
Abstract
The Social Compass Curriculum (SCC) was investigated for its effectiveness in improving core social skills in three descriptive case studies of students with autism. Treatment fidelity of the SCC was also measured in the school setting. The Social Responsiveness Scale and the Autism Social Skills Profile were completed by parents to measure pre- and postintervention social skills for three students aged 8 to 11 years who participated in the present multisite pilot study. Fidelity of implementation data were collected via a checklist during observations for three educators who implemented the intervention. Results indicate that the SCC improved core social deficits based on standardized rating scales measures. Fidelity observations revealed that 83% of teaching components were completed correctly after 3 hr of training. The results of this study aligned with the National Autism Center’s call for ongoing research of school-based interventions and school-friendly interventions for people with autism spectrum disorders (ASD).
Keywords
The characteristics of autism spectrum disorders (ASD) are well documented and difficulties in social interaction are a core facet of ASD (American Psychiatric Association [APA], 2000). Although the definition of social skills is not undisputed in the autism community, its description typically encompasses perspective taking, joint attention, social pragmatics, social reciprocity, linguistic conventions, and appropriate emotional affect. Social deficits in ASD have significant consequences; people with ASD tend to be isolated in social environments, especially in a mainstreamed school setting (Rao, Beidel, & Murray, 2008; Sansosti, 2010, White, Keonig, & Scahill, 2007). Social isolation, particularly for adolescents, has been implicated as a possible cause for secondary manifestations of psychiatric illness in individuals with ASD later in life (Hurtig et al., 2009; White et al., 2007). Research suggests that the lack of social involvement for youth with ASD leads to serious long-term mental health consequences that exasperate social deficits. During school years, these students may frustrate their teacher’s ability to manage a classroom of students with mixed abilities, which can lead to the individual with ASD being moved into more restrictive environments where positive social models may not exist. The current special educational paradigm involves the adherence to full inclusion for all students to the highest degree possible. Students with autism can pose unique challenges to a classroom teacher especially due to behaviors resulting from a lack of social competence. They do not learn social skills incidentally or vicariously in the same manner as their nondisabled peers, or even persons with other disabilities (Volkmar, 1993). As such, these students often behave in a manner, which may draw negative attention from others or cause avoidance by neurotypical peers. In addition, they may find others unpredictable and therefore difficult to interact with due to their failure to follow rigid routines or structures utilized by the person with ASD. The crux for the classroom teacher is to create a learning environment that will work for all students and avoids crisis management due to problem behaviors. In other words, educators need to reduce the potential for challenging behaviors before they arise rather than focus on contingency plans for managing behaviors once they occur (Marks et al., 2003). Based on the fact that poorly formed social skills is a common attribute across the spectrum of autism disorders, directly teaching social skills is a proactive strategy teachers may use to effectively manage their classrooms. Time is probably a teacher’s most precious commodity. Therefore, a social skills program used by teachers needs to be easy to implement, adaptable to unique student characteristics, and effective. Individuals with ASD are most likely to be receptive to social skills programs that consist of routine structures, provide alternate modes of completing assignments, use visual cues, provide mnemonic devices, and nonverbal cues (Marks et al., 2003). Programs that are provided to a whole class of students assist in creating a common language in the classroom for social behaviors, helping all students understand components of positive social interactions. This may help facilitate positive interactions between people with ASD and other students. In addition, Sansosti, in a guide for school-based professionals, states, . . . to be most effective, school-based efforts aimed at enhancing the social skill development of individuals with ASD should be conducted by using a systematic approach. That is, social skill interventions should focus on a combination of school-wide, small group, and individualized supports. (Sansosti, 2010, p. 259)
Current social skills interventions approach the problem from an environmental standpoint as well as intra-individually. Environmental interventions aim to alter the setting by working with other students and creating a physical environment that facilitates social interactions. These include The Circle of Friends Program (Frederickson & Turner, 2003) and Peer Buddies (Roeyers, 1996), which work with typically developed students to form facilitated friendships between students with ASD and neurotypical peers. These interventions have positive anecdotal effects for all young people involved (National Autism Center, 2009). However, the positive impact of these environmental interventions does not continue when a person with ASD leaves his or her school site or reaches adulthood. Orsmond, Krauss, and Seltzer (2004) reviewed social relationships among adults with autism and found that nearly 50% of the adults with ASD reported no social interactions outside prearranged group activities. Moreover, the same study found that reciprocal friendships existed for only 8% of adults with ASD when prearranged social outings were not provided. These findings corroborated the low rate of friendships reported in other studies and helped reveal the unfortunate fate for many people with ASD who age-out of school and lose facilitated social interactions. The absence of structured friendships for these adults explains the profound loneliness and isolation leading to the onset of psychiatric behavioral problems that may further restrict access to community life (Ghaziuddin, Ghaziuddin, & Greden, 2002). As Ghaziuddin et al. (2002) detail, social isolation and resultant psychiatric behavior problems further diminish a person with ASD’s ability to engage in the community at large, thus creating an immeasurable fissure between sound mental health and mental illness. This means that young people with autism need to learn skills rather than depend fully on changes to their environment.
