
Abstract
This article reviews inequalities in health risks and outcomes based on a large longitudinal cohort study of distance-learning adult students enrolled at Sukhothai Thammathirat Open University (n = 87,134). The study began in 2005 and the first follow-up was completed in 2009. Risks analyzed for health inequalities were divided into demographic, socioeconomic, geographical, behavioral, and environmental groups. Unequal risks and outcomes identified that would be amenable to policy interventions in transitional Thailand include the following: heat stress—contributing to many adverse outcomes, including occupational injury, psychological distress, and kidney disease; urbanization—unhealthy eating, sedentary lifestyles, low social capital, and poor mental health; obesity—increasingly common especially with rising income and age among men; and injury—big problem for young males and associated with excessive alcohol and dangerous transport. These substantial inequalities require attention from multisectoral policy makers to reduce the gaps and improve health of the Thai population.
Introduction
The study of social inequalities has become important in many fields of research including economics, sociology, political science, public health, and epidemiology. Health inequalities among population subgroups have been documented in public health literature for centuries. Two famous English examples are from the work of William Farr in the 1830s when he measured and reported large geographic variations in the risk of death by districts (Farr, 1839; Whitehead, 2000) and from Edwin Chadwick in the 1840s noting large variations in life expectancies by class and occupation (Chadwick, 1842; Golding, 2006).
The study of inequalities in health in recent years has not only measured the magnitude of inequality but has also identified characteristics of those most at risk within populations (Braveman, 1998; d’Uva et al., 2008; Huisman et al., 2005; Starfield, 2002). In 2008, as part of the report by the World Health Organization’s (WHO) Global Commission on Social Determinants of Health (CSDH), global health inequalities reached center stage. The CSDH shone a spotlight on the health of the poor around the world (CSDH, 2008; Friel et al., 2008; Marmot et al., 2008). Furthermore, it documented large social gradients in health within countries and substantial inequalities for health among countries. This report helped to set the global health agenda at the start of the 21st century.
Health inequalities are driven by social and political inequalities and the way in which these drivers play out varies greatly due to differing political, economic, social and cultural contexts. These contexts produce structural factors that connect the drivers and finally result in good or bad daily living conditions that are distributed unequally across the social hierarchy (Figure 1).
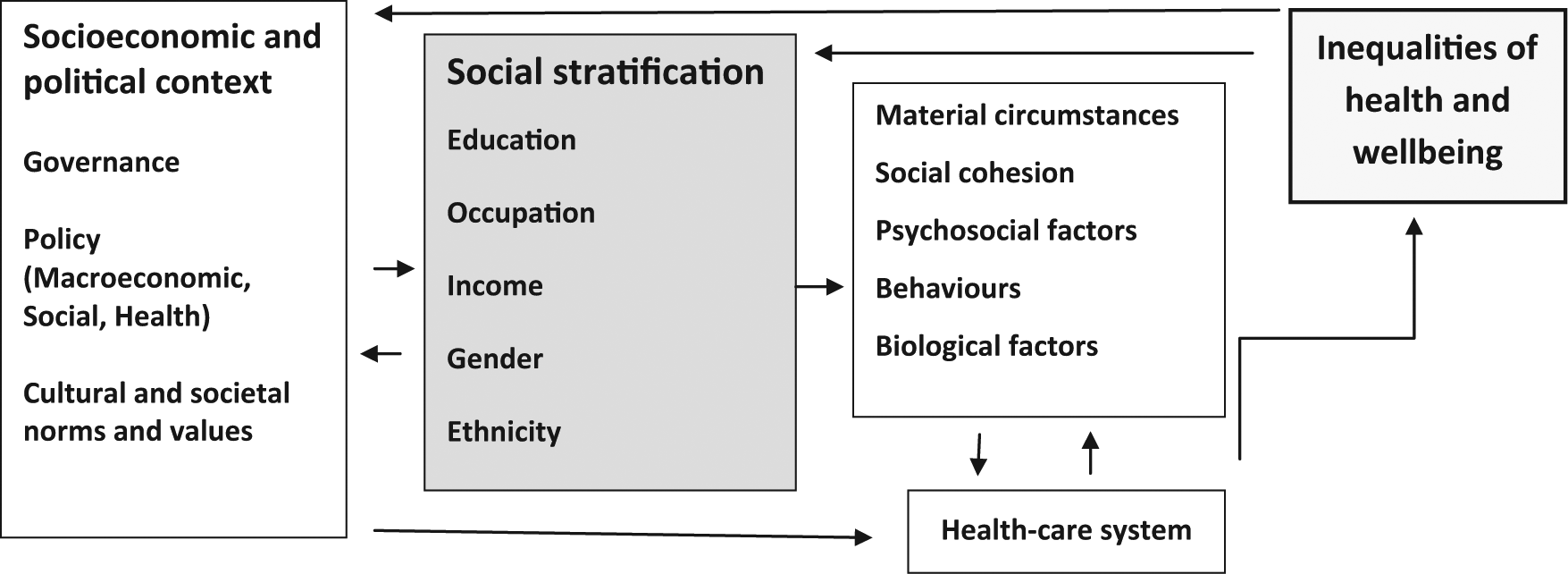
Conceptual framework on risk and health inequalities.
