
Abstract
The current study had two main objectives. The first was to investigate Botswana’s university students’ intentions to seek psychological help. The second was to investigate whether (a) Attitude Toward Seeking Professional Psychological Help (ATSPPH), (b) Self-Stigma of Seeking Help (SSOSH), and (c) Social Stigma of Receiving Psychological Help (SSRPH) predicted the students’ intentions to seek psychological help. A total of N = 519 (283 females and 236 males) students from the University of Botswana completed the survey. Results indicated that generally, the students had moderate intentions of seeking psychological help. Multiple regression analysis revealed that of the three predictors, only ATSPPH and SSRPH significantly predicted intentions to seek psychological help. The current study is important because while it has been established that university students are a high-risk population for mental health problems, there is close to nothing documented on university students in Botswana. Findings of the current study will undoubtedly increase knowledge relating to psychological help-seeking and its predictors in Botswana and may inform interventions that aim to encourage young people to seek psychological or counseling help.
Little is documented on Botswana’s university students’ intentions to seek psychological help and/or their attitudes toward seeking psychological help. This is despite the World Health Organization’s (WHO) estimations that in 2001 alone, 121 million people suffered from depression; 24 million suffered from schizophrenia; 70 million were affected by alcohol use disorders; and 5 million were negatively affected by drug use disorders. While these statistics are global, they still suggest that in a lifetime, any individual may suffer from a mental disorder, come into contact with someone with a mental disorder, and/or have to care for someone with a mental disorder. The statistics also suggest that individuals need knowledge to realize when they or others may be suffering from psychological disorders, and to know when to seek help or to advice their close others to seek help. Such need is also exacerbated by research that suggest that university students are a high-risk population for mental health illness problems (Ryan, Shochet, & Stallman, 2010) as being at university may present threats to the student’s emotional well-being (Wittenberg, 2001).
In Botswana, this might be worsened by the generally negative historical views of mental illness (Seloilwe & Thupayagale-Tshweneagae, 2007) and the fact that a large number of students in Botswana have to relocate from many different remote areas to the capital city for their university education. Such migrations, coupled with interactions with new groups of people, loss of contact with familiar people, and changing environmental conditions (Sabone, 2009) may further add to the challenges students face as they adapt to the new environments (i.e., the city and university environments).
The University of Botswana is the largest university in Botswana, and like many universities across the world, it has a counseling service for the students. While existence of such facilities should be applauded, researchers have reported that, generally, few university students seek professional help when experiencing problems (Wade, Post, Cornish, Vogel, & Tucker, 2011). This makes it important for researchers and practitioners to investigate factors that may facilitate or inhibit intentions to seek psychological help.
In line with the currently ongoing debate about the possibility of indigenizing psychology in the African context (Moll, 2002), there is a need to address the issue of why knowledge documented elsewhere about stigma and help-seeking behaviors might not be adequate to address the challenges specific to a country like Botswana. Furthermore, Mpofu (2002) also noted the benefits of including and documenting African experiences in the literature of psychology, arguing that it will not only enrich the discipline, but will also make it globally relevant. The current study is important more so that psychology is a fairly new discipline in Botswana. For example, to the knowledge of the authors, the only existing psychology department (i.e., a university teaching department) in the whole country was only established in 2004 at the University of Botswana (www.ub.bw).
According to Plattner and Moagi-Gulubane (2010), it was observed that the majority of counseling services in communities around Botswana were being offered by individuals who were not specifically trained as psychologists. To bridge the gap in the provision of these essential services, the BPsych program at the University of Botswana was tailored to provide the graduates with skills that would enable them to work as professionals under supervision. However, a lot remains to be done in terms of educating the public and getting them to appreciate the need to seek psychological help.
Outside Botswana, factors contributing to people’s reluctance to seek psychological help include stigmatization of mental illnesses (Corrigan, 2004; Narikiyo & Kameoka, 1992), emotional openness (Komiya, Good, & Sherrod, 2000), self-reliance (Tata & Leong, 1994), and age (Currin, Hayslip, Schneider, & Kooken, 1998), while others include fear (Kushner & Sher, 1989), a person’s outcome expectations (Fischer, Jome, & Atkinson, 1998; Halgin, Weaver, Edell, & Spencer, 1987; Kim, Ng, & Ahn, 2005; Vogel, Wester, Wei, & Boysen, 2005), gender (Addis & Mahalik, 2003; Pederson & Vogel, 2007; Tata & Leong, 1994), one’s discomfort with self-disclosing information (Vogel & Wester, 2003), and one’s cultural orientation (Tata & Leong, 1994). While these factors may also be significant in Botswana, this has not been confirmed through research. Specific to Botswana, the challenges may include preferences of other sources of intervention such as traditional doctors, family, and religious leaders. For instance, it has been documented that irrespective of the level of education and social status, Batswana continues to seek help from traditional healers (Stockton, Nitza, & Bhusumane, 2010). Furthermore, the need for understanding university students’ intentions of seeking psychological help and/or their attitudes toward seeking psychological help is further heightened by the Botswana’s HIV/AIDS challenges, alcohol and drug problems, high unemployment rate, and the scourge of “passion killings.”