There is a shortage of evidence-based social skills curricula available to teachers of students with ASD, while at the same time educators are experiencing the striking rise in the occurrence of children with autism. The current estimate for autism prevalence is 1 in 88 for all children and 1 in 54 for male children (Centers for Disease Control and Prevention [CDC], 2013), which is up from a rate of 5 cases per 10,000 individuals approximately 10 years ago (APA, 2000). Individuals with ASD are no longer rare in classrooms and their needs are painfully obvious to any educator. The National Autism Center’s large-scale project, National Standards Project, seeks to objectively articulate evidence-based thematic intervention approaches for ASD rather than endorse particular curriculums or programs. This project calls for the use of established and emerging interventions for people with ASD and for educators to conduct scientifically meaningful research to further establish interventions for this population. Krasny, Williams, Provencal, and Ozonoff (2003) argue that fundamental skills needed are: nonverbal skills, emotional awareness, conversation skills, and social problem solving. The Social Compass Curriculum is a story-based intervention; as such it uses an instructional methodology cited among the established practices according to the National Standards report (National Autism Center, 2009). Furthermore, the SCC intervention meets the need for schools to be the place where the majority of intervention occurs for young people with ASD. The SCC was initiated in the schools after collaboration with educators, parents, and specialists; the first edition of the SCC was implemented in 2002. The SCC has its foundation in a story-based intervention that focuses on four key areas: Nonverbal Communication, Emotions, “We” Skills, and Social Problem Solving. Each lesson consists of a story relating a particular social problem, a visual aid, facilitator modeling of successful behavior to remedy the social problem, student role-playing, student self-reflection, and a letter to the home to enhance generalization of learned skills. In 2011, a poster was presented at the California Association of School Psychologists presenting data reflecting that educators found the SCC very effective for teaching social skills to students with autism within a school setting (Boyd, McClelland, & Flowers, 2011). These findings were based on an online anonymous, nine-item Likert-type scale, wherein 100 educators who attended a training on the SCC were invited to respond. These educators worked within one suburban Special Education Local Plan Area (SELPA) including elementary, middle, high school, and adult transition grade levels. Of the 100 educators invited to participate in the survey, 18 responded. The highest percentage of respondents represented educators who work with students whose disabilities range from mild to moderate and whose educational placement was in special day class. The majority of the students were reported to function within the first to sixth grade level. Sixty percent of respondents reported that they were able to implement the SCC in their classrooms “pretty well” which was reported via the following scale: 1 = not well, 2 = somewhat well, 3 = pretty well, 4 = very well. Due to anonymity of the survey, the researchers were not able to determine the number of hours of training the educators had prior to implementation. The results may be biased toward individuals who had positive relationships with the creators of this curriculum and thus took the time to respond to the survey. However, this preliminary data suggest that students who function between the first and sixth grade levels were able to access the curriculum in a school setting, while the actual grade level of the students is unknown. Based on preliminary data, it appears that students who function at the elementary grade levels can benefit from the SCC and that their teachers found they could use the SCC “pretty well” in a school setting (Boyd et al., 2011).
The current research aims to answer two research questions:
In the present study, fidelity was measured via direct observation by the trainer using a checklist to describe how well teachers are able to follow the structure of the SCC in a typical school setting. Fidelity is an important component of ASD intervention research since it ensures that the intervention was implemented as prescribed and allows the practitioner to estimate how applicable a particular intervention will be in a typical classroom environment (Sansosti, 2010).
