
Abstract
States vary in standards for sex education, some requiring an emphasis on abstinence. Schools seek to identify curricula that reflect local community values and meet state standards. Choosing the Best (CTB), a classroom-based abstinence education curriculum, has been implemented in 75 Georgia school districts since 1995. CTB Inc., sought to determine if this popular program had an impact on abstinence attitudes, intentions, and behavior. Six Georgia public schools (1,143 ninth graders) participated in the study in 2009-2010. Four randomly assigned schools received the CTB curriculum, taught by trained CTB staff. Two control schools received their usual textbook-based abstinence lessons. Surveys were conducted at the beginning and end of 9th grade, and the beginning of 10th grade. Data demonstrated significant impact of CTB at the end of 9th grade on commitment to abstinence, proabstinence beliefs and attitudes, intentions to maintain abstinence, and lower onset of sexual intercourse, and at the beginning of 10th grade on proabstinence attitudes. In two communities that sought an abstinence education approach, CTB had a short-term impact on abstinence attitudes, commitment, and behaviors, and a longer term impact on abstinence attitudes only.
Keywords
Introduction
School-based sex education programs have undergone dramatic shifts in focus and content over the past two decades. In 1996, Title V of the Social Security Act authorized US$50 million per year, requiring proportional state-matching funds, to provide education that met the specific “A-H” definition regarding abstinence until marriage, and it was reauthorized in 2003 (U.S. Department of Health and Human Services, 1997, 2002). As the political landscape changed, funds were appropriated in 2009 for a new Teen Pregnancy Prevention (TPP) initiative to implement specific programs identified as effective, or deemed “promising” based on preliminary research criteria designated by TPP. The majority of the TPP programs funded have been comprehensive sex education programs, although limited funds for abstinence education programs were appropriated in the 2010 health reform legislation (Boonstra, 2010).
Since 1996, a variety of abstinence education programs proliferated. Evaluation of their impact, however, has yielded only limited studies, which have suggested delayed sexual initiation (Denny & Young, 2006; Weed, Ericksen, Lewis, Grant, & Wibberley, 2008), several demonstrating that the programs were not effective (Kirby, 2002; Silva, 2002; Thomas, 2000; Trenholm et al., 2008), or studies have not been rigorous enough to draw conclusions (Kirby, 2007, 2008). One study demonstrated long-term impact of an abstinence program on sexual behavior; however, the program’s definition of abstinence did not meet A-H abstinence-until-marriage guidelines (Jemmott, Jemmott, & Fong, 2010).
While the Federal government has made a significant investment in abstinence education since 1996, states have varied widely in their approaches to curriculum requirements, some taking advantage of the federal funds and their associated matching requirements, which required programs to meet the A-H abstinence-only-until-marriage definition. Other states opted out of the federally funded program, thereby not having access to the federal funds, but enabling individual school districts to choose programs with or without the A-H emphasis (Boonstra, 2010).
Meanwhile, state standards for curricula vary widely. A total of 18 states and the District of Columbia require information on contraception, while 18 require instruction on the importance of engaging in sexual activity only within marriage (Guttmacher Institute, 2011). In all, 13 states expressly require inclusion of information on the negative outcomes of teen sex and pregnancy, and 36 require that instruction on abstinence be provided. Georgia mandates that sex education for public school students include “abstinence from sexual activity as an effective method of prevention of pregnancy, sexually transmitted diseases, and acquired immune deficiency syndrome.” Furthermore, Georgia allows, but does not require, information on condoms or contraception (State of Georgia Department of Education, 2011). Similarly, Texas, Alabama, and Mississippi promote or require schools to adopt programs that focus exclusively or at least partially on abstinence (Table 1; eLobbyist, 2011; FindLaw for Legal Professionals, 2011; The Institute for Youth and Development, 2004). Despite varying state standards, a significant number of teens nationwide continue to report having sex and engaging in behaviors that place them at risk for pregnancy, HIV, and sexually transmitted infections (STIs; Centers for Disease Control and Prevention [CDC], 1991-2009). As individual communities seek to address these issues, school districts try to identify curricula that both reflect local community values and meet their state education standards.
