
Abstract
eHealth literacy (eHEALS) has yet to be examined with regard to need for cognition (NFC), as well as whether NFC moderates the relationship between eHealth literacy and seeking out online health information. Past research that has examined NFC as an interaction between whether interactivity on health web sites affected comprehension and attitudes, but no research to date has examined whether cognitive need interacts with eHEALS and subsequent information seeking behaviors. The present study tests eHEALS and its connection to need for cognition (NFC) in the role of online health information seeking behaviors. Results showed that high eHEALS individuals were more likely to seek out online health information and were more likely to have higher NFC scores. NFC did not emerge as a moderator on the relationship between eHealth literacy and online health information seeking behaviors. Future directions are discussed, in particular, examining eHEALS as a construct of efficacy and further need to examine eHEALS with need for cognition in health communication research.
eHealth interventions have targeted concerns such as physical activity and behavior change (G. J. Norman et al., 2007); asthma management in low-income families (Wise et al., 2009); and self-management for adjustment after curative breast cancer (van den Berg, Gielissen, Ottevanger, & Prins, 2012). It is crucial for individuals to develop eHealth literacy skills to better understand, evaluate, and use the health-related information that is disseminated online (Jensen, King, Davis, & Guntzviller, 2010; Sarkar et al., 2010). eHealth literacy (C. D. Norman & Skinner, 2006) has a reliable and consistent measure known as eHEALS that, in recent research, has shown promise as a tool for assessment in using information technology for health purposes (e.g., van der Vaart et al., 2011).
eHealth literacy skills are especially important to develop in young adults because these skills will inform their decision-making processes later in life. Linking electronic health information seeking behaviors to need for cognition (NFC) is important to see if there are differences among young adults who are less vested in cognitive thought as opposed to those who are. This investigation can give insight as to how young adults are developing their health-related decision-making skills along with their NFC, two processes that will carry them through their adult life. Research has examined the use of the electronic health literacy scale (eHEALS, C. D. Norman & Skinner, 2006), but studies have yet to connect health literacy to NFC, particularly in the young adult population.
A growing body of research in the leading journals on health communication has cited a critical need to conduct research on how health literacy skills in young adults influence health information-seeking behaviors, particularly through the use of new Internet technologies (Benjamin, 2010; Berkman, Davis, & McCormack, 2010; Dutta-Bergman, 2005; Eng, 2002; Manganello & Clayman, 2011; Paek & Hove, 2012). As such, this study aims to address how health literacy impacts young adults’ information-seeking behavior on the internet. This study is also interested in examining a possible relationship between higher levels of eHealth literacy and young adults’ engagement in healthy behaviors, such as engaging in physical activity.
In the present study, eHEALS is connected to NFC and online health information seeking behavior. Furthermore, we propose that eHEALS items could be measuring health self-efficacy rather than literacy, thus building off prior work suggesting eHEALS is not necessarily a reliable measure of health literacy (Jordan, Osborne, & Buchbinder, 2011). Traditional literacy measurements tend to include items that test proficiency (National Center for Education Statistics, 2012), rather than items about perceived ability, which are traditionally items that belong in the domain of social cognitive theory (Bandura, 1986). eHEALS has not been examined with regard to NFC, nor has the role of NFC as a moderator of the relationship between health information seeking and eHEALS. Past research that has examined NFC as an interaction between whether interactivity on health websites affected comprehension and attitudes (Lustria, 2007), but no research to date has examined whether NFC interacts with eHEALS and subsequent information seeking behaviors. Thus, this study aims to contribute to the growing body of literature on eHealth literacy and information seeking behaviors by (a) examining the relationship between cognitive need and use of seeking out health information online; (b) the role of eHealth literacy, seeking out information online, and whether cognitive need plays a role in that behavior; and (c) the connection between levels of eHealth literacy and enactment of healthy behaviors.
eHealth Literacy
Health literacy is, as defined in the U.S. Department of Health and Human Services Healthy People 2010 report, “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions” (Location 12). Health literacy goes beyond basic reading ability. It includes the ability to understand instructions on drug usage, appointment cards and brochures, and directions, as well as the ability to navigate complicated health care systems. The eHealth literacy scale (eHEALS), though, provides a measure of an individual’s self-perceived skill and self-efficacy in using information technology for health purposes (C. D. Norman & Skinner, 2006). eHEALS has been tested in intervention trials and population surveys in multicultural samples with strong internal consistency and reliability.