Method
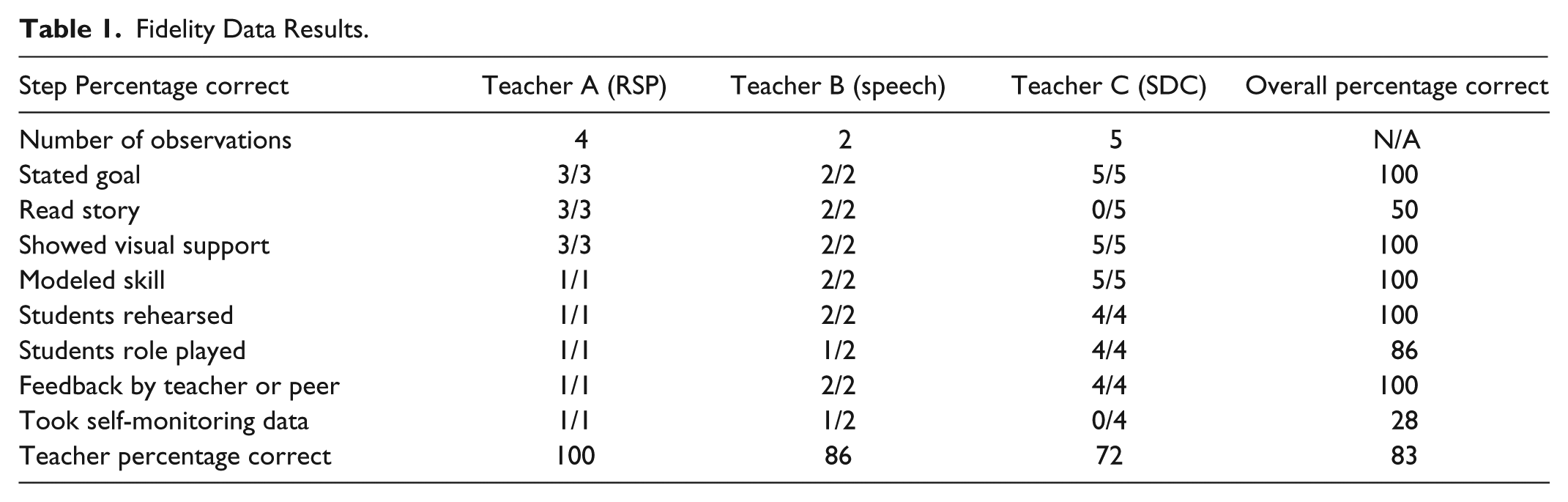
The present study utilized a descriptive case studies design for analysis of student social skills development in three students with ASD. Two public school sites were invited to participate, representing two different educator facilitators. The SCC trainer conducted fidelity of implementation observations across the implementation of the intervention phase of the study. See Table 1.
Fidelity Data Results.
Experimental Intervention
The independent variable for this study was the Social Compass Curriculum: A Story-Based Intervention Package for Students with Autism Spectrum Disorders (Boyd, McReynolds, & Chanin, 2013). It follows recommendations put forth by Krasny et al. (2003), “fundamentals . . . such as nonverbal communication and affect recognition need to be practiced in a group setting” (p. 108). Areas of social skills that are addressed in the 24-lesson curriculum include: Nonverbal Skills, Emotions, “We” Skills, and Social Problem Solving. Each lesson incorporates the comprehensive components outlined by Krasny et al. (2003) and Marks et al. (2003) such as: defined goals, visual supports, a narrative of a social challenge, teacher modeling, rehearsal, role-play, feedback, reinforcement via self-monitoring, and a take-home letter to encourage generalization of skills. All instructional components of the SCC lessons encompass skills that a classroom teacher or service provider already has in his or her collection of classroom techniques. Each SCC lesson can be completed in approximately 40 min with a group of students. The 8 lessons of the SCC lessons were presented to groups of students within a pull out social skills group. The intervention was delivered by California credentialed educators who received 3 hr of training prior to and brief consultation during the intervention.
Ethics Statement
Informed consent was obtained from minor students’ parents for student participation in a school-based social skills curriculum, collection of survey data, and presentation of data in the form of a research paper. Consent to conduct research at school sites was approved by a committee of administrators representing the various school districts, the Special Education Local Plan Area administrators, and the governing cabinet for individual school districts. Students were given the opportunity to assent to the intervention as well as to voluntarily withdraw from the intervention. No financial offering or gifts were provided to the parents of the students or to the students for participation. The educator participants were provided a free SCC manual that they were allowed to keep.
Participants
The focus of this investigation was on students with ASD who were provided intervention with the SCC. The three students evaluated had educational designations of Autistic-Like Behaviors determined by school personnel. The participants aged from 8 to 11 years attended one of two public elementary schools in a suburban area of Southern California experienced the SCC intervention. Demographics of three students studied with ASD consisted of two male students and one female student. All three students attend public elementary school in a fully included general education environment without the assistance of an adult aide. All students are able to access grade-level academics independently. The three students would be described as individuals with high functioning autism based on their ability to access grade-level general education academics. However, these students showed social impairments with T-scores about 76 on the Social Responsiveness Scale (SRS). The three students studied were provided the SCC intervention as a pull out designated service per their individualized education program. See Table 2.
Participant Demographics.