In line with the above-mentioned gap in research, the current study was an exploratory study with two main objectives. The first was to investigate Botswana’s university students’ intentions of seeking psychological help. The second was to investigate whether (a) Attitude Toward Seeking Professional Psychological Help (ATSPPH), (b) Self-Stigma of Seeking Help (SSOSH), and (c) Social Stigma of Receiving Psychological Help (SSRPH) predicted the students’ intentions to seek psychological help. The findings of the current study might also inform human services programs, the educational programs, researchers, and practitioners, and also enable them to have targeted programs that encourage help-seeking behaviors for university students in Botswana and in other similar countries.
Theoretical Background
Intentions to Seek Counseling
Research suggests that there are many factors that may affect one’s decision to seek help when faced with a psychological problem. Furthermore, it has been noted that intention is one of the good predictors of such behavior (e.g., Bathje & Pryor, 2011). As suggested by Mechanic (1966), the care-seeking process can be influenced by social and cultural factors. Others added that personal and agency factors (i.e., factors relating to counseling services such as the service and the counselor) may also affect intentions (Fischer, Winer, & Abramowitz, 1983; Setiawan, 2006). Seloilwe and Thupayagale-Tshweneagae (2007) further added that care of the mentally ill in most societies takes place within complex historical, economic, political, social, and cultural contexts, pointing to the need to investigate factors that may facilitate help-seeking behaviors in different socio-economic-cultural-political contexts.
The current study focused on Botswana university students because researchers have also highlighted problems in accessing mental health services (Kurtz & Street, 2006) and on the decision to seek mental health services for individuals from minority ethnic groups and university students. It is also important to understand the reception of mental health services in contexts like Botswana where the treatment modalities, the practices, and the approaches used in psychotherapy are mostly imported from the Western world. It is noteworthy that Botswana has transformed from a society that solely associated mental disorders with witchcrafts and/or possession of bad spirits to a society that has recognized the need for counseling centers and mental hospitals (Seloilwe & Thupayagale-Tshweneagae, 2007).
Studies conducted elsewhere have consistently revealed that many individuals who could potentially benefit from psychological services do not seek help or follow-through with treatment (Corrigan, 2004; Jorm, 2000). This makes it important for Botswana practitioners and researchers to understand some of the barriers to seek counseling or any other related mental health services within Botswana. Pepin, Segal, and Coolidge (2009) classified barriers associated with seeking and utilizing mental health services into intrinsic barriers (i.e., barriers that operate within an individual) and extrinsic barriers (i.e., barriers that operate outside of an individual). The current study focused on intrinsic factors only that included a negative view of mental disorders, stigma associated with seeking or receiving mental health services, or limited knowledge about the potential benefits of psychotherapy. While it is understood that having intentions to seek treatment is a different process, distinct from actually contacting the mental service providers (Saunders, 1993), the current study only measured students’ intentions to seek counseling and factors that might influence such a process. Given the Batswana’s general negative cultural and historical views of the mentally ill (Seloilwe & Thupayagale-Tshweneagae, 2007), it was predicted that university students may have low intentions of seeking psychological help.
Attitudes Toward Seeking Psychological Help
Greenwald and Banaji (1995) defined attitudes as favorable or unfavorable dispositions toward an attitude object, such as people, places, and policies. They further explained that positive correlations have been established between measured attitudes and the favorable aspects of observed behavior. It has also been revealed that people from ethnic or minority groups are likely to hold negative and stigmatizing attitudes toward mental disorders and the mentally ill (Papadopoulos, Leavey, & Vincent, 2002). Moreover, people who have little knowledge and contact with the mentally ill are likely to hold even stronger negative attitudes toward people with mental disorders (Papadopoulos et al., 2002). Other studies have revealed that such negative attitudes toward help-seeking are strongly related to lower intentions to seek counseling (e.g., Bathje & Pryor, 2011). Specifically, negative attitudes toward help-seeking have been found to reduce the likelihood of using mental health care services and the likelihood of perceiving the need to seek psychological help (Mojtabai, Olfson, & Mechanic, 2002).