Language From the Educational Standards of Selected States That Emphasize Abstinence Education
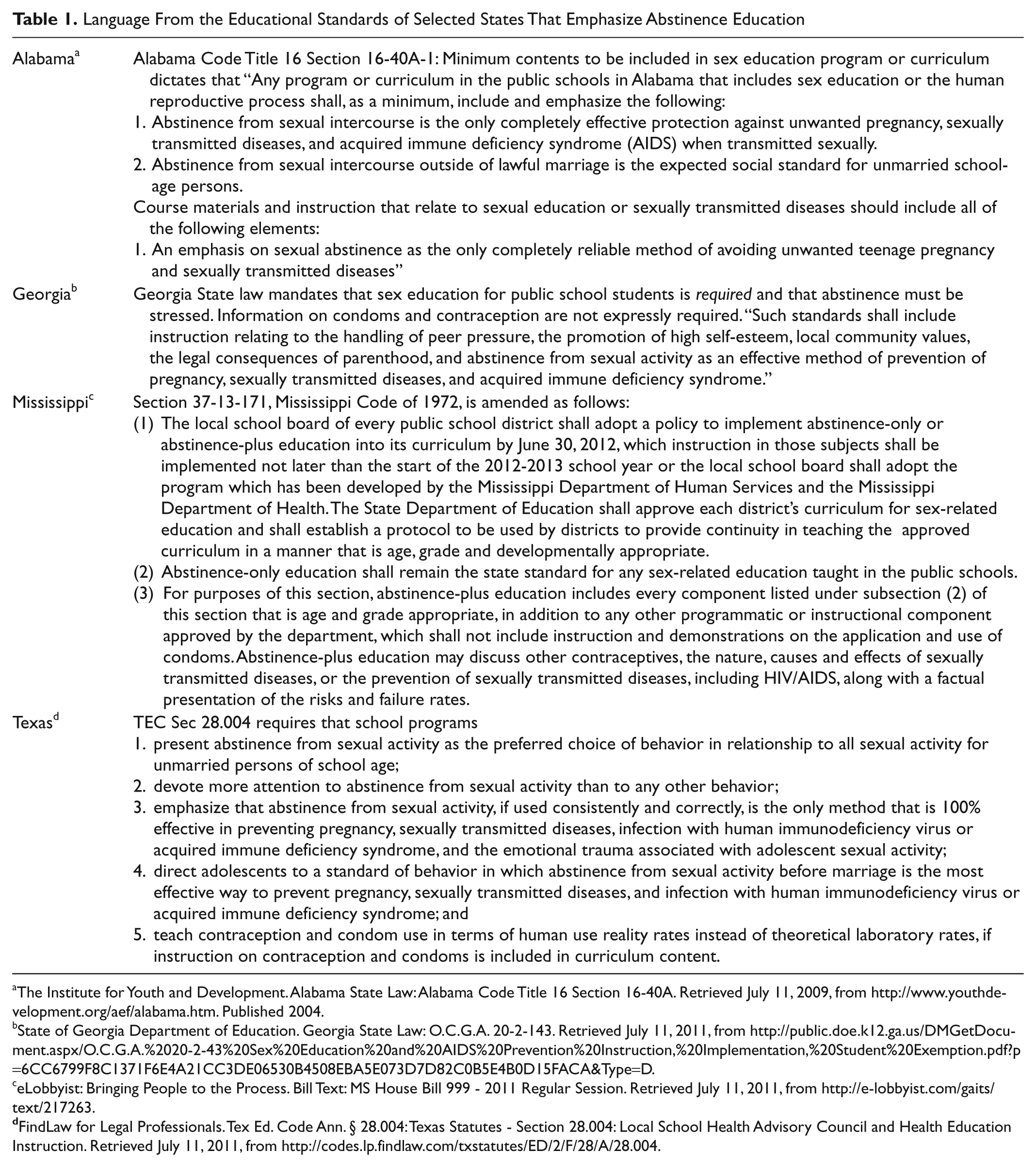
The Institute for Youth and Development. Alabama State Law: Alabama Code Title 16 Section 16-40A. Retrieved July 11, 2009, from http://www.youthdevelopment.org/aef/alabama.htm.Published2004.
State of Georgia Department of Education. Georgia State Law: O.C.G.A. 20-2-143. Retrieved July 11, 2011, from http://public.doe.k12.ga.us/DMGetDocument.aspx/O.C.G.A.%2020-2-43%20Sex%20Education%20and%20AIDS%20Prevention%20Instruction,%20Implementation,%20Student%20Exemption.pdf?p=6CC6799F8C1371F6E4A21CC3DE06530B4508EBA5E073D7D82C0B5E4B0D15FACA&Type=D.
eLobbyist: Bringing People to the Process. Bill Text: MS House Bill 999 - 2011 Regular Session. Retrieved July 11, 2011, from http://e-lobbyist.com/gaits/text/217263.
FindLaw for Legal Professionals. Tex Ed. Code Ann. § 28.004: Texas Statutes - Section 28.004: Local School Health Advisory Council and Health Education Instruction. Retrieved July 11, 2011, from http://codes.lp.findlaw.com/txstatutes/ED/2/F/28/A/28.004.