The National Institutes of Health (2012) has current efforts dedicated to continuing to develop and improve health literacy. The U.S. Department of Health and Human Services (2012) has compiled recommendations for developers and practitioners to develop easy to use health web sites that put action behaviors first and engage people.
The Elaboration Likelihood Model and Need for Cognition
Need for cognition (NFC) is one of the most studied individual factors in message processing and persuasion (Cacioppo, Petty, & Kao, 1984). The Elaboration Likelihood Model (ELM; Petty & Cacioppo, 1986) and Heuristic Systematic Model (Chaiken, Liberman, & Eagly, 1989) designate NFC as a way to assess individual differences in cognitive effort. ELM is a model that focuses on how attitudes develop and change over time, and designates NFC as the central factor that influences cognitive involvement. Based on the role of persuasion and message processing, people high in NFC tend to enjoy thinking without external influences and tend to more closely scrutinize communication in addition to processing information more actively and more in-depth (Chang & McDaniel, 1995; Verplanken, Hazenberg, & Palenewen, 1992). Most importantly, though, individuals high in NFC are more intrinsically motivated to think as opposed to those who are low in NFC (Haugtvedt & Petty, 1992). Similarly, high NFC individuals tend to engage in online activity that requires more cognitive effort (Tuten & Bosnjak, 2001). Recommendations on examining health literacy have suggested that a key connection is the individual’s need to engage in cognitive thought (Safeer & Keenan, 2005) and that the NFC scale can lend important insight.
Research on cognitive involvement, or the degree to which an individual is intensely involved in some stimulus, has largely been examined using theoretical frameworks such as the Elaboration Likelihood Model (e.g., Petty & Cacioppo, 1986), which examine the role of one’s level of cognitive involvement when presented with stimuli. The need for cognition (NFC) is a variable that examines the extent to which one is involved with some stimuli that requires some cognitive output. For example, relatively recent research has explored NFC in terms of listening style preference and the relationship between high and low cognition (Worthington, 2008), the interaction of NFC and message type on positive health encouragement (Williams-Piehota et al., 2006), and understanding the dimensions of perceived interactivity in social interactions (Sohn & Lee, 2005). What is still missing from the literature is an exploration as to how NFC relates to eHealth literacy, particularly in the young adult population.
Need for Cognition as a Moderator in eHEALS and Health Information Seeking Behavior
Research using the NFC scale has explored how others’ reactions to news presented on the Internet affects individual perceptions of public opinions and as a result, their personal opinion (Lee & Jang, 2010). NFC was used as a moderator on the effects of approval rating and individual comments. High NFC individuals were more reliant on approval ratings, but low NFC individuals remained unaltered. Other research looked at the effectiveness of testimonials compared with informational health messages in regard to personal involvement (Braverman, 2008). There remains a need, however, to look at whether NFC is a factor in one’s use of the Internet to seek out information about health issues. New measures, such as the electronic health literacy scale (eHEALS; C. D. Norman & Skinner, 2006), have emerged as a response to the growing need for examining electronic health literacy. But, as the authors earlier suggest, items in eHEALS tend to reflect efficacious beliefs (i.e., “I know how to use the Internet to answer my health questions,” “I have the skills I need to evaluate the health resources I find on the Internet”), rather than literacy-based items. In any case, eHEALS has been found to be a tight fitting scale with high correlational values and a strong body of support (Knapp, Madden, Wang, Sloyer, & Shenkman, 2011; van der Vaart et al., 2011), and is being adapted in multiple languages (e.g., Koo, Norman, & Chang, 2012; Mitsutake, Shibata, Ishii, Okazaki, & Oka, 2011).