Countries with different levels of socioeconomic development face different health-risk challenges. There have been a limited number of studies on inequalities in health and their determinants in middle-income economies. The main challenges for such transitioning countries include the bipolar burden of disease pattern, with countries struggling to control legacy and emerging infectious diseases such as dengue, malaria, human influenza, HIV/AIDS, avian influenza, and multidrug resistant tuberculosis, while concurrently responding to the rapid growth in “new” health risks, such as chronic noncommunicable diseases (e.g., diabetes, hypertension) and traffic injury (WHO, 2011). Thailand is such a transitioning middle-income country in Southeast Asia.
Thailand has now experienced several decades of rapid economic growth and is grappling with the problems of economic and social inequality (National Economic and Social Development Board [NESDB], 2011). Over the past few decades, Thailand has been attempting to address concerns over health inequalities, and in particular has focused on inequities in use of health services, leading to the introduction of Universal Health Coverage in 2001 (Tangcharoensathien & Jongudomsuk, 2004; Wibulpolprasert, 2005). At present, almost all Thais are covered by health insurance but some socioeconomic and geographic inequalities still persist thus highlighting the need for continued effort in monitoring and action of an array of social determinants of health inequalities.
The aim of this article is to take advantage of the knowledge arising from the comprehensive analyses of data from a large national cohort study of the health-risk transition in Thailand (Sleigh, Seubsman, & Bain, 2008). Here we review the inequalities in health risks and outcomes identified to date in this ongoing Thai Cohort Study, noting inequalities of physical and mental health outcomes and their determinants. The objective of this article is to serve as a guide to introduce readers to a wide array of recent published health and social research from a large cohort of Thai adults. The findings for Thailand will be useful for other middle-income countries, revealing how health inequalities arise when social, economic, and health transitions occur.
The Thai Health-Risk Transition (The Thai Cohort Study)
In 2005, baseline questionnaires were mailed out to approximately 200,000 adult students enrolled at Sukhothai Thammathirat Open University (STOU) and 87,134 persons aged 15 to 87 years responded. The questionnaire was developed by a multidisciplinary team of experts in Thailand and Australia. Cohort participants were generally similar to the population of Thailand (especially in the 20-39 years age group) for sex ratio, median income, and geographical location (Sleigh et al., 2008). The self-administered baseline questionnaire covered demographic, socioeconomic and geographic information, physical and mental health status, history of doctor-diagnosed diseases, personal well-being, health service use, risk behaviors, traffic and nontraffic injuries, diet, physical activity, and family background. A 4-year follow-up was conducted in 2009 (n = 60,569, response rate = 70%) and an 8-year follow-up is currently underway in 2013.
Ethical Issues and Data Protocol
Ethics approval was obtained from STOU Research and Development Institute (Protocol 0522/10) and the Australian National University Human Research Ethics Committee (Protocols 2004/344 and 2009/570 for follow-up). Informed written consent was obtained from all participants. Data scanning and editing used Thai Scandevet software. Further data editing was completed using SQL and SPSS software. Besides descriptive results presented, an epidemiological approach was generally used for this review. The most common statistical analyses were multivariate binary logistic regression and multinomial logistic regression and reported Odds Ratios.