Choosing the Best (CTB; Cook, 2009) has been utilized in schools in 48 different states, although its use has been more prevalent in Southeastern and Midwestern states. More than 3 million students have participated in a CTB program since 1993. Specifically, in Georgia, 75 of its 183 districts have selected the CTB program since 1995. Georgia’s teen pregnancy rate has gone down at a higher rate than the nationwide trend over that same period, but remains alarmingly high, 36.8 per 1,000 15- to 17-year-old females (Georgia Department of Human Services, 2007). Recognizing that the co-occurrence of high rates of program use and lower rates of teen pregnancy do not demonstrate evidence, CTB sought to determine if its approach, while popular in communities seeking an abstinence curriculum, was actually resulting in the maintenance of abstinence or a return from sexual activity to abstinence.
CTB is a classroom-based curriculum, providing developmentally phased messages—for Grades 6 through 12—about the risks of sexual activity, including, but not limited to, intercourse. CTB uses medical information to emphasize the role of abstinence as the best way to prevent pregnancy, disease, and emotional consequences of sexual intercourse, as well as its role in supporting academic and other goals for future success. In accordance with the review process for all federal abstinence education grantees, CTB was reviewed and deemed “medically accurate.” One study suggested that CTB significantly affected a range of “cognitive mediators” for sexual behavior, as well as onset of sexual activity 1 year after the program (Weed & Anderson, 2005). The mediators included holding abstinence values, personal efficacy to maintain abstinence values, future orientation to goals as they relate to maintaining abstinence, independence from peer pressure, maintaining attitudes that do not justify sexual behaviors, and intentions and commitment to remain abstinent. Despite several methodological limitations, the study’s findings suggested that a more rigorous, experimental evaluation was warranted. Funding from a Community-Based Abstinence Education grant enabled CTB Inc., to conduct an independent study in 2009-2010, in which schools were randomly assigned to the program, focused on CTB Journey (Cook, 2009). CTB Journey is the component designed for the 9th grade, where abstinence education is typically taught in high school and when the majority of students report that they have not had sexual intercourse (Eaton et al., 2010). It should be noted that most large-scale studies of such school-based programs use random assignment of schools, but few are able to randomize individual students or classrooms within schools (Kirby, 2008). Such studies are very difficult to implement and are subject to contamination across students within a particular school.
Method
Participants
Study participants were 1,143 ninth graders in two Georgia school districts that had a total of six high schools, randomly assigned to intervention (four schools) or control (two schools). These two school districts were chosen because they did not already offer the CTB program, but expressed an interest in it, and were therefore willing to cooperate in a study in which some schools would randomly be assigned to the control condition. Ninth graders in control schools received their regular textbook-based health lessons (Bronson, 2009; Frideman, Stine, & Whalen, 2009), which included a discussion of abstinence, that is, the “usual care” in these districts. Ninth graders in intervention schools received the eight-session CTB Journey program, taught during health class, by trained CTB staff. The schools in these two districts, one rural and one a very large suburban district, were widely spread out from each other, and there was limited contact between students from different schools within or between each of the districts.
The pool of eligible students included approximately 2,000 ninth graders in the intervention schools and 1,000 ninth graders in the control schools. Ultimately, 1,143 students, 38% of the total eligible pool, returned parental consent to participate in the research. The rate of parental consent did not differ between the intervention and control schools. Comparison of study participants to the overall school demographics suggested that those who received consent were more likely to be female and African American from the population of ninth graders in the intervention schools, but the control group sample did not differ from the ninth graders in their schools. These differences are discussed further in the “Results” section.
Program
Unlike comprehensive sex education programs that focus on the reduction of risks due to sexual activity, CTB uses what has been termed a “risk avoidance” approach. Students in the program receive a maximum of eight, 45-min classroom sessions during their regular health classes. In those sessions, CTB teaches that abstinence from sexual activity until marriage is the best way to avoid teen pregnancy, disease, and possible negative emotional consequences, and is the best way to help students focus on academic and other future-oriented goals. CTB discusses both benefits and limitations of condoms and other forms of contraception in preventing pregnancy and STIs, in the context of promoting abstinence until marriage as the healthiest and most reliable choice. Built on the Theory of Reasoned Action and Planned Behavior (Ajzen & Madden, 1986; Fishbein & Middlestadt, 1987), CTB focuses on building intention to maintain abstinence, providing students opportunities to explore their own beliefs and values, and to understand how these are influenced by others’ beliefs. In addition, CTB is designed to help students understand how to set limits in relationships and establish refusal skills to build a sense of control and power (Albarracín, Johnson, Fishbein, & Muellerleile, 2001). Consistent with this theory, the study hypothesized that students in the CTB schools would demonstrate significantly greater increase from baseline to posttest than those in the control schools in attitudes and beliefs that support abstinence, discussions about abstinence with their parents and others whose opinions were important to them, sense of empowerment and confidence (self-efficacy) to maintain abstinence to meet their long-term life goals, and delay of sexual activity. Similarly, it was hypothesized that these significant differences would increase or be maintained at the long-term follow-up.