Researchers have used NFC as an interaction term with other constructs. Individual attitudes such as trust in media sources may interact with gratifications sought when people shape their media usage (Tsfati & Cappella, 2005). Some research has investigated the interactive effects of NFC; for instance, Priester and Petty (1995) examined source credibility and its interaction with NFC on persuasion and message processing. They found that message processing of low NFC individuals tended to be influenced by source credibility, whereas high NFC individuals tended to be less influenced by source credibility. Here, NFC interacted with source trustworthiness, providing an early rationale for NFC as an interaction term. More recently, Tsfati and Cappella (2005) examined the role of NFC as interacting with media skepticism and the joint effect on media exposure. NFC significantly interacted with media skepticism in the effect on mainstream news exposure—which Tsfati and Cappella argue that, as NFC goes up, the connection between news skepticism and news exposure disappears, thus supporting NFC as a moderator.
With regard to online information seeking behaviors, Lustria (2007) conducted an experiment to examine the effects of web interactivity on comprehension and attitudes toward health websites and whether individual differences moderated the effects. In that research, two websites on skin cancer were created by the researcher and evaluated by participants. Lustria found that whether or not the website had interactive information affected comprehension and attitudes, and predicted that high NFC individuals would have a higher comprehension score of website information compared with low NFC individuals. This is compelling because it suggests that high NFC individuals are more likely to engage in effortful information-seeking behaviors, and furthermore, that they understand more than those who do not enjoy thinking as much; importantly, comprehension is a critical facet of eHealth literacy.
Those higher in NFC may be more willing to invest time into satisfying that cognitive need, such as exposing themselves to new information, resulting in a decrease in selective exposure of media sources (Tsfati & Cappella, 2005). When NFC is high, the likeliness to have a cognitive need to seek out health information could also be high. On the other hand, when NFC is low, people may be less likely to seek out information online if they do not have a reason.
Research Design
To increase generalizability in the findings, this study used a survey design with university undergraduate students. A survey design (Alreck & Settle, 2004) allowed the researchers to directly ask participants questions about their use of the Internet for health purposes, the critical issues recommended by the CDC for college students, and answered the NFC and eHEALS scales. The present manuscript addresses the following questions: First, does need for cognition have a relationship with whether an individual has sought out health information online, and second, does it predict future intent to seek out health information online? With new measures like eHEALS, is there some relationship between level of cognitive exertion and this scale? The following research questions are offered:
Finally, in an attempt to contextualize the contribution of NFC and eHEALS, we sought out the relationship between eHealth literacy and healthy behaviors in the areas identified as key by the Centers for Disease Control: substance abuse, sleep, vaccination, sexual health, diet, and mental health. As such, the final research question asks,
Method
On IRB approval, data were collected in 2012 over a period of 3 months at a large Midwestern University in the United States. An online survey was distributed in a computer lab to university students. The survey was created to assess students’ use of the Internet to address health concerns or issues. The survey included the eHEALS scale (C. D. Norman & Skinner, 2006) and the abbreviated version of the Need for Cognition scale (Cacioppo et al., 1984).
A description of the survey is below, and the appendix contains the full survey.
Study Tool: Survey Measures
In the survey, participants first answered a series of demographic questions, followed by a question that asked whether they have a health condition that requires regular interaction with a physician. Participants were not asked to elaborate on this answer. The majority of participants did not report a condition (90.60%), but some did (9.4%; missing values = 3). After this, participants answered the eHEALS scale. Then, they completed four questions relating to how they maintain their general health, followed by blocks of four questions in each of the following areas: exercise, substance abuse, sleep, vaccination, sexual health, diet, and mental health. These health areas were selected because they were listed as the American College Health Association’s (2012) recommendations based on extensive research as the key issues affecting undergraduate students. Finally, participants responded to the NFC scale (unchanged). On completion of those questions, participants had completed the survey and were thanked for their time. The survey instrument is included as an appendix.