Stigma in Seeking and Receiving Psychological Help
Researchers have also revealed that stigma associated with mental disorders may be one of the key factors that inhibit individuals from seeking help from mental help professionals (Saunders, 1993; Vogel, Wade, & Haake, 2006). This is because being diagnosed with a psychological disorder and the actual act of seeking treatment appear to be stigmatizing (Ben-Porath, 2002). For example, in one study, Kurtz and Street (2006) revealed the participants’ fear of the stigma surrounding mental health and also the effect of such stigma on young people’s reluctance to discuss their challenges with individuals they did not know or did not trust. In countries like Botswana, even families with persons who show signs of any mental disorder may also be stigmatized, which may lead them to avoid seeking the necessary assistance for fear of being either labeled or ostracized (Seloilwe & Thupayagale-Tshweneagae, 2007). According to Corrigan and Watson (2002), different components or types of stigma are commonly present in the general public, and even in the stigmatized individuals. For instance, individuals may expect to be socially rejected before they receive psychological help, or actually experience social rejection after participating in mental health treatment (Link, 1987; Verhaeghe, Bracke, & Christiaens, 2010). They may then consequently engage in self-rejection or self-stigma (i.e., experience shame and feelings of inferiority as a result of receiving or seeking mental health service; Verhaeghe et al., 2010). Corrigan (2004) differentiated between public stigma (we also referred to this type of stigma as social stigma) and self-stigma, and other researchers have also emphasized the need to study multiple dimensions and multiple outcomes of stigma experiences (e.g., Verhaeghe et al., 2010). Therefore, in the current study, the impact of public/social stigma and self-stigma on the intentions of seeking psychological help were investigated separately.
Public/SSRPH
The public/social stigma is influenced by the societal response to people who seek or receive help for psychological distress (Bathje & Pryor, 2011). This type of stigma may be viewed as a form of prejudice comprising affective, behavioral, and cognitive reactions to the individual seeking psychological help (Corrigan et al., 2005). Furthermore, it may involve the actual negative stereotypes and/or discriminating behaviors against the stigmatized individuals (Corrigan, 2004), or in some instances, the awareness of responses to people with mental disorders or people who seek mental health services. People with mental disorders may be viewed as dangerous (Crisp, Gelder, Rix, Meltzer, & Rowlands, 2000), embarrassing, socially disagreeable (Coolidge, Mincic, & O’Riley, 2005), and/or even responsible for their own illnesses (Corrigan et al., 2005). Social stigma associated with seeking or receiving psychological help does not only affect those diagnosed or perceived as mentally ill. For instance, Lefley (1989) and Corrigan, Watson, and Miller (2006) suggested that stigmatization of the mentally ill generalizes to their family members because of social barriers that are erected against the relatives and households of the mentally ill. Corrigan, Watson, et al. (2006) further explained that the behaviors of persons with psychotic disorders may also diminish the family’s reputation, and jeopardize relationships with friends and neighbors. Therefore, a negative relationship between social stigma of seeking psychological help and intentions of seeking professional psychological help was expected.
SSOSH
The self-stigma is the individual self-labeling that can negatively impact one’s participation in society at large (Holmes & River, 1998). Self-stigma has also been shown to negatively impact one’s perceived self-worth, self-esteem, and has also been linked to outcomes such as depression and reluctance to seek help (Corrigan, Watson, & Barr, 2006; Holmes & River, 1998; Link & Phelan, 2001). Bathje and Pryor (2011) conceptualized it as the internalized impact of social stigma. Accordingly, Holmes and River (1998) suggested that adequate help of individuals coping with mental disorders should involve addressing societal and self-stigma. Kroska and Harkness (2008) explained that self-stigma works in such a way that when an individual is first diagnosed with a mental illness, cultural ideas and stereotypes that have been linked with the mental illness or the mentally ill individuals become personally relevant and promote negative self-feelings. Thereafter, the individual expects others to reject him/her, in turn, triggering defensive behaviors aimed at preventing the rejection. Such defensive behaviors may include: hiding one’s treatment history, withdrawing from social interaction, and/or teaching others about mental illness. Such conceptualization of self-stigma suggests that awareness and endorsement of public/social stigma are necessary to generate self-stigma (Corrigan, Watson, & Barr, 2006). Overall, understanding stigma is important for researchers and practitioners as it gives insights into why individuals with significant life problems may be hesitant to seek professional help (Vogel et al., 2006). As a result of the above discussions, the following hypothesis were formulated and tested:
Hypothesis 1: Students will report low intentions of seeking professional psychological help.