Instruments
In early 2009, a draft survey instrument, based on existing, new, and funder-required items, was developed by program and evaluation staff. The survey was approved by school district personnel and Boards of Education of two Georgia school districts in May 2009. It was pilot tested among 42 students from one ninth-grade class in each of the two school districts. The final survey, modified using pilot data and feedback, included items that reflected six separate scales: Proabstinence Attitudes, Proabstinence Beliefs, Empowerment/Hopefulness for the Future, Commitment to Abstinence, Parent/Child Communication, and Self-Efficacy. 1 Scales were created using the mean of the individual items for each of the six constructs. Table 2 presents the scales, sample items, and Cronbach’s alpha for each of the scales. Additional items measured abstinence intentions (likelihood of having sex within the next year, and likelihood of having sex as a teen before marriage), whether or not they had had sexual intercourse, and, if so, when was the last time. Although the curriculum focuses on a range of sexual behaviors, the evaluation specifically defined sex as “sexual intercourse or going all the way.” Due to concerns about the schools’ and communities’ sensitivity to more explicit questions, and the primary focus on abstinence behavior, the schools and researchers agreed that the survey would not include questions regarding contraceptive use among those who had had sex.
Scales, Items, and Scale Reliabilities at Baseline

Note: STD = sexually transmitted disease.
Expected direction of the scales and items is lower score, except for the Empowerment and Parent Communication scales.
Procedure
Students were surveyed 3 times—at the beginning and end of 9th grade and at the beginning of 10th grade. The evaluator met with health teachers, before the 2009-2010 school year, to elicit support in encouraging students to return consent forms. The evaluator trained data collection staff in protocols, confidentiality, and completion of cover sheet identifying information. Data collectors were CTB staff not teaching or involved in the program at those schools.
Consent forms were mailed to all 9th-grade parents, before the 1st week of school, directly from the principals, with a second request 1 or 2 weeks later. As an incentive to encourage their parents to return a consent form, students were eligible to be enrolled in a lottery for an ipod player at their school, if their parent returned a consent form. Pretests for all students who had active consent took place during August 2009, in their regular English classrooms. Students who did not have parental consent were given an alternative assignment in another location, as determined by each school’s administration. Data collectors had students place the surveys directly into an envelope, which was sealed while in the classroom, and then delivered to the project evaluator for data entry and analysis.
After all baseline surveys were completed, the evaluator used a table of random numbers to assign the six schools to a study condition. The randomization process successfully resulted in two of the three high schools in each district serving as intervention schools and one school in each district assigned to the control condition.
Collection of post and follow-up data took place in English classes, during May and October 2010 (the end of 9th and beginning of 10th grades). Teachers in control schools and CTB program staff completed a student attendance form for every session that the CTB program and textbook lessons were taught. Those data were entered by name and ID and then transmitted to the evaluator by ID only, to merge with the survey database for calculation of program dosage.
Data Analysis
Chi-square tests and t tests compared baseline means and proportions. Each participant had three measurements on the outcome variables; thus, outcome variables (continuous and binary) were analyzed using generalized estimating equation models for longitudinal data (proc genmod procedure in SAS 9.1, logit link function was used for binary outcome variables). The models included terms for treatment condition, time, a time-by-treatment interaction, and other controlling covariates—pretest scores, age, gender, race/ethnicity, and program dosage. Models were built for all students and separately for those who were virgins at pretest and for those who had had sex. A second set of models for each of the groups also controlled for pretest commitment to abstinence. This set is presented here, as commitment to abstinence improved the models, but did not influence the treatment outcomes.
The intraclass correlation coefficient (ICC) was calculated for the continuous outcomes, to study the school-level clustering effect in the analyses. The ICC overall was computed using the linear mixed-effects model with the schools as the random effects (Stanish & Taylor, 1983). The ICC for the outcome variables are all less than .01 in this study.
Results
More than a third (38%) of the ninth-grade parents gave active consent for their child to participate (n = 1,172), and 97.5% of those (n = 1,143, 756 intervention and 387 control) participated in the study. The control group sample was representative of their schools’ overall gender and race/ethnicity demographics. The intervention study sample was more likely to be female and less likely to be White than the overall demographic for their respective study schools. The total study sample was slightly more female than male (57% female), just over half were Caucasian (55%), and a third (33%) were African American. Additional descriptive information about the sample is reported in Table 3.