eHEALS
The eHEALS scale 1 is an 8-item measure of electronic health literacy (α = .93) to measure users’ knowledge, comfort and skills at finding, evaluating and using electronic health information (C. D. Norman & Skinner, 2006). Descriptives for eHEALS showed that M = 29.41, SD = 5.53. The eHEALS scale was developed to potentially serve as a way to identify people who may or may not benefit from referrals to an electronic health intervention. However, given the questions of the eHEALS scale, it can be argued that eHEALS is a better measure of electronic health self-efficacy. In the present manuscript, study results point toward eHEALS as related to self-efficacy, rather than as a pure measure of literacy.
Need for Cognition
The Need for Cognition scale (α = .81; NFC) refers to the tendency to engage in cognitive efforts and to enjoy such efforts. The initial NFC included 34 items, and two procedures resulted in decreasing the number of items in the scale to 18 (r = .95, p < .001; Cacioppo et al., 1984). All appropriate items that denoted ** were reverse coded. The descriptives for the summed NFC scale were M = 52.48, SD = 8.5.
Results
A total of 420 participants took the survey, ranging in ages 18 to 35 (M = 20.48, SD = 2.14), and all participants were undergraduate students (M = 2.76, SD = 1.15). Participants predominantly reported Caucasian/White as their ethnicity (78.6%), with some Asian/Pacific Islander (11.4%), African American (3.8%), Hispanic/Latino (3.3%), Other (2.6%), and four missing values.
Research Question 1 asked, “Will high NFC individuals will be more likely to have sought out health information online than low NFC individuals?” We ran a linear regression using the control variables of gender and age and the question “I have used Internet resources to help me understand or manage my health needs this semester” as the dependent variable and need for cognition scale as the predictor. The results of this regression are given in Table 1. No relationship was found between these variables (r = .036, p < .501). A second model regressed NFC onto intent to seek out health information (as opposed to past behavior), and again, no relationship was found (r = .005, p < .932). Research Question 1 was not supported.
Regression Model on High NFC Individuals Likeliness to Seek Out Health Information Online.

Note. NFC = need for cognition.
p < .0001.
Research Question 1a asked “Will high eHEALS individuals will be more likely to have sought out health information online than low eHEALS individuals?” Research Question 1a regressed the eHEALS score with “I have used Internet resources to help me understand or manage my health needs this semester.” A significant relationship was found (r = .275, p < .0001). Research Question 1a was supported, albeit with a small relationship (see Table 2 for the regression model).
Regression Model on High eHEALS Individuals Likeliness to Seek Out Health Information Online.

Note. eHEALS = eHealth literacy.
p < .0001.
Research Question 2 asked “Will individuals who score high on the NFC scale will also be high in self-efficacy, according to the eHEALS scale?” For Research Question 2, a linear regression was run with the question “I have used Internet resources to help me understand or manage my health needs this semester” as the dependent variable and the eHEALS score as the predictor (see Table 3). When the NFC score was entered into a regression model with eHEALS score as the dependent variable, a positive relationship was found (r = .179, p = .001). There was a small but significant relationship that at least suggests that individuals high in NFC may also be high in Internet health self-efficacy, according to eHEALS.
Regression Model Predicting High NFC Scores Are Also High in Self-Efficacy.

Note. NFC = need for cognition; eHEALS = eHealth literacy.
p <. 0001.
Finally, Research Question 3 suggested that as NFC increases, the relationship between health self-efficacy and health information seeking behavior becomes stronger. For Research Question 3, an interaction term was created (eHEALS × NFC). A linear regression showed that the interaction between eHEALS and NFC was not a significant predictor of health information seeking behavior (p = .792). Thus, Research Question 3 was not supported.