Three public educators were observed to measure fidelity of treatment. Two were California credentialed special education teachers and one was a California licensed speech and language pathologist. See Table 3.
Teacher Demographics.

Procedures
The first month of the study, teachers attended a 3-hr training using a PowerPoint that described the research components’ rationale and corresponding strategy present in each lesson. Each of the five steps to a lesson was described in detail with several examples provided from the text. The original of the visual supports and how to give feedback was role-played with the participants. At the onset and conclusion of the study, social skills rating scales were provided to parents or guardians of students with designated ASD.
Next, the social skill groups were assembled. Male A participated with Teacher B (speech) in a mixed group of four students who were pulled out of their general education placement for designated speech services in one public elementary school. Male B and Female A participated with Teacher A (RSP) in a mixed group of five students who were pulled out of their general education placement in the second public elementary school.
During the intervention phase, the SCC trainer measured fidelity of the intervention using a data collection system composed of a checklist. The trainer observed the entire lesson and checked off the presence or absence of each step of the lesson listed in Table 1. Targeted observations were scheduled once every 1 to 2 weeks to achieve an adequate measure for treatment integrity, 10 of 33 sessions were observed. See Table 4.
Weekly Timeline of Research Activities.

Indicates trainer-observed session and collected fidelity of implementation data.
Indicates Male B absent.
At each observation, data were collected on the educators’ implementation of the comprehensive components of each lesson. Total observations may have included parts of a single lesson as Teacher A and B provided intervention twice a week for 20 min and Teacher C met once a week for 45 min. Teacher A and B used small pull-out groups and Teacher C worked with the whole class of students in a special day class (SDC) with moderate disabilities. The SDC teacher modified the curriculum by summarizing the social narrative and replacing the self-monitoring with whole group feedback as the students’ attention to these aspects was poor. The SDC teacher found it useful to use two sessions per lesson for whole class instruction.
Social Skills Measures
Most rating scales are given at the beginning of a study and can be used for follow-up measures (Sansosti, 2010). Two rating scales were chosen to be completed by parents for this study. The SRS as it is believed to have the potential to be sensitive to treatment changes in children with autism spectrum disorder (Sansosti 2010; White, 2007) as well as the ASSP by Scott Bellini (Sansosti, 2010). The authors provide mean changes on social skills measures as well as qualitative case descriptions for the effect of the SCC for three students with ASD.
Social Responsiveness Scale
The Social Responsiveness Scale (SRS) is a 65-item rating scale based on a normative sample of 1,600 children from 4 years to 18 years of age. This rating scale prescribes to measure emotionally appropriate social interactions of individuals who may have ASD. According to Constantino et al. (2003), the SRS provides a .7 correlation with the Autism Diagnostic Interview–Revised and the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) in its ability to identify autism and a .8 interrater reliability. The SRS designates ASD by evaluating the individual’s social interactions without regard for intellectual capacity. This scale is described as appropriate for research pursuits due to its brief administration, approximately 15 min, and its linkage to current theories. It is designed to be completed by an adult, a teacher, or parent. Subscales on the SRS include social awareness, social cognition, social communication, social motivation, and autistic mannerisms.
The SRS was selected for its ability to quickly identify aspects of social skills present before and after the SCC intervention and for confirmation of identified participant ASD status. The SRS was sent to the participant’s parent via the SCC facilitator. The parent independently completed the rating scale as a survey without the assistance of the facilitator or the researcher. The researcher scored the rating scale according to the manual and analyzed the scores at the overall level, domain level, and item level.
Autism Social Skills Profile
The Autism Social Skills Profile (ASSP) is a scale developed to measure social functioning in individuals with ASD and specifically to facilitate progress monitoring through an intervention process. The preliminary psychometric analysis was conducted with mothers representing 93% of respondents, then fathers (3%), grandparents at 2% and other as last 2% (Bellini & Hopf, 2007).The ASSP ascribes to measure three domains: social reciprocity, social participation/avoidance, and detrimental social behaviors. The ASSP utilizes a 4-point Likert-type scale for each of the 49 items and can be completed by parents or teachers in approximately 15 to 20 minutes. Bellini and Hopf (2007) analyzed the psychometric properties of the ASSP finding the internal consistency (Cronbach’s α) to range from α = .848 to α = .940 depending on the sample. Test–retest reliability was .904 for the entire sample and factor loading was low (.09 to .36) suggesting the measure identifies distinct factors. The ASSP was sent home to the participant’s parent by the SCC facilitator; the parent independently completed the rating scale as a survey without the assistance of the facilitator or the researcher. The ASSP was scored using instructions provided by the authors and was analyzed at the overall, domain, and item level.