Baseline Sociodemographic Characteristics, Sexual Intentions, Attitudes, and Related Variables, by Treatment Condition

Significance (p value) of χ2 test of independence.
Significance (p value) of t test of difference of means between groups.
There were no significant differences between the intervention and control samples on age or gender (Table 3). There was a significant between-group difference on race/ethnicity, with the control group more likely to be White and less likely to be African American than the intervention group. Because there were significant differences between the treatment and control group on race/ethnicity, the statistical models controlled for this variable. There were no significant intervention/control group differences on pretest sexual activity or any of the scales at baseline.
At the pretest, 69.3% of the CTB group reported that they were virgins, that is, had never had sexual intercourse, whereas 72.3 % of the control group were virgins. At the posttest, 66% of the CTB group were still virgins and 63% of the control group were still virgins. By the long-term follow-up, 58% of the CTB group and 61% of the control group were still virgins, a drop of 11% from the pretest in both groups. None of the differences between groups at baseline, posttest, or follow-up were significant.
Table 4 presents the sample size (N), means at pretest, posttest, and follow-up on each of the study variables. It also presents the effect size at the posttest for the outcome variables for all students. Retention rates from pretest to post-test and from pretest to follow-up were 85% and 78%, respectively, in the intervention group, and were 81% and 69% in the control group. Analyses compared pretest gender, ethnicity, and sexual experience for those lost to follow-up between the intervention and control groups. There were no significant differences in loss to follow-up between intervention and control groups in terms of gender, ethnicity, and sexual experience.
Treatment and Control Group Means at Pretest, Posttest, and Follow-Up for Each Outcome Variable

Note: CTB = Choosing the Best.
Table 5 presents modeling results for each of the models controlling for age, gender, baseline commitment to abstinence, pretest score on each of the dependent variables, program or lesson dosage (i.e., how many lessons were received, regardless of whether they were CTB or the control textbook condition), and race/ethnicity. All the models were fitted by using the pretreatment value as a covariate in the analyses of posttreatment (both posttest and follow-up) outcomes. Thus, in the estimated models, the treatment estimates represent the treatment difference at the posttest from pretest. The treatment-by-time interaction estimates represent treatment and control group difference in terms of the change from posttest to follow-up (Fitzmaurice, Laird, & Ware, 2004).
Analyses of Group Differences in Outcome Variables for Youths in Choosing the Best and Control Groups, Including Predictor Variables
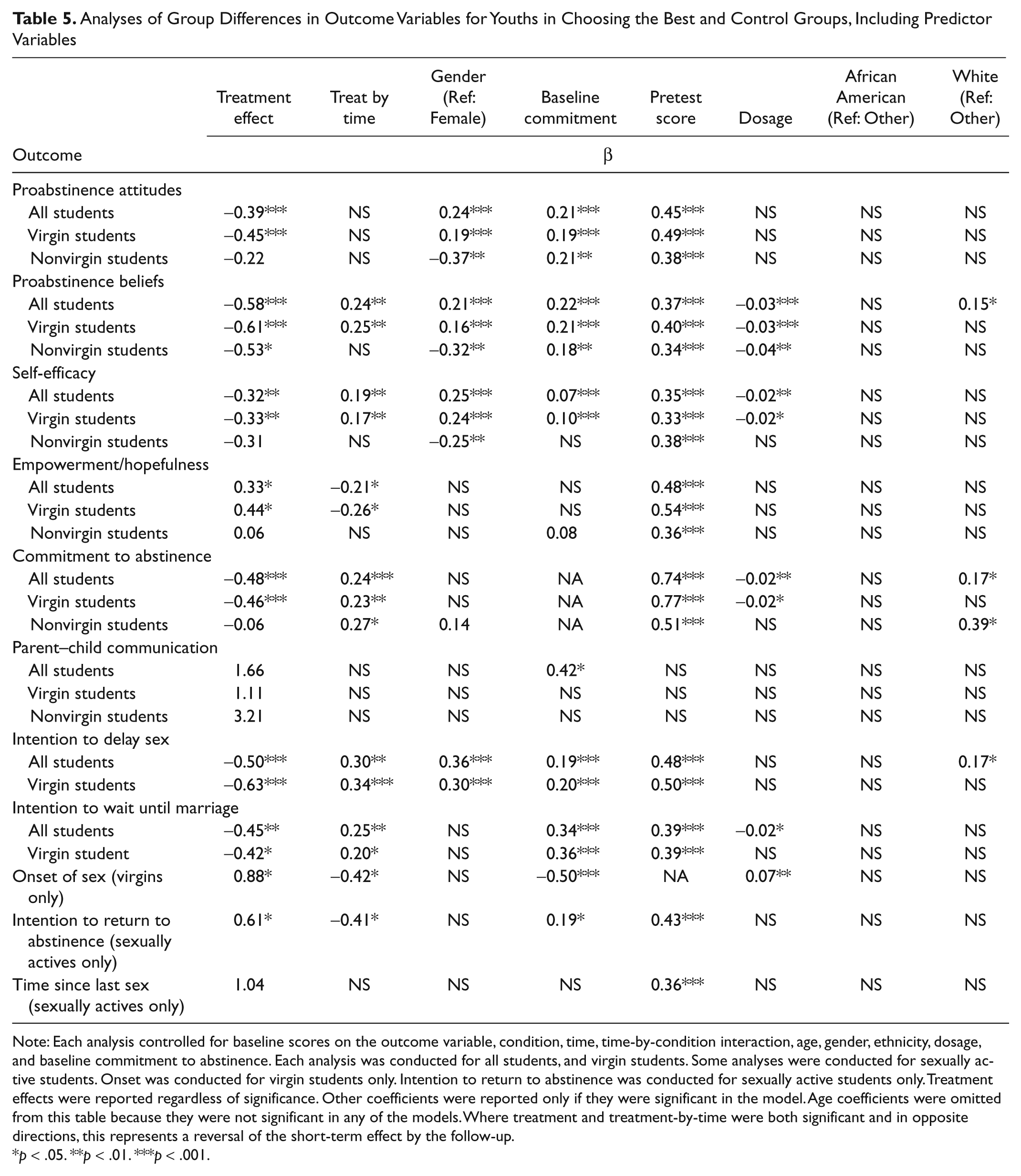