Research Question 4 asked, “Does eHealth literacy contribute to healthy behaviors?” in the areas identified by the CDC as crucial for college students, including substance abuse, sleep, vaccination, sexual health, diet, and mental health. To answer this question, a composite term Healthiness was created by taking the mean of each of the areas of substance abuse, sleep, vaccination, sexual health, diet, and mental health. The mean of Healthiness was M = 3.66, SD = 0.53. For R1, a linear regression was run with eHEALS as the dependent variable and the predictors Age, Gender, and Healthiness composite. With all components in the model, a positive relationship was found (r = .201, p = .001). Table 4 shows the full model. Indeed, when looking at the full model, after controlling for Age and Gender, Healthiness contributed 21.3% of the variance in the model, and was significant at p = .0001. Based on these results, we have evidence that suggests that eHealth literacy may contribute to healthy behaviors. However, because this was a preliminary question, we recommend further studies examine the relationship with these constructs in much greater depth.
Regression Model of eHealth Literacy on Healthiness.

p < .001. p < .0001.
Discussion
The first research question asked if high NFC individuals would have been more likely to seek out health information online than those who do not. Although support for this research question was not found, demographic factors should be considered. It may be that this particular population have not been as active, given that they are a younger demographic and may not have had as many experiences to necessitate time spent seeking out this health information. A recent report from the Pew Internet and American Life Project (2010) found that the “millennial” generation—today’s teens and young adults in their twenties—are split among their health information seeking online. According to that report, 31% of ages 12-17 receive health or physical fitness information on the Internet, but groups above the age of 17 are more likely to begin to use the Internet for health information. In fact, according to the Pew Internet and American Life Project, 72% of adults aged 18-29 look for health information online, although it is unclear how that breakdown occurs in that age range. Given that the average age of participants in the current study is 20.48, it may be that at this point in their lives, it is simply too soon to tell whether such a difference exists. It may also be that as a college demographic, health issues may not have been as salient for this population. Finally, this population may not have been the most generalizable group because participants were undergraduates. At the same time, it is curious that high scoring eHEALS individuals were more likely to have sought out health information online. It may be that there is a greater connection with health self-efficacy and health information than there is with whether one is high or low in their need for cognition. As such, there remains a need to test eHEALS and health information seeking behaviors with other populations, including young adults.
Although Research Question 1 did not find a relationship between high NFC individuals and health information seeking behaviors, support for Research Question 1a suggests that individuals who are higher in eHEALS are more likely to seek out health information online. This is consistent with other research that has found a positive relationship between literacy skills and seeking out information (Kinengyere, 2007; Paek & Hove, 2012). As eHEALS items are focused on perceived ability to use Internet resources, this makes sense. Findings from Research Question 1a suggest a need to examine the role of health self-efficacy and information seeking behaviors among different demographics. It also suggests the role of enhancing self-efficacy in online health interventions, as individuals with higher self-efficacy are more likely to seek out information on particular health issues. Similarly, the relationship between eHEALS and high NFC scores (Research Question 2) was found to be significant, which makes sense, given that both measures attempt to better understand individual characteristics in cognitive need and perceived capability.
When examining the role of NFC as a moderator between eHEALS and health information seeking behaviors, no relationship exists. While NFC was positively related to eHEALS and information seeking, it could be that it serves more of a predictive, rather than moderating role. Recent research examining the role of NFC as either a predictor or moderator in a smoking intervention found NFC did not moderate the role of a tailored intervention on actual smoking abstinence (Haug et al., 2010).
Results for Research Question 4 indicated that high levels of eHealth literacy do contribute to individuals engaging in healthy behaviors (e.g., physical activity), a finding supported by earlier work (Neuhauser & Kreps, 2010). This relationship could be causal in either direction: Individuals who have high eHealth literacy, by definition, are more able to understand healthy behaviors and their benefits, and thus engage in these behaviors more frequently. On the other hand, individuals who frequently participate in healthy behaviors might have the vocabulary, experiences, and motivation to help them discover and better understand health information online. Further work in this area can more closely evaluate this relationship.