The tool was designed to monitor progress on social skill interventions for students with autism. Bellini and Hopf (2007) reported parents of students with intellectual disability scores between 67 and 161, students with autism scored between 67 and 177, and students identified as high functioning autism scored between 70 and 177. Bellini and Hopf (2007) reported the mean score for high functioning students with autism as 109.83. A group if individuals with intellectual disabilities or severe language deficits had a mean score of at 97.12. This instrument did not provide cutoff scores but rather ranges of scores related to severity of impairment.
Results
Fidelity data collected by the SCC trainer is displayed in Table 1. Key components of the intervention were monitored while the teacher implemented the SCC with a mixed group of students. All Teachers successfully stated the goal of the lesson. Teacher A (RSP) and Teacher B (Speech) read the social narrative aloud at each observation point. Teacher C (SDC) did not read the short story aloud straight through from beginning to end when the observer was present. Instead this teacher adapted the story to address the student’s attention span and unique needs using gestures to act out story as she went along. All teachers modeled skills, allowed for student rehearsal, and provided feedback to students. Student self monitoring was an area of difficulty; Teacher B (speech) was observed as presenting the self monitoring aspect of the SCC half of the time and Teacher C (SDC) did not implement the student self monitoring component of the lessons when observed by the trainer. The self-monitoring component of the Social Compass Curriculum was the biggest challenge to all three groups and required teachers to prompt students to complete the self-monitoring tasks. To teach students to self-monitor, the teacher is expected to provide prompting initially and continue until students are independent and accurate with the task. Without therapist coaching provided and after fidelity observations, teachers reported they would be likely to stop implementing this step. Overall Teacher A (RSP) implemented the SCC with 100% fidelity. Teacher B (speech) implemented the SCC with 86% fidelity. Teacher C (SDC) implemented the SCC with 72% fidelity.
Social Skills Measures
Social Responsiveness Scale
Two of three participants with ASD returned the pre- and post-tests for the Social Responsiveness Scale (SRS) fully completed; one participant (Female A) returned a partially completed posttest rating scale. The SRS generates T-scores with a mean of 50 and a standard deviation of 10 based on a normative sample of 1600 individuals. A T-score of T-59 or below suggests normal range; T-60 to T-75 indicates mild to moderate range; and T-76 or higher represents severe range
All participants for pre- and post-tests had T-scores in the severe range and corroborates the identification of participant ASD. A comparison of pretest and posttest total scores for the SRS shows that the post-test yielded an average T-85 versus an average pre-test of T-89 with a −4.49 mean percent change. The standard error of measure (SEM) on the SRS is 2.4 for male children and 2.6 for female children. The numeric difference of T-scores from pre- to post-test for individual students as well as the average T-score numeric difference was greater than the SEM for the testing instrument, which suggests that the changes in T-scores were greater than the degree of natural fluctuation in the instrument’s sensitivity. See Table 5.
SRS Total Score T-Score Results.

Incomplete rating scale.
Item level Analysis for Participants—SRS
Parental rating of participants’ pre- and post-intervention were evaluated at the item level to provide progress monitoring data. The SRS rating scale employs the following Likert-type scale: 1 = not true, 2 = sometimes true, 3 = often true, 4 = almost always true. Items that directly relate to social functioning were reviewed and areas of change are reported below for each single case studied. See Table 6.
Male A—Item Responses SRS Pre and Post.

Male A had the greatest number of socially related items on the SRS that improved. At the same time this individual student also had a T-score of 90+ at baseline. He improved in multiple aspects of social communication such as making eye contact and matching his facial expressions with what he is communicating. Male A, according to parental observations, improved his tendency to interact with other people as indicated by SRS prompts: does not join activities unless told to do so, appears to avoid starting social interactions with peers or adults, and has difficulty making friends, even when trying his best. See Table 7.
Male B Item Responses SRS Pre and Post.

Male B improved on four items related to social skills. His parent’s responses on the SRS indicated improvement in the area of understanding that others have feelings or thinking, a measure of perspective taking. He was noted as being able to imitate the actions of others more often after the SCC intervention and was noted as offering comfort to others when sad to a greater degree after the intervention. Male B was observed as thinking and talking about the same thing, which may describe rigid interests, to a lesser degree after the SCC intervention.
Female A improved on six items of the SRS that relate to social competency. Female A’s parent reported improvements in her ability to take turns during social interactions, maintaining eye contact, and offering comfort to others when sad. Her parent also reported that she plays appropriately with children her age to a greater degree and is less likely to be regarded as odd or weird by other children. Lastly, Female A’s parent noted that she was not observed as taking things too literally without gaining the real meaning in conversations as often as before the intervention with the SCC. See Table 8.