Note: Each analysis controlled for baseline scores on the outcome variable, condition, time, time-by-condition interaction, age, gender, ethnicity, dosage, and baseline commitment to abstinence. Each analysis was conducted for all students, and virgin students. Some analyses were conducted for sexually active students. Onset was conducted for virgin students only. Intention to return to abstinence was conducted for sexually active students only. Treatment effects were reported regardless of significance. Other coefficients were reported only if they were significant in the model. Age coefficients were omitted from this table because they were not significant in any of the models. Where treatment and treatment-by-time were both significant and in opposite directions, this represents a reversal of the short-term effect by the follow-up.
p < .05. **p < .01. ***p < .001.
As shown in Table 5, there were strong short-term (i.e., end of ninth grade) intervention effects on proabstinence attitudes, proabstinence beliefs, self-efficacy, commitment to abstinence, empowerment/hopefulness, intention to delay sex, and intention to wait until marriage, in both the total and the virgin student models. There was no program effect on parent–child communication about abstinence and sex. Treatment effect sizes (Table 4) at posttest ranged from a low of 0.08 to a high of 0.34, indicating relatively small to medium effect sizes on some variables, at the short term. The odds ratio of 1.43 was reported as the effect size for the binary outcome variable “onset of sex,” which can be interpreted to mean that virgins in the CTB program were nearly 1.5 times more likely to delay the onset of sex than virgins in the control group at the posttest measurement. As described below, however, these effects did not last over the longer term.
As shown in Table 5, all significant treatment-by-time interaction effects had a negative sign compared with the treatment effect, except on proabstinence attitudes, which did not have a significant interaction effect. This indicates that by the 10th-grade follow-up, all but one of the treatment effects had significantly diminished. 2
With respect to sexual onset, there was a short-term effect of treatment among those who were virgins at pretest. The statistical model (Table 5) indicates that treatment had a positive effect to “onset of sex,” indicating that the virgins in CTB group were more likely to delay sex than the virgins in the control group, when controlling for gender, baseline commitment to abstinence, dosage, and race/ethnicity at the posttest measurement.
The treatment-by-time interaction analysis, however, demonstrated that the program effect on sexual onset was not sustained at the long-term follow-up. In addition, lesson dosage (whether of the CTB program or the textbook lessons) and baseline commitment were significant predictors of sexual onset, at both short and longer term follow-up.
Among students who had already had sex by the time of the pretest, there were short-term treatment group differences on proabstinence beliefs and on intentions to “return to abstinence,” but the treatment effect on intentions had significantly diminished by the 10th-grade follow-up.