Hypothesis 2: Positive attitudes toward seeking professional psychological help positively predict intentions of seeking professional psychological help.
Hypothesis 3: Public/social-stigma of receiving psychological help negatively predicts intentions of seeking professional psychological help.
Hypothesis 4: Self-stigma of seeking psychological help negatively predicts intentions of seeking professional psychological help.
Method
Participants
A convenient sample of total of N = 519 (283 females and 236 males) University of Botswana students completed the survey. Participants between the ages of 16 and 20 comprised 38.7% of the sample, 21 and 24 comprised 35.0% of the sample, 26 and 30 comprised 5.0% of the sample, and above 31 comprised 8.9% of the sample. In terms of nationality, 82% indicated they were Batswana, 2.1% indicated that they were other African nationalities, and 0.4% indicated that they were other nationalities. The majority (90.0%) of the participants were single, 9.6% were married, and 4% were widowed. Most of the participants did not have children (81.8%). The sample consisted of 147 first-year students, 139 second-year students, 97 third-year students, 106 fourth-year students, 28 fifth-year students, and 1 student who was in the sixth year. There were no group differences on any other sociodemographic variables.
Procedure
Ethics clearance for the research was obtained from Botswana’s Ministry Health. Data were collected using paper-and-pencil surveys. Specifically, questionnaires were distributed to students in classroom settings. Participants were treated in accordance with the ethical principles of the Botswana’s Ministry Health. Specifically, the questionnaire started with a participant information cover page that detailed research objectives, informed the participants of their right to withdraw from the research at any time, and requested their consent. It took between 20 and 30 min to complete the questionnaire.
Measures
Intentions of seeking psychological help
Intentions of seeking psychological help were assessed with the Intentions to Seeking Counseling Inventory (ISCI) by Cash, Begley, McCown, and Weise (1975). The ISCI is a 17-item scale that measures participants’ intentions to seek counseling services for a range of specified problems. The scale contains some of the following items: weight control, excessive alcohol use, depression, test anxiety, and loneliness. For each item, participants were asked to rate on a scale from 1 (very unlikely) to 4 (very likely) how likely they were to seek counseling if they were experiencing the listed problem. Support for construct validity of the ISCI has been provided by the findings that participants who reported greater self-stigma associated with seeking psychological help as measured by the SSRPH had less intentions to seek treatment for psychological and interpersonal concerns as measured by the ISCI (Vogel et al., 2006), and positive association between the ISCI and the ATSPPH (Kelly & Achter, 1995). Coefficient alpha in the current study was α = .91, indicating a strong reliability.
Attitudes Toward Seeking Professional Psychological Help Scale
ATSPPH was measured with the 10-item shortened version of the Attitude Toward Seeking Professional Psychological Help Scale (Fischer & Farina, 1995) originally developed by Fischer and Turner (1970). A sample of items on the scale included: “If I were experiencing a serious emotional crisis at this point in my life, I would be confident that I could find relief in psychotherapy” and “I would want to get psychological help if I were worried or upset for a long period of time.” Items on this scale were scored on a scale from 1 (disagree) to 4 (agree). Higher scores on this measure reflected a more positive ATSPPH. Internal consistency of the measure has been found to be acceptable (α = .82; Vogel et al., 2005). The scores on the Self-Stigma of Seeking Psychological Help scale also significantly predicted ATSPPH (Vogel et al., 2006), indicating a good construct validity. Coefficient alpha in the current study was α = .50.
Self-Stigma of Seeking Help Scale
The self-stigma associated with seeking psychological help was measured with the Self-Stigma of Seeking Help (SSOSH) scale (Vogel et al., 2006). The SSOSH has 10 questions and responses on this scale were rated on a 4-point Likert-type scale ranging from 1 (strongly disagree) to 4 (strongly agree). Higher scores indicated a greater perception of self-stigma associated with seeking psychological help. Sample items on this subscale include “Seeking psychological help would make me feel less intelligent” and “It would make me feel inferior to ask a therapist for help.” In the current study, internal consistency for this scale was α = .66.