Following a multilevel eco-social model of health and its determinants operating to produce the Thai Health-Risk Transition (Figure 2), this review of inequalities in health and social outcomes includes five health-risk domains: demographic characteristics (age, sex, marital status), socioeconomic status (income, assets, work status), geographical influences (regions, urban-rural residence), health-related behavior (smoking, alcohol drinking), and environment (heat stress). Table 1 summarizes and comments on the findings for the health inequalities detected in the Thai Cohort Study.

Multilevel model adopted for the Thai Health-Risk Transition Study.
Health-Risk Determinants and Health Inequalities Among Thai Cohort Members.

Analyses used logistic regression reporting Odds Ratios (ORs).
Population attributable fractions were reported to give an indication of potential public health importance.
Analyses were based on multinomial logistic regression reporting Odds Ratios.
Demographic Attributes
Age, sex, and marital status were found to be strongly associated with health outcomes. For example, younger males were at high risk of road injuries and older females were at high risk of home injuries (Yiengprugsawan, et al., 2012b). Older males were more at risk of obesity, while younger females tended to be underweight (Banwell et al., 2009). Age and sex modified the inequalities in health measures. For example, reported happiness by marital status showed those separated, divorced, or widowed were the least happy, and this adverse effect was minimal among older females and maximal among younger males (Yiengprugsawan et al., 2012b).
Socioeconomic Status
High socioeconomic status is generally associated with better health outcomes but also is positively associated with obesity among older Thai males but negatively for young females in the cohort (Seubsman, et al., 2010b). In addition, smoking decreased among men with a higher level of education or income; in contrast, among women, higher incomes were associated with more smoking (Pachanee et al., 2011). Occupational-related heat stress, especially among those performing physical jobs, was found to be affecting overall health (Tawatsupa, et al., 2012b). Unemployment was also closely and negatively associated with happiness and well-being, especially notable among middle-aged and older males (Yiengprugsawan et al., 2012b).
Geographic Influences
Urbanization was shown to be a strong geographic influence on inequalities with positive outcomes (such as increase in attained height ; Jordan et al.., 2012) but also negative outcomes such as obesity and depression (Lim et al., 2009; Yiengprugsawan et al., 2011a). Urban living associated with various health-risk behaviors, including smoking, drinking, unhealthy diets, and physical inactivity (Lim et al., 2009; Pachanee et al., 2011; Yiengprugsawan et al., 2012a). One third of cohort members resided in urban areas in 2005 and had been rural residents at age 12. They were much more likely to be in smaller households, to have less intergenerational support, much less social interaction, support, and trust—all found to produce psychological distress (Yiengprugsawan et al., 2011b; Yiengprugsawan et al., 2011c).
Health-Related Behavior
Certain health-risk behaviors such as smoking and alcohol drinking were associated with adverse health outcomes such as hypertension among males (Thawornchaisit et al., 2013). Among females, hypertension was found to associate with eating behaviors such as roasted or smoked food (Thawornchaisit et al., 2012; Thawornchaisit et al., 2013) and obesity was strongly associated with frequent consumption of fried food and with Western food and sugary drinks (Banwell et al., 2009).
Environment
In tropical Thailand, heat interference could impact daily activities at home and in the workplace. Exposure to heat stress in the cohort associated with various health outcomes ranging from low energy, low life satisfaction, and psychological distress (Tawatsupa et al., 2010; Tawatsupa et al., 2012b). In particular, older men performing physical work who reported heat stress were twice as likely to report kidney disease (Tawatsupa, et al., 2012a). As well, occupation injuries were also found to be more prevalent among cohort members reporting heat stress (Tawatsupa et al., 2013).
Discussion and Conclusion
Set in Thailand, this study reviews existing analyses of health inequalities among adults evidenced by social and health outcomes. We identified important determinants of health inequalities that highlight the need for monitoring and understanding the needs of different population subgroups. For example, Thai females are much less likely to smoke or drink alcohol, partly explained by cultural difference. Demographic attributes and health-related behavior relate to younger males, drinking and sustaining traffic injuries; older males with increased socioeconomic status experience obesity, while other males with unemployment manifest psychological distress. Other associations were sociodemographic and environmental such as the link between physical jobs, heat stress, and kidney disease. Geographic influences such as lifetime urbanization associated with various health-risk behaviors (sedentary lifestyle, unhealthy eating) that in turn linked to many adverse health outcomes.