Female A Item Responses SRS Pre and Post.
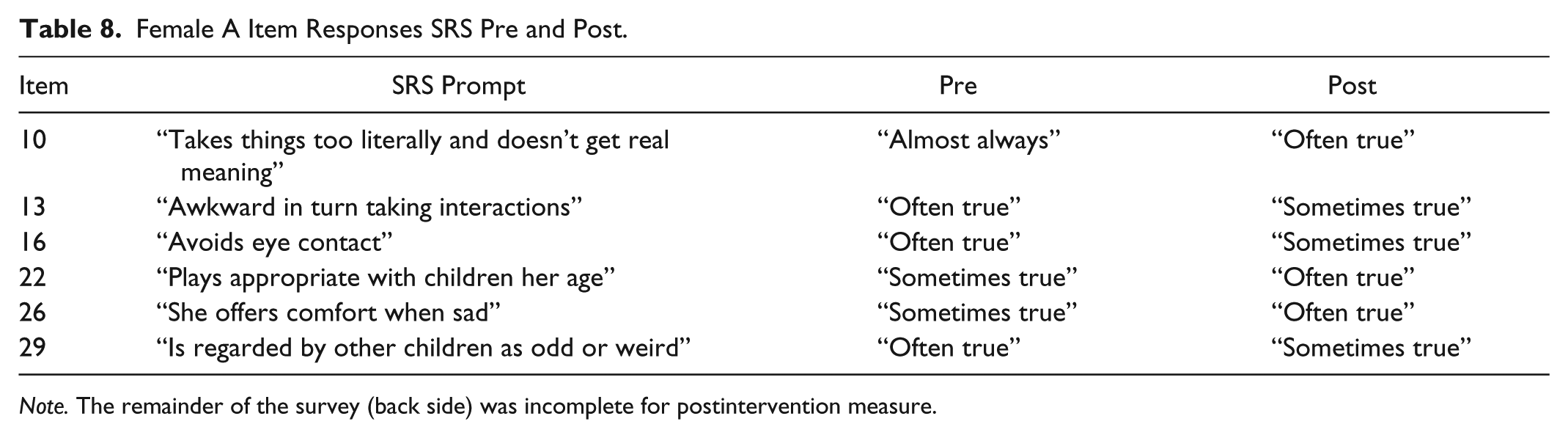
Note. The remainder of the survey (back side) was incomplete for postintervention measure.
Autism Social Skills Profile
Of the three participants with ASD, three parents/guardians completed the pre- and posttest measures for the ASSP scale. At the time the ASSP post-test was completed, the students had completed 8 to 9 of the 24 lessons included in the intervention. The study began in January, sessions began in March, sessions ended in early June and post intervention was collected in June before the school year concluded. The ASSP was reported as being appropriate for monitoring of progress for social skills interventions; higher total scores for social functioning represents more positive social behaviors (Bellini & Hopf, 2007). All students’ total scores for social functioning increased. The range of percent increase was 3.96% to 32.94%. When scores were averaged for the group, 16% change was noted.
Item Analysis Pre–Post for single Participants
The ASSP Provides the respondent with the following Likert-type scale: 1 = never, 2 = sometimes, 3 = often, 4 = very often. Areas of improvement are provided in the following tables based on parental responses pre- and post-intervention (in this case post refers to approximately 8 to 9 of the 24 lessons).
Male A improved on seven items of the ASSP that related to social competence. His parent reported improvements in his ability to interact with peers in structured and unstructured activities. He was reported as being able to verbally express how he was feeling to a greater extent than before the SCC intervention. Male A was reported as having positive experiences with peers often and joining activities with peers. See Table 9.
ASSP Male A—Item Responses ASSP Pre and Post.

Indicates items that were also improved on another participant’s item analysis.
Male B improved, according to his parent respondent, in his ability to interact with peers during unstructured activities and allowing peers to join in activities. He was reported as engaging in solitary interests or hobbies less often which seems to account for the aforementioned report of engaging with others more often. He was noted as being less likely to misinterpret the intentions of others as well as being less likely to end conversations abruptly. See Table 10.
Male B—Item Responses ASSP Pre and Post.

Indicates an item that was also improved on another participant’s item analysis.
Female A improved on three items on the ASSP that relate to social competency by her parent. From baseline to the post-measure, Female A was more likely to interact with peers in structured and unstructured activities. She was also reported to interact with groups of peers more often than prior to the SCC intervention. See Table 11.
Female A—Item Responses ASSP Pre and Post.

Indicates items that were also improved on another participant’s item analysis.