Social Stigma of Receiving Psychological Help Scale
SSRPH was measured with the Social Stigma of Receiving Psychological Help Scale (Komiya et al., 2000). The scale contained five questions each rated on a 4-point Likert-type scale ranging from 1 (strongly disagree) to 4 (strongly agree). Higher scores in this scale indicated greater perceptions of social stigma associated with receiving professional psychological help and lower scores indicated lesser perceptions of social stigma associated with receiving professional psychological help. Sample items on this scale included “Seeing a psychologist for emotional or interpersonal problems carries social stigma” and “People will see a person in a less favorable way if they come to know that he or she has seen a psychologist.” The coefficient alpha for the SSRPH was initially found to be α = .73 (Komiya et al., 2000), and in another study it was .76 (Vogel et al., 2006). In the current study, α =.73.
Results
Statistical Analyses
First, Cronbach’s alpha coefficients (α) were calculated to assess the internal consistency of the measuring instruments (Clark & Watson, 1995; Cortina, 1993). Table 1 presents the means, standard deviations, and alpha coefficients of measures.
Means, Standard Deviations, and Alpha Coefficients of Measures.

Second, for those scales yielding a low alpha (i.e., ATSPPH and SSOSH) further analyses were conducted to identify problematic items. Despite the low Cronbach’s alpha, the item analyses on both scales did not indicate that the removal of any of the items would improve the scale’s Cronbach’s alpha. To further identify the problem with the scales, the items were factor analyzed using Exploratory Factor Analysis (EFA) and principal axis factoring analysis with a direct oblimin, that is, an oblique rotation. The scales were expected to manifest unidimensional set of items to reflect variance in their latent variables.
For the SSOSH scale, the initial EFA analysis results (Table 2) identified all the reverse-coded items as problematic as the items loaded on the separate extracted factor. 1
Exploratory Factor Analysis of the Self-Stigma of Seeking Help Scale.

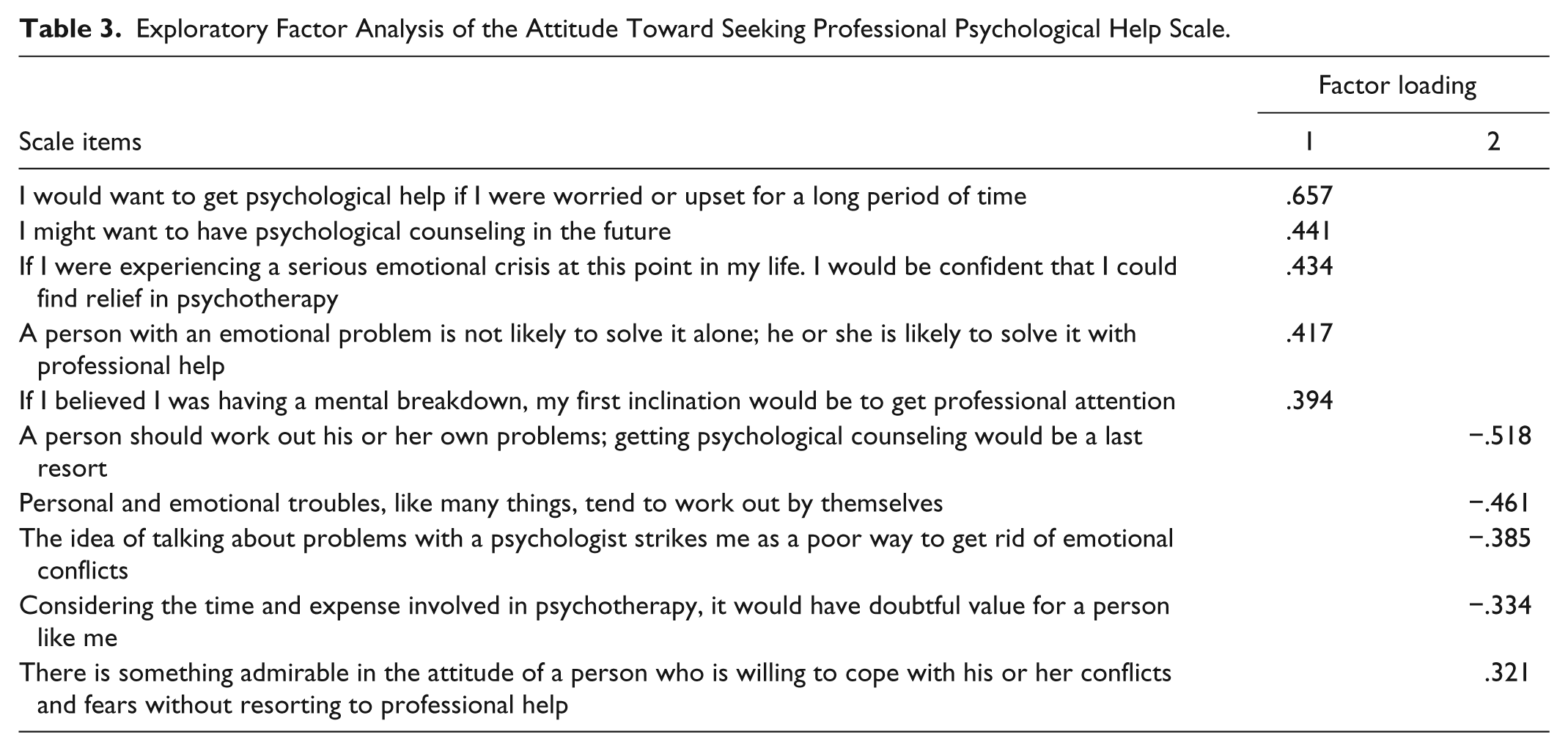
Another problematic scale was the scale measuring ATSPPH. Following a low alpha, the scale was also subjected to EFA. The results presented in Table 3 show that similar to the SSOSH scale, all the reverse-coded items and one extra item that was not necessarily reverse-coded (i.e., “Considering the time and expense involved in psychotherapy, it would have doubtful value for a person like me”) also failed the unidimensionality test. 2
Exploratory Factor Analysis of the Attitude Toward Seeking Professional Psychological Help Scale.
As per recommendations of Hair, Babin, Money, and Samouel (2003) regarding the use of alphas below .70 in preliminary studies, a decision was made to still use all the scales in further analysis. Items from each scale were therefore summed together to form indexes measuring ATSPPH, intentions of seeking counseling (ISC), SSOSH, and SSRPH.