The strength of this study lies in its sample size, the nationwide residence of study participants, and the wide range of social and health outcomes available; in addition, data were generated from a longitudinal cohort making causal analyses available to examine social and health inequalities. We note one limitation of this review is its dependence on existing published papers arising from the Thai Cohort Study and that work is not yet completed and does not cover all possible health inequalities. As well, we acknowledge the university-level education of the cohort members, while facilitating the accuracy of self-administered questionnaires, could lead to a positive bias in health outcomes compared with the general population with lower education level.
This review has highlighted several important outcomes and associated upstream determinants amenable to policy interventions in transitional Thailand. These include heat stress—contributing to an array of adverse outcomes, including occupational injuries, psychological distress, and kidney disease; urbanization—with unhealthy eating, sedentary lifestyles, low social capital, and poor mental health; obesity—common among higher income and older men; and injury—common among young males and associated with alcohol and transport. Obesity, injury, psychological distress, and heat stress-related illness are all eco-social health outcomes produced by multilevel social determinants (Figure 2).
We have examined published epidemiological analyses of Thai health inequalities and their determinants along with associated adverse health outcomes. The observations arise in a transitional health-risk setting typical of many Asian emerging economies. The findings presented here are consistent with other reviews of social determinants of health outcomes (Friel et al., 2011a; Friel et al., 2011b). The 11th Thai National Economic and Social Development Plan (2012-2016) has addressed some of these emerging challenges (NESDB, 2011).
The next steps for the Thai Study involve completion of the 8-year cohort follow-up, currently underway for 2013/2014. The ongoing data linkage includes matching death records through the Thai Ministry of Interior and Ministry of Public Health. Analyses of mortality data, cause of death, and risk factors among the cohort members will provide further insights into the health-risk transition in Thailand. As well, ancillary studies are planned or underway on aging and caregivers, impact of heat stress, mental health, and chronic diseases including diabetes and cardiovascular diseases. Our current review points to the pressing need to address the main challenges—emerging chronic diseases related to urbanization, injury related to transport, and other adverse effects of heat stress on the general population and among physical workers. Promotion of healthy low-risk lifestyles and support for social capital in urban areas should be emphasized by multisectoral policy makers aiming to reduce social inequalities in health and to subsequently improve the health of the Thai population.
Footnotes
Acknowledgements
We thank the staff at Sukhothai Thammathirat Open University (STOU) who assisted with student contact and the STOU students who participated in the cohort study. Informed written consent was obtained from all participants. We would like to thank the editor and reviewer for helpful comments and suggestions that improved the manuscript.
Authors’ Note
The Thai Cohort Study Team: Thailand: Jaruwan Chokhanapitak, Chaiyun Churewong, Suttanit Hounthasarn, Suwanee Khamman, Daoruang Pandee, Suttinan Pangsap, Tippawan Prapamontol, Janya Puengson, Yodyiam Sangrattanakul, Sam-ang Seubsman, Boonchai Somboonsook, Nintita Sripaiboonkij, Pathumvadee Somsamai, Duangkae Vilainerun, and Wanee Wimonwattanaphan. Australia: Chris Bain, Emily Banks, Cathy Banwell, Bruce Caldwell, Gordon Carmichael, Tarie Dellora, Jane Dixon, Sharon Friel, David Harley, Matthew Kelly, Tord Kjellstrom, Lynette Lim, Anthony McMichael, Tanya Mark, Adrian Sleigh, Lyndall Strazdins, and Vasoontara Yiengprugsawan. Ethics approval was obtained from Sukhothai Thammathirat Open University Research and Development Institute (Protocol 0522/10) and the Australian National University Human Research Ethics Committee (Protocol 2009/570).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was supported by the International Collaborative Research Grants Scheme with joint grants from the Wellcome Trust, United Kingdom (GR071587MA), and the Australian National Health and Medical Research Council (NHMRC 268055), and as a global health grant from the NHMRC (585426).