Others have recommended combining verbal explanations with numbers, or presenting all the information qualitatively when presenting numeric health information to people with low health numeracy (Gordon-Lubitz, 2003; Paling, 2003). Brewers and colleagues (2009) found that information formats that combined verbal with numeric information received the highest rating among breast cancer survivors. However, there is little consensus about what constitutes the best format for presenting numeric health information to the general population, much less for immigrants; factors including basic numeracy skill, age, education, language, disposition, and culture influence numeric format preference (Lipkus, 2007; Timmermans, Ockhuysen-Vermey, & Henneman, 2008; Wright, Whitwell, Takeichi, Hankins, & Marteau, 2009).
Although Mandarin-speaking immigrants had marginally better health numeracy scores than Kikuyu-speaking immigrants, language was not an important predictor of variation in S-TOFHLA numeracy scores. The reason for this is not evident from our data. However, the S-TOFHLA health numeracy questions tap numeric and prose concepts rather than only health numeracy. Moreover, participants responded orally, requiring sufficient comprehension of the questions being asked. Both of these factors may have affected the impact of language on test results.
We found that educational level was not a consistent factor in predicting variation in numeracy or health numeracy scores in our sample of ESL immigrants. Only education at the university level was predictive of performance in one component of the French Kit (the addition and subtraction correction task). Despite high educational attainment in our sample (about 40% of Kikuyu and 70% of Mandarin speakers held at least a university degree), this had little impact on numeracy and health numeracy skill. Others have reported that speakers whose first languages are other than English (including Asian languages) have poor numeracy despite high educational qualifications (university degrees; Smyth & Lane, 2009). In contrast, findings from the International Adult Literacy Survey (including data for Canada) show that individuals with higher education (college or university) score higher on all domains of literacy (including numeracy) than those with less education (high school or less). Yet, the impact of primary language persists: Even after 30 years of having spoken the test language (English), a gap of more than 25% of a standard deviation remained in literacy performance of non-native speakers of English, which translated into 2 years of schooling (Willms, 1997). This language gap is also suggested by our study: The effect of speaking a minority language (Kikuyu or Mandarin) as the first language was a strong influence on numeracy whereas formal education level only modestly, if at all, mitigated the impact of language.
Limitations
This study has limitations. First, we used a convenience sample rather than a probability sample based on Canadian census data. Random sampling was not possible because no reliable sampling frame exists for Kenyan (Kikuyu-speaking) immigrants to Southern Ontario. Consequently, a convenience sample using networking and snowball sampling was the best approach to reach this population. The same strategy was applied to Mandarin-speaking immigrants to maintain consistency in study design. Second, the instrument used to capture health numeracy (the numeric subtest of S-TOFHLA) was not developed as a stand-alone measure of health numeracy. Another more recent test—the Numeracy Understanding in Medicine Instrument (Schapira et al., 2012)—may have resulted in different self-efficacy effects; however, this test was not available at the outset of our study. Moreover, S-TOFHLA is a widely accepted measure of health literacy and numeracy and has been used in ESL populations (Donelle, Arocha, & Hoffman-Goetz, 2008). Third, format preference for numeric health information was captured by a single prose item on the questionnaire rather than providing illustrations (e.g., a pie graph) or by multiple questions to establish face validity. For future studies, additional response categories may provide insights into the role of format in numeric health information for ESL immigrants. Fourth, education levels differed between Kenyan and Chinese immigrants but were not a significant predictor of numeracy or health numeracy. This was not unexpected because attained education remains an imperfect marker for health literacy (Chew, Bradley, & Boyko, 2004) and, from our study, health numeracy. Fifth, we did not (and could not) measure political and cultural factors in China and Kenya that potentially influence math self-efficacy of the ESL immigrants in our study. Finally, although the literature shows that low health numeracy is associated with poor health outcomes of immigrants and vulnerable populations, we did not measure health outcomes or health status in our ESL populations. Future research incorporating clinical measures will be needed to determine how primary language, math self-efficacy, and numeracy affect the actual health status of non-native speakers of English.
Contribution to Literature
Health information is often presented with numbers and percentages, and immigrants face challenges understanding such information. We examined the impact of math self-efficacy on numeracy and health numeracy in Mandarin-speaking and Kikuyu-speaking immigrants to English Canada. We found that although math self-efficacy contributes to performance in basic numeracy, it may be less important in health numeracy. Self-reported preferred format for presenting numeric health information was associated with better health numeracy among our immigrant sample. Our findings suggest that public health interventions to improve numeracy for ESL immigrants may differ from those needed to improve health numeracy.
Footnotes
Acknowledgements
The authors thank Dr. S. K. Brown for statistical advice. Dr. J. Guan is acknowledged for help with participant recruitment. The Mandarin- and Kikuyu-speaking participants in this study are gratefully thanked.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The research was supported by a grant from the Social Sciences and Humanities Research Council of Canada.