Discussion
The results of this study at least partially answer the research question as to whether parents of individuals studied with ASD would note improvements in core social skills. Combined parental pre- and post-measures using the ASSP showed that indicators of social reciprocity by querying aspects of social exchange, such as maintaining the “give and take” of conversations, responding to questions directed at him or her, taking turns during a game, acknowledging others’ interests, and joining a conversation without interrupting (Bellini & Hopf, 2007, p. 85) improved from the baseline after approximately eight to nine lessons through the 6-month period of the case studies on the SCC intervention. Comparison of averaged pre- and posttest results revealed an increase in social functioning of 16% change, with an average pretest score of 100 and an average posttest score of 116. When individual items were analyzed for the three students with ASD, there was an overlap in parental perception of improvement for interacting with peers in unstructured activities for all three students. The fact that all three parents observed their child interacting with others during unstructured activities is a major gain for these youths as unplanned interactions with peers is known to be an aspect of social interaction that is particularly difficult for people with autism who often seek interactions that are controlled by adults (Orsmond et al., 2004). The SCC includes multiple lessons that directly teach individuals the mechanics of social interactions; moreover, the use of peer role-plays integrates a range of interpretations by students in which the student with ASD can observe and learn appropriate responses.
The Social Responsiveness Scale (SRS) supports outcome analysis of emotionally appropriate social interactions of people with ASD. The SRS has an additional function of assisting in the identification of people with ASD. In this regard, the SRS provided a dual purpose: first, to measure differences in congruency of emotional response to social interactions pre and post, and second, to confirm that participants noted in the study as having ASD were correctly identified. The SRS provides T-score designations of functional level; a T-score of 59 or below is considered normal range, T-60 to T-75 relates to mild to moderate range, and T-76 or greater indicates severe range. All participants exhibited T-scores greater than 76, indicating a high probability of ASD. T-scores for all participants decreased after exposure to the SCC intervention. The average percentage change was −4.49 with an average difference of 4 for T-score results. All outcome measures were above the cutoff for standard error of measure, suggesting changes were greater than natural fluctuations in scores innate to the SRS. For the participants in this study, the item analysis of the SRS showed improvement in social skills as it relates to emotional appropriateness of the situation while participant T-scores remained within the severe range. This finding suggests that the pivotal skills of emotional awareness and social problem solving may have improved after exposure to the SCC.
When individual items were evaluated for the three students with ASD, there was overlap on two items between Male A and Female A and Male B and Female A. Items where there was shared improvement across participants were using more typical eye contact and offering comfort to others when sad. The SCC offers students the opportunity to practice effective conversational behaviors, which include facing one’s conversational partner and this repeated practice may have improved the children’s tendency to offer eye contact. Emotional understanding represents a unit of lessons in the SCC including identifying emotions based on facial expressions and discerning emotional intensity in others. Appropriate responses to other’s emotions are presented in a social narrative, modeled by the facilitator, role played by the student, and then considered by peer review as well as self-reflection. At face value it appears that the SCC would teach emotional understanding in such a way that improvements may be accepted as actual changes in the child with ASD’s understanding of how to interact with a person who is sad by offering comfort.
Specific topics covered during the course of the SCC intervention were reading body language, using proximity to communicate intent to communicate, using volume and tone of voice to communicate in expected fashion with peers, using social referencing to communicate intent to interact with group, and using appropriate intensity of emotions to match the emotional intensity of the social situation. Methods for teaching include providing an adult-generated model, imitating model (rehearsal), adult and peer feedback of correct and incorrect examples of behavior, student role-playing, allowing peer-mediated feedback, and last, student self-monitoring. In addition, each lesson included a parent send home letter to describe the content of the lesson and encourage parental praise of desired behaviors—a practice to encourage generalization and maintenance of learned behaviors. The inclusion of a parent letter describing the content of each lesson may have caused the parents to inflate their ratings on measures of social skills due to directing the parent’s attention to particular social skills. Although this practice may have inflated parental responses, this possibility is viewed as a positive attribute, because this would mean that the parents were attending to positive behaviors to a greater degree than prior to the SCC intervention. Praise of prosocial behaviors by parents would predict repetition of those behaviors by the children, assuming the children desire parental attention, and thus would possibly increase those behaviors in multiple environments which may influence generalization as well as maintenance of learned skills.