The second set of statistical tests was conducted to assess the students’ ISC. Table 4 shows the descriptive results of students’ scores of ISCI. Other researchers have identified three subscales (i.e., Interpersonal Problems, Academic Problems, and Drug/Alcohol Problems; Cepeda-Benito & Short, 1998) of the ISCI. In the current study, an attempt was made using EFA to evaluate the factor structure of the 17 items. Unfortunately, the current data did not yield the factor structure identified by Cepeda-Benito and Short (1998).
Students Intentions to Seek Counseling.

Nonetheless, other researchers have summed the items of the ISCI to yield scores ranging from low to high, with higher scores indicating a greater likelihood of seeking counseling for the various problems (e.g., Kelly & Achter, 1995; Leech, 2007). In the current study, the items were also summed to yield scores ranging from 17 to 68. The summed scores were also used to conduct correlations and multiple regression analyses. To examine students’ intentions of seeking help, it was also deemed necessary to evaluate students’ intentions to seek help for each one of the listed items. Finding past research that established cutoffs for the scale was difficult. Therefore, in the current study, it was decided that as the responses ranged from 1 = very unlikely, 2 = unlikely, 3 = likely, to 4= very likely, for each item, any scores 2.0 and below will indicate that the participants were unlikely to seek help for the identified problem. In addition, any score between 2.1 and 3.0 were used to reflect that the individual has low to moderate intentions to seek help, while the scores above 3.0 indicated that the individuals were more likely to seek help for the specified problem. The results revealed that for most of the areas of concern, the mean scores ranged from 1.96 to 3.45. The average mean score was 2.82 (SD = 0.61).
Predictive Analyses Using Multiple Regression
Before conducting multiple regression analysis, descriptive statistics and intercorrelations were calculated for all study variables. The correlation matrix is presented in Table 5. Conducting correlation analysis was important in detecting multicollinearity that may occur when predictor variables are overcorrelated. Multicollinearity may cause some problems in validation, interpretation, and analysis of the model (Feng-Jeng, 2008). A general rule of thumb is that variables with a correlation (r < .75) may cause multicollinearity. In our study, all correlation coefficients were below .40.
Correlation Matrix.

Note. ATSPPH = Attitude Toward Seeking Professional Psychological Help; ISC = Intentions of Seeking Counseling; SSOSH = Self-Stigma of Seeking Help; SSRPH = Social Stigma of Receiving Psychological Help.
p < .05. **p < .01, two-tailed.