Conclusion
This study examined the role of a relatively new but validated measure (eHEALS) that seems to be a relatively valid predictor of whether an individual has the capacity to engage with eHealth information sources. There are several limitations in the study, however. Firstly, while young adults were selected purposefully for the present study, various demographics should be examined in future research. This type of research should study mothers and fathers of young adults in college and compare their use of the Internet for health-information seeking behaviors, in addition to exploring how they themselves understand eHealth. Elderly adults should also be examined in terms of their ability to use the Internet for health information, whether they are successful in finding what they look for, and what their recommendations are for improvement, which would be helpful in understanding web usability as well.
In addition, while this research suggests that eHEALS could be a potentially better measure of efficacy rather than literacy, it did not directly study the role of self-efficacy on electronic health information seeking behaviors. Future research should seek to study the eHEALS measure more closely with traditional efficacy research.
This study had mixed results with regard to the role of NFC and eHEALS. The results from this study point toward a need to develop intervention materials when conducting eHEALS research and more closely examine how NFC operates within that frame. For instance, a prime way to develop an intervention would be one on making decisions about getting the HPV vaccine. That would include providing priming materials, which could be in print or another media, and contain statements that are gain or loss framed with regard to getting the vaccine (Rothman, Martino, Bedell, Detweiler, & Salovey, 1999). Gain-framed messages seem to positively influence preventive health behavior (Witting, Boere-Boonekamp, Fleuren, Sakkers, & Ijzerman, 2012). The way an individual high in NFC interprets those types of messages could lend critical insight into the factors that contribute toward getting the vaccine—and even more so on a theoretical level.
Multiple avenues for further research exist based on these results. A replication of the study with a broad demographic may give information as to whether demographics were a factor with the lack of support for NFC. It may also be that highly cognitive individuals may be more motivated to seek out health information online, but that NFC simply is not the best measure to capture that information. Further research should continue to assess, quantitatively and qualitatively, the need for cognition, along with emerging measures on health literacy and self-efficacy, to better understand such behaviors.
Finally, need for cognition states that high cognitive misers are more likely to engage in thought-provoking acts, whereas low cognitive misers are less likely to think in-depth. The theory behind eHEALS (Norman & Skinner, 2007) is that it purports that electronic health literacy comprises assessing comfort and skill in using information technology for health. For instance, in a clinical environment, eHEALS can potentially serve as a way to identify those who may or may not benefit from eHealth resources and interventions. But to better assess this outcome, eHEALS should be connected to need for cognition because its items focus on patient efficacy, rather than traditional literacy skills. Indeed, to a lesser extent, eHEALS is a tool for usability testing of a given health web site or technical interface based on the self-efficacy of a patient. Considering the need for high or low thought should be included in this framework because it can directly affect the way users interact with a health web site based on its messages, images, and multimedia content. Interventions that subsequently connect eHEALS to cognitive thought not only makes it more valuable from a usability perspective, but for better assessing the user.
The implicit connection between eHEALS and NFC has implications for future interventions on eHealth in terms of literacy, efficacy, and message strategy. Indeed, NFC has shown to moderate the processing of health information (Williams-Piehota, Schneider, Pizarro, Mowad, & Salovey, 2003), because the meaning behind that information is processed in different ways. For instance, findings from Williams-Piehota et al. (2003) show that messages tailored to high or low NFC individuals tended to be better at persuading mammography screening. With the increasing growth in Web 2.0 strategies that encourage tailored, individual messages, it makes sense that eHEALS should be administered with NFC in research and intervention strategies.