Previously presented research revealed that a group of 18 educators found that they were able to implement the SCC pretty well with limited training (Boyd et al., 2011). To be useful, an intervention benefits from a format that reduces interventionist’s vigilance (Koegel, Koegel, Harrower, & Carter, 1999a). A predictable routine in an intervention aligns with strengths of people with ASD in adhering to routines (Krasny et al., 2003; Marks et al., 2003). The SCC uses a common structure to each lesson while addressing new concepts, thus providing needed routines which lessen interventionist vigilance. For a teacher, this would likely improve fidelity as well as satisfaction with the SCC. Moreover, student motivation was noted by Krasny as being related to student perceived relevance of the instructed social skills, and was reported as being enhanced by story-based lessons (Krasny et al., 2003). Each SCC lesson includes a vignette of a particular social problem wherein the protagonist of the story solves his or her social problem. The SCC social narratives serve a dual purpose: to provide relevance to the skills taught as well as providing an explicit example of a social problem and how the problem can be solved.
The SCC is an intervention that educators were able to use with fidelity; educators reported that students could participate in it easily, and it stated teaching procedures clearly. This is especially important with regard to current political educational mandates that educators must apply differentiated teaching for individuals with ASD. For example, state mandates in California require special educators to obtain additional credentialing, an autism authorization, to teach students with autism. The need for school-friendly effective interventions are timely and of paramount importance.
The research presented in this study suggests that the Social Compass Curriculum melds current ASD instructional best practices with user-friendly intervention educators can easily use with a whole class or smaller groups of students.
According to Odom and others (2003) the APA, Division 12, reported on single-case research designs that were deemed well established or probably efficacious based on particular standards. Those single-case research designs that included N > 9, included well-designed experimental procedures, a treatment manual, fully described participants, and compared the treatment with another treatment or condition were deemed well established. Single case studies that included N > 3 and met the same criteria as noted earlier were described as probably efficacious. This research did not meet the standards for “probably efficacious” based on the APA’s criteria on multiple levels. Although a series of three case studies were presented and had some areas of common findings, the number was not greater than three. A treatment or intervention manual was available to the facilitators and did result in strong fidelity for the implementation of the SCC intervention for the students with ASD who were reported here, but the students’ single cases were not compared with another treatment or a control condition. The experimental design of pre- to post-test is not as strong as other single case designs such as ABA (baseline, intervention, removal of intervention) due to the nature of an intervention that includes learning which is impossible to remove once gained by the participants. Possible confounds to the findings in this study include possible inflation of parental responses due to knowledge of the content of lessons taught with the SCC as well as potential desire to report positive results due to parental relationships with the facilitators of SCC or the author of the SCC.
The gold standard of research, the fully randomized clinical trials as used in medical research, is far from the portrayal of data here, and it is well known that educational research often falls short of the ultimate goal (Odom et al., 2005). In an evaluation of research in special education, it was noted that special education research is particularly complex due to heterogeneity of participant characteristics and the continuum of educational placements which makes the creation of equivalent groups with large enough sample sizes very difficult to obtain or infeasible (Odom et al., 2005).
This study does provide preliminary data that helped determine which rating scales possessed the specificity needed to measure small changes after the SCC intervention; the Social Responsiveness Scale and the ASSP yielded changes pre- and post-intervention. Moreover, parental observations of improvement were noted in several items on the SRS and ASSP some of which overlapped which suggest that changes may have been due to more than chance. Face validity applies when one compares items wherein students behaviors changed align well with social skills directly taught during the SCC intervention.
Maintenance of social capacity is another area wherein the present study did not provide solid evidence and is thus a fertile area of research. In the future, a social rating scale could be provided to parents and teachers well after the SCC intervention occurred to determine whether participants maintained skills beyond the active intervention phase. At present, teachers need as many classroom-based social skills interventions as possible to address the unique needs of individuals with ASD, and small studies with preliminary results assist in meeting this need. The SCC does align well with recommended procedures indicated by the National Autism Center (2009). In addition, teachers who used the SCC reported that the intervention was easy to follow and that the intervention appeared to work well for students (Boyd et al., 2011).
Students who participated in the SCC were reported to engage in unstructured peer interactions to a higher degree based on parental observations after the SCC than before the intervention. It is suspected that if these youths with ASD continue this practice that social reinforcement will aid in these youths continuing this practice which may reduce the potential for future isolation known to occur in those people with ASD after school-aged activities cease (Orsmond et al., 2004).
The ultimate goal for full integration of individuals with ASD into the least restrictive environment is to provide a mechanism for all students to develop an understanding of personal differences and develop a way to successfully interact socially. It is believed that any social skills intervention that enhances this possibility is useful for students.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare the potential conflict of interest related to one of the author’s creation of the Social Compass Curriculum. No financial gain has been experienced and the curriculum has been made available to schools, for 10 years prior to publication, free of charge.
Funding
The author(s) received no financial support for the research and/or authorship of this article.