In addition to findings with respect to treatment effects, other variables were significant contributors to the desired outcomes: Gender and baseline commitment to abstinence were significant contributors to proabstinence attitudes; gender, baseline commitment to abstinence, dosage, and race/ethnicity to abstinence beliefs; gender, baseline commitment to abstinence, and dosage to self-efficacy; dosage and race/ethnicity to commitment to abstinence; baseline abstinence commitment to parent–child communication (among the total sample); gender, baseline commitment, and race/ethnicity to intention to delay sex; and baseline commitment to abstinence and dosage to intention to wait until marriage. Where gender was significant, girls’ responses were in the more “pro-abstinence” direction than boys. Where race/ethnicity was significant, White students held lower “pro-abstinence” beliefs, commitment to abstinence, and intention to delay sex than all other groups. There was no racial/ethnic difference in onset of sexual intercourse. That is, although there were racial/ethnic group differences in intentions, commitment, and beliefs, White students were no more or less likely to begin having sex than other groups.
Discussion
The study demonstrated promising short-term findings among those who had not yet had sex on a range of attitudes, beliefs, intentions, and behaviors. More specifically, analyses controlling for gender, age, race/ethnicity, pretest scores, and baseline commitment to abstinence, among virgin students, yielded significant short-term treatment group effects on intentions to remain abstinent, proabstinence attitudes, proabstinence beliefs, commitment to maintaining abstinence, self-efficacy to set and communicate boundaries in relationships, and sense of power in reaching future goals. Among the sexually active group, there were significant short-term program effects on beliefs and intentions only. Although the program did include parent–child homework activities in an attempt to expand the school curriculum’s reach to parents, there was no program effect on parent–child communication about abstinence and sex among either virgin or sexually active students, suggesting the need to strengthen efforts to directly engage parents.
CTB students who were virgins at the pretest were nearly 1.5 times more likely to delay onset of sexual behavior by the end of the 9th grade, a difference, however, that was not sustained by the beginning of the 10th grade. CTB students who had already had sex were more likely than the control group to report an intention to return to abstinence at the posttest, but there was no treatment group impact on time since last sex, and the effect on intentions to return to abstinence was not sustained by the 10th-grade follow-up. Notably, among these 9th graders, more than one in four reported that they had already had sex, reflecting significant risks by the beginning of high school.
Thus, some of the study hypotheses were supported, whereas others were not. Students in the CTB groups showed significantly greater increase in abstinence attitudes and beliefs, intentions to maintain abstinence, and delay of sexual behavior at the posttest. Hypotheses related to empowerment and parent communication, however, were not supported, and at the long-term follow-up, only the hypothesis regarding abstinence beliefs was supported, but not those related to other predictors, to intentions, or to sexual behavior. For those that were supported, effect sizes were relatively small, but these are consistent with other studies of abstinence programs (Kirby, 2008).
The CTB program, when taught by professional staff, appeared to be more effective than a typical classroom textbook-based program on ninth-graders’ attitudes, beliefs, intentions, and behavior at the short-term posttest. The program’s impact on proabstinence attitudes and commitment to abstinence for virgin students are notable. One longitudinal study of sexually abstinent adolescents found that conservative values contributed to the ability of adolescents to persist in sexual abstinence (Blinn-Pike, Berger, Hewett, & Oleson, 2004), and another suggested that holding a strong commitment to abstinence may contribute to maintaining sexual abstinence (Buhi, Goodson, Neilands, & Blunt, 2011). A study of virginity “pledges” (i.e., a formalized commitment to remain abstinent until marriage) demonstrated that, under certain very limited circumstances, adolescents who had taken an abstinence pledge remained virgins longer than those who had not (Bearman & Bruckner, 2001). These data suggested that virgin students in the program increased both proabstinence attitudes and commitment to abstinence. Their relationship to intentions and behavior, however, are not clear, as the short-term treatment effect on both intentions and sexual onset were not sustained at the longer term follow-up.
Students received a maximum of eight, 45-min sessions, for both the CTB program and the regular textbook health lessons focused on abstinence in one school year. The CTB program, by design, is intended to be offered in a sequenced multiyear format (Cook, 2009). Unfortunately, school districts are often unable to provide the entire scope and sequence in such multiyear programs, given pressures to fulfill more mandates across primary academic participants (Tappe, Allensworth, & Grizzell, 2010). The lack of long-term impact of the program may illustrate what is known about the challenges of school-based health interventions, which may not last a sufficient number of hours, be reinforced over multiple grade levels (Connell, Turner, & Mason, 1985), and/or are not maintained in schools over time, to achieve sustained attitude and behavior change (Smith, Redican, & Olsen, 1992). The finding that higher dosage of either program was associated with some positive outcomes further suggests the importance of classroom time and reinforcing messages, regardless of the approach.
Questions about the impact, positive or negative, of abstinence education programs on students who are already sexually active have been raised in the literature (Santelli et al., 2006; Wiley, 2002). Although the majority of students in the ninth grade are not yet sexually active, nearly one in four of this study population reported that they had already had sex by the time of the pretest. Among those students, the study findings were limited to short-term abstinence beliefs. This study tested only the impact of the single-year CTB program in the ninth grade; thus, it did not address the potential cumulative impact of a program that is designed to begin in the sixth grade, when nearly 95% of students would not yet have had sex (Eaton et al., 2010).