The last step of the statistical analysis involved using multiple regression analyses to test the hypotheses that ATSPPH, SSOSH, and SSRPH predict the students’ intentions to seek counseling (i.e., Hypotheses 2, 3, and 4). Table 6 summarizes the results of the regression analysis. The total model was statistically significant, R2 = .20, F(3, 379) = 31.50, p < .01. This indicates that 20% of the variance was explained by the three predictors. Hypothesis 2 stated that ATSPPH positively predicts ISC. In our data, Hypothesis 2 was supported (B = .38, t = 7.58, p < .001). Hypothesis 3 stated that SSRPH negatively predicts ISC. Hypothesis 3 was also supported (B = −.11, t = −2.60, p < .05). Hypothesis 4 stated that SSOSH negatively predicts ISC. While the relationship was in the hypothesized direction, the hypothesis was not supported (B = −.05, t = −.86, p > .05). 3
Regression Analysis.

Note. R2 for the regression equation is .20 (p < .001). SE = Standard error; ATSPPH= Attitude Toward Seeking Professional Psychological Help; SSOSH = Self-Stigma of Seeking Help; SSRPH = Social Stigma of Receiving Psychological Help.
p < .01.
Discussion
As expected, correlation analysis showed that perceived social stigma was positively related to self-stigma; self-stigma and perceived social stigma were negatively associated with the attitudes toward seeking psychological help and ISC; and that positive attitudes toward seeking psychological help were positively associated with ISC.
Results from the current study revealed that the University of Botswana’s students generally have low to moderate intentions to seek counseling. In particular, depression, excessive alcohol use, and drug problems received the highest mean scores. The only area of concern that the students were unlikely (i.e., receiving a mean score of less than 2.0) to seek counseling for was weight control. Other areas of concern receiving the lower mean scores included speech anxiety, difficulty with friends, and difficulties of dating.
The ISCI was used in another study aimed at measuring the effects of mental health education on students’ willingness and intentions to seek counseling by Hobson (2008). In Hobson’s study, the experimental group was exposed to mental health education and the control group was not. The findings revealed that means on the ISCI for the experimental group were found to be significantly higher (M = 42.45, SD = 8.24) than the means for the control group (M = 37.21, SD = 9.42; Hobson, 2008). In another study, where 732 students also completed questionnaires about their perceived likelihood of seeking professional psychological help, the findings revealed a mean of 45.86, SD = 16.45 (Cepeda-Benito & Short, 1998). In another study by Kelly and Archer (1995), the mean score for the ISCI overall scale was 46.04, SD = 17.1. The mean for the current study (M = 47.91, SD = 10.40) was therefore considered slightly higher than Kelly and Archer’s (1995) and Cepeda-Benito and Short’s (1998) studies and was comparatively higher than in Hobson’s (2008) study.
While the ISC scale yielded a very good alpha, some of the items in this scale might have been perceived as not warranting the need for one to seek psychological help. For example, being in the plus size range is not necessarily perceived negatively by Batswana and subsequently not an issue worth the attention of a counselor. Problems related to speech anxiety, difficulty with friends, and difficulties of dating also received lower mean scores. Lack of knowledge on the availability of counseling resources could be one possible contributing factor, especially as noted earlier that psychology as a profession is relatively new in the country of Botswana and formal training for undergraduates was only introduced in 2004. Another possible explanation is that, in Botswana, the practices and approaches used in psychotherapy are mostly imported from the western world. As a result, the majority of the population might still prefer traditional avenues like traditional healers, priests, family, and/or friends to deal with challenges like dating problems.
These findings also point to the need for exposure to psychological education as these might help to dispel myths about the field and make people more aware of the benefits that one can accrue from seeking counseling. Furthermore, the Batswana’s cultural and historical views of the mentally ill as explained by Seloilwe and Thupayagale-Tshweneagae (2007) might also keep the students from seeking counseling for certain psychological problems.
Regression analysis showed that a positive attitude toward seeking psychological help positively predicted intentions to seek psychological help. These findings support past research that has shown that negative attitudes toward help-seeking has been found to reduce the likelihood of using mental health care services (e.g., Bathje & Pryor, 2011; Mojtabai et al., 2002). As predicted, the results also showed that SSOSH and SSRPH were negatively correlated with the intention to seek psychological help. However, it was only the SSRPH that significantly predicted intentions of seeking psychological help. The findings that perceived social stigma and negative attitudes negatively affect utilization of psychological services are consistent with literature on the centrality of sociocultural factors of negative perceptions of mental disorders for those afflicted with mental disorders (Kgathi, 2005; Papadopoulos et al., 2002) among groups that has not traditionally used psychological help. Researchers have noted among these ethnic groups that where there is perceived negative reaction of the family and the community (i.e., where salient beliefs and valued social norms are incongruent with seeking psychological help), individuals are less likely to have intentions to seek help when faced with a psychological problem (Goldston et al., 2008).