Footnotes
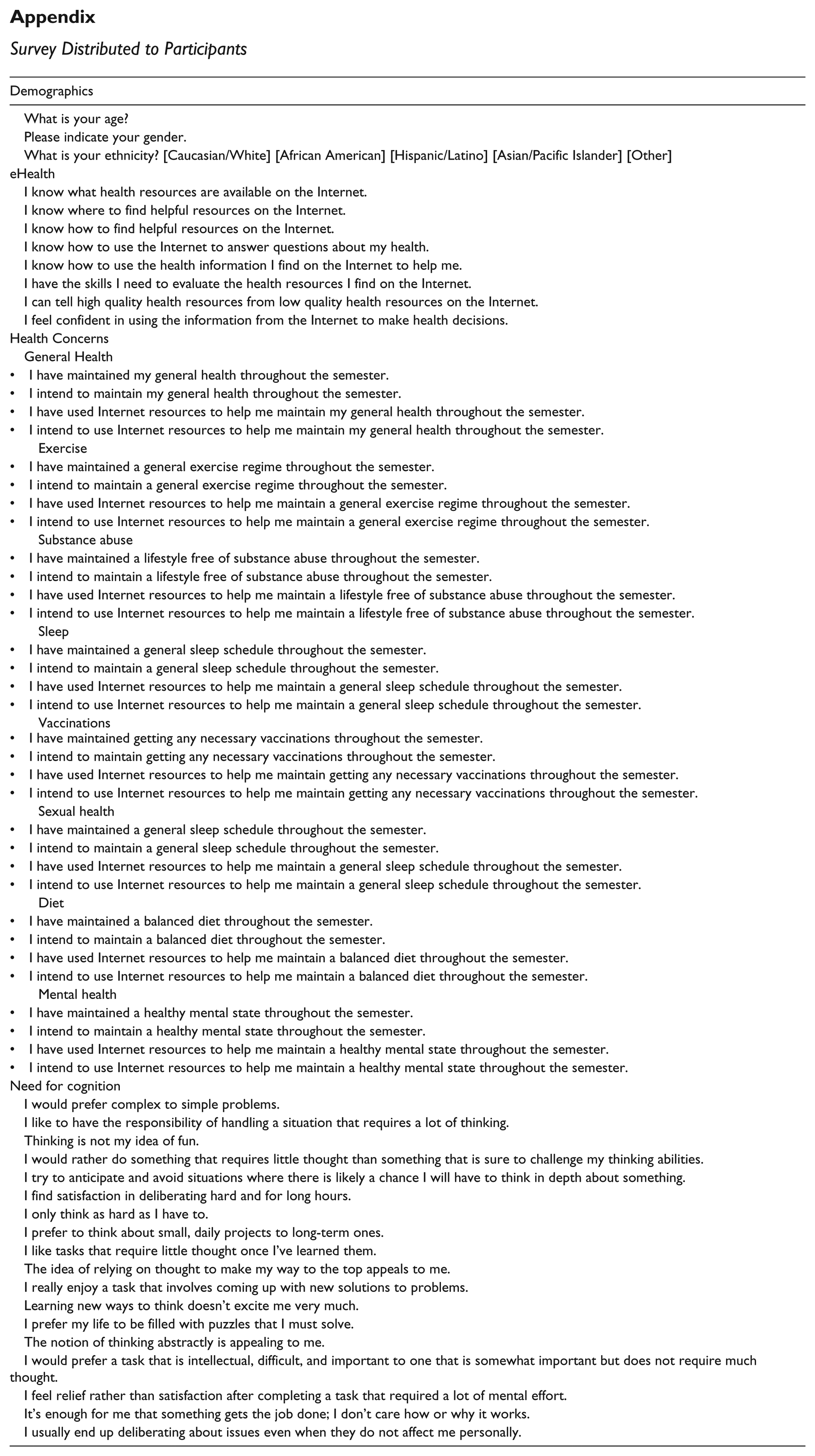
Appendix
Survey Distributed to Participants
| Demographics |
|---|
| What is your age? |
| Please indicate your gender. |
| What is your ethnicity? [Caucasian/White] [African American] [Hispanic/Latino] [Asian/Pacific Islander] [Other] |
| eHealth |
| I know what health resources are available on the Internet. |
| I know where to find helpful resources on the Internet. |
| I know how to find helpful resources on the Internet. |
| I know how to use the Internet to answer questions about my health. |
| I know how to use the health information I find on the Internet to help me. |
| I have the skills I need to evaluate the health resources I find on the Internet. |
| I can tell high quality health resources from low quality health resources on the Internet. |
| I feel confident in using the information from the Internet to make health decisions. |
| Health Concerns |
| General Health |
| • I have maintained my general health throughout the semester. |
| • I intend to maintain my general health throughout the semester. |
| • I have used Internet resources to help me maintain my general health throughout the semester. |
| • I intend to use Internet resources to help me maintain my general health throughout the semester. |
| Exercise |
| • I have maintained a general exercise regime throughout the semester. |
| • I intend to maintain a general exercise regime throughout the semester. |
| • I have used Internet resources to help me maintain a general exercise regime throughout the semester. |
| • I intend to use Internet resources to help me maintain a general exercise regime throughout the semester. |
| Substance abuse |
| • I have maintained a lifestyle free of substance abuse throughout the semester. |
| • I intend to maintain a lifestyle free of substance abuse throughout the semester. |
| • I have used Internet resources to help me maintain a lifestyle free of substance abuse throughout the semester. |
| • I intend to use Internet resources to help me maintain a lifestyle free of substance abuse throughout the semester. |
| Sleep |
| • I have maintained a general sleep schedule throughout the semester. |
| • I intend to maintain a general sleep schedule throughout the semester. |
| • I have used Internet resources to help me maintain a general sleep schedule throughout the semester. |
| • I intend to use Internet resources to help me maintain a general sleep schedule throughout the semester. |
| Vaccinations |
| • I have maintained getting any necessary vaccinations throughout the semester. |
| • I intend to maintain getting any necessary vaccinations throughout the semester. |
| • I have used Internet resources to help me maintain getting any necessary vaccinations throughout the semester. |