Limitations
The study compared the CTB abstinence-focused curriculum taught by its own professional staff with a typical health class textbook-based approach that contained lessons about abstinence, that is, the “usual” intervention in these high schools. Thus, it was not an attempt to compare CTB with other philosophical or practical approaches, nor to make the case for abstinence education overall.
An experimental study that included more schools was not feasible, given the myriad challenges of school-based research, for example, concerns at the district level about randomization, sensitivity of the subject matter, that is, sex, and limited instructional time, thereby creating hesitancy to use classroom time for survey research. The study used the most feasible design, randomization at the school level, involving two districts with supportive administrators who agreed to maintain two schools as control schools for the duration of the study. This design eliminated the threat of contamination within schools, and the schools’ level of cooperation resulted in a study in which treatment groups and protocols were successfully maintained. The analyses took clustering into account, as a way to address randomization by school, but the total number of school units was still relatively low. The complexity and cost of including large numbers of units (i.e., schools) in randomized studies is a significant challenge and limitation of most school-based research.
Baseline and follow-up data were collected at the beginning and end of the school year, at the same time for all study participants. Students in the study, however, took ninth-grade health in either the fall or spring. They were scheduled for fall or spring health class by computer; thus, there were no systematic demographic or academic differences that might be associated with sexual behavior variables between students who received the program in the fall or spring. This method resulted in high rates of survey completion among eligible students and also accounted for maturational differences between students who had health in the fall or the spring of ninth grade. The scheduling did result, however, in varying follow-up periods, with posttests ranging from 3 months for those who had health in the spring semester to 6 months for those who had it in the fall. Consequently, longer term follow-up was a range of 7 to 10 months. Ultimately, the ability to gather more data and to control for maturation by conducting all surveys at the same points was considered by the researchers to outweigh the disadvantage of the variable follow-up periods. This is, however, a significant limitation of the study and makes estimation of the length of time that the program impact “lasts” nearly impossible.
Behavioral data were limited to self-reports, as most studies of this type. Monitoring pregnancies within each of the school districts would have offered additional objective information. Furthermore, questions about contraception and condom use among students who were already having sex were not able to be asked. Both the intervention and the study, itself, were relatively short term, following students who had received a maximum of eight class sessions in the ninth grade through the beginning of tenth grade. Thus, if generalized, application of the findings must be limited to single-year programs and relatively short-term outcomes, and within communities that are already supportive of an abstinence education approach, as these study school districts were.
Conclusion
In a randomized study design, with schools as the unit of randomization, the study demonstrated that, in two communities that supported and sought an abstinence-focused approach, CTB “Journey” resulted in significant short-term impact on ninth-graders’ commitment to abstinence, proabstinence beliefs and attitudes, and intentions to remain abstinent. Among pretest virgins, there was a lower onset of sexual intercourse by the end of ninth grade. Among students already sexually active, there was a short-term treatment effect on intentions, but not sexual behavior. The study was designed to determine the effectiveness of the CTB abstinence education curriculum, as compared with the typical health textbook approach to discussion of abstinence. It was not designed to study the overarching question of whether abstinence education is more or less effective than other approaches. Rather, it was designed to test the effectiveness of this curriculum on a range of outcomes, within two communities that sought an abstinence message for their high school students and which were within a state that requires an abstinence emphasis.
As educational theories and data demonstrate, long-term changes in skills, attitudes, and behaviors are rarely achieved with short-term approaches, but require repetition, reinforcement, and increasing complexity. The CTB program was designed for developmentally phased and sequenced lessons in multiple grades. This study measured a single-year’s intervention only and demonstrated positive short-term effects on ninth graders who were not yet sexually active. Future studies should include multiple years of intervention, beginning in earlier grades, to determine if this particular abstinence program can demonstrate a longer term impact on sexual activity.
Footnotes
Acknowledgements
Special thanks to the students, teachers, administrators, and parents who participated in this research; to Betsy Birkholz, Director, and to the staff of Choosing the Best Inc., for assistance in the planning and implementation of the study; and to Kayla Ryan and Tahira Randhawa, graduate students at Montclair State University, for assistance in the preparation of this manuscript.
Institutional Review Board (IRB) approval for the pilot phase and for the full research study was received from the IRB at the University of Florida in April 2009 for the survey development and July 2009 for the full study.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Funding for this study was provided by the Administration for Children Families and Youth (ACFY), the Family and Youth Services Bureau, Grant No. 90AE0273/01.