Contrary to the stated hypothesis, internalized self-stigma was not found to significantly predict ISC among the University of Botswana students. While researchers have suggested that individuals from groups with collective orientations may face greater self-stigma associated with seeking counseling (e.g., Goldston et al., 2008); such suggestions were, however, refuted in the current study. Researchers have suggested that stigma vary across cultures as it might be influenced by social and cultural contexts (Pescosolido, Martin, Lang, & Olafsdottir, 2008). This may also be explained by suggestions that individuals tend to have either independent or interdependent self-construals (Schein, 1984), and this might affect whether they are impacted more by the self-stigma or the social stigma. In collectivistic cultures like Botswana, identity may be embedded in social groups in which interdependence among group members is emphasized (Cheung & Halpern, 2010; Markus & Kitayama, 1991). For individuals with interdependent self-construals, endorsing the societal stereotype of people who seek or receive help for psychological distress might be easier than for people with independent self-construals because how “others” view them is important for the development of the self. Furthermore, public/social stigma might also be more damaging as the individuals might also like to protect their family/group image from associations with mental disorders as it has been suggested that in countries like Botswana even families with persons who show signs of mental disorders may also be stigmatized (Seloilwe & Thupayagale-Tshweneagae, 2007).
Limitations of the Current Study
In interpreting the findings from the current study, some limitations should be taken into account. First, while the study used existing instruments that have been used broadly in studying self-stigma, social stigma, intentions of seeking psychological help, and ATSPPH, in the current study, some of the instruments revealed low alphas necessitating removal of certain items to strengthen reliability. These findings suggest that the instruments that have been designed from different contexts need to be piloted first to ensure their validity and/or reliability. Still relating to this limitation, even after removing some of the items from the Attitude Toward Seeking Psychological Help scale, the scale still yielded an alpha lower than the recommended critical cutoff value. While the use of scales with such alphas has been recommended for preliminary studies, caution in interpreting the results still need to be exercised as such measures might have inflated or deflated the results.
In addition, the study’s sample limits the generalizability of the findings such that the findings might only apply to the context of the University of Botswana. The study also used a cross-sectional design where all the variables were assessed at one point in time. However, data analysis did not control for intervening and moderating variables that could have contributed to the relationships. The results were also based on self-reporting, and these could have inflated the magnitude of relationships due to common method variances. Despite these limitations, the results of the current study expand previous findings regarding college students’ intentions to seek counseling and also highlighted important similarities in a different culture.
Implications and Suggestions for Future Research
Overall, the limitations of the present study point out several avenues for future research. For example, the low reliability of the ATSPPH and the SSOSH suggests that researchers in different contexts might need to design their own instruments or use varying instruments for measuring the two constructs. Furthermore, to address concern regarding intervening variables, testing moderational models, mediational models, longitudinal designs, and experimental designs might provide a more rigorous test of the proposed relationships. The role of variables such as gender, upbringing, age, and even spiritual beliefs could also be assessed when exploring the relationships between attitudes, stigma, and Batswana college students’ ISC. For instance, the seemingly existence of a parallel system where Batswana continue to seek help from professional counselors and traditional healers (Bhusumane, 2007) requires professionals to understand how indigenous method and practices may enhance or comprise the counseling process.
Research has also suggested that university students tend to seek help from a variety of sources; however, the present study has only focused on help-seeking from mental health professionals. It is therefore important to investigate the student’s intentions to seek help from other sources. Another important issue that needs to be investigated is whether intentions to seek counseling are also related to actual behaviors. While researchers such as Ajzen (2001) have demonstrated the link between the attitudes, intentions, and behavior, it is still important for us to conduct research that fully examines the link between intentions and behavior in the Botswana context.
Given the importance of cultural norms and values, future research should also explore the intentions to seek psychological help from a cultural orientation point of view. For example, Botswana is a country developing economically and socially, and such developments directly impact the cultural landscape of Batswana; hence, longitudinal studies would be vital to examine the effects of those changes on perceptions of psychological help-seeking patterns.
The findings also have implications for research and psychological intervention program designs as there might exist specific sociocultural factors that differently influence Batswana university students’ decision to seek psychological help. Such interventions may include psychological education and outreach. Practitioners in Botswana may also need to be innovative in coming up with varying treatment options for individuals who may be experiencing or anticipating social stigma or any other negative consequences of seeking help.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by the University of Botswana’s Research Grant Number R-825.