| • I intend to use Internet resources to help me maintain getting any necessary vaccinations throughout the semester. |
| Sexual health |
| • I have maintained a general sleep schedule throughout the semester. |
| • I intend to maintain a general sleep schedule throughout the semester. |
| • I have used Internet resources to help me maintain a general sleep schedule throughout the semester. |
| • I intend to use Internet resources to help me maintain a general sleep schedule throughout the semester. |
| Diet |
| • I have maintained a balanced diet throughout the semester. |
| • I intend to maintain a balanced diet throughout the semester. |
| • I have used Internet resources to help me maintain a balanced diet throughout the semester. |
| • I intend to use Internet resources to help me maintain a balanced diet throughout the semester. |
| Mental health |
| • I have maintained a healthy mental state throughout the semester. |
| • I intend to maintain a healthy mental state throughout the semester. |
| • I have used Internet resources to help me maintain a healthy mental state throughout the semester. |
| • I intend to use Internet resources to help me maintain a healthy mental state throughout the semester. |
| Need for cognition |
| I would prefer complex to simple problems. |
| I like to have the responsibility of handling a situation that requires a lot of thinking. |
| Thinking is not my idea of fun. |
| I would rather do something that requires little thought than something that is sure to challenge my thinking abilities. |
| I try to anticipate and avoid situations where there is likely a chance I will have to think in depth about something. |
| I find satisfaction in deliberating hard and for long hours. |
| I only think as hard as I have to. |
| I prefer to think about small, daily projects to long-term ones. |
| I like tasks that require little thought once I’ve learned them. |
| The idea of relying on thought to make my way to the top appeals to me. |
| I really enjoy a task that involves coming up with new solutions to problems. |
| Learning new ways to think doesn’t excite me very much. |
| I prefer my life to be filled with puzzles that I must solve. |
| The notion of thinking abstractly is appealing to me. |
| I would prefer a task that is intellectual, difficult, and important to one that is somewhat important but does not require much thought. |
| I feel relief rather than satisfaction after completing a task that required a lot of mental effort. |
| It’s enough for me that something gets the job done; I don’t care how or why it works. |
| I usually end up deliberating about issues even when they do not affect me personally. |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.