
Abstract
The life course perspective and cumulative inequality theory suggest that childhood adversity, occurring during a sensitive period of the life course, can have long-term consequences for adult mental health and well-being. Yet, the long-term influence of adversity on adult outcomes may depend on both the features of adverse childhood experiences (e.g., the number, type, and co-occurrence of adversities) as well as the outcome assessed. Using latent class analysis applied to several waves of prospective data from the Great Smoky Mountains Study (GSMS; N = 1,420), we identify subpopulations that are similar in their adversity experiences before age 18. We then predict adult internalizing and substance use disorder diagnoses by adversity experience. Results reveal five distinct classes of adversity, with unique risks for specific diagnoses in adulthood.
Introduction
The life course perspective and cumulative inequality (CI) theory (Ferraro and Shippee 2009) suggest that early life experiences are important predictors of life course health and well-being, and extensive research cites the particular role of childhood adversity in shaping adult mental health (Copeland et al. 2018; Ferraro and Wilkinson 2013). Childhood adversity here refers to traumatic or stressful experiences occurring before age 18 such as those identified in the original adverse childhood experiences (ACEs) study (Felitti et al. 1998), falling under the umbrellas of abuse, neglect, and household dysfunction. Research on childhood adversities has yielded several important findings, including that adversities are not rare (Felitti et al. 1998; Merrick 2019); adversities seldom occur in isolation; and multiple exposures to adversities are more detrimental to health than a single exposure (Barboza 2018). These findings are important as the mental health consequences of childhood adversity can range across a host of disorders (e.g., substance abuse, depression, and anxiety) (Merrick 2019), all of which may impact one’s quality of life and may spillover to impact one’s ability to achieve normative expectations of adult roles, relationships, and attainment (George 2013).
Despite gains made in connecting adversity to health outcomes, this inquiry has been clouded by inconsistency in the measurement of childhood adversity (Heidinger and Willson 2019; Wang et al. 2022) and a history of research operationalizing childhood adversity as the summation of negative experiences (see Lian, Kiely, and Anstey 2022 for recent discussion). Although informative, a summative approach assumes that each adversity is equally relevant when evaluating the risk for poor adult outcomes and does not allow for consideration of the influence of qualitatively distinct sets of adversity. The impact of childhood adversity on adult mental health is not always certain (Ferraro and Shippee 2009) and the magnitude of the impact may depend on these important aspects of adversity experience (Kamis 2020; Schafer and Ferraro 2013).
Therefore, researchers have increasingly called for the use of alternate approaches, such as latent class analysis (LCA) (Barboza 2018; Curran et al. 2018; Heidinger and Willson 2019; Lian et al. 2022; Wang et al. 2022) to capture both the type and the number of adversities experienced when assessing whether childhood adversity predicts adult outcomes. LCA allows for the identification of subpopulations that are similar in their responses to a set of indicators—in this case, experiences of childhood adversity—without a priori distinctions made by the researcher (Barboza 2018). In addition to distinguishing adversity experience, identified subpopulations (“classes”) represent how adversities commonly cluster in the real world, enabling important epidemiologic insight into multiple adversity exposure and providing intervention points for reducing the public health burden of adversity and subsequent poor mental health.
This study, situated within the life course perspective and drawing from CI theory, follows past studies employing LCA to examine whether the link between childhood adversities and adult mental health outcomes is dependent on the number and type of co-occurring experiences. Using prospective data from the Great Smoky Mountains Study, we identify subpopulations that are similar in their adversity experiences before age 18. As past research suggests that adversity predicts a host of mental health outcomes (Merrick 2019), but that unique adversity experiences may be more predictive of certain disorders (Giano et al. 2021; Kim et al. 2021), we include several internalizing mental health and substance use disorder outcomes based on diagnostic interviews. In addition to considering several outcomes, this study extends past work in several ways. We use prospective, as opposed to retrospective, measures of childhood adversity that are captured over several years of childhood and are based on both child and parent reports. These reports avoid potential recall biases of retrospective reports and leverage the strengths of both self- and parent-reported events (Brewin, Andrews, and Gotlib 1993; Hardt and Rutter 2004). Furthermore, guided by recent arguments to expand the inclusion of adverse childhood experiences beyond those listed in the original ACEs study (Felitti et al. 1998) to additional major childhood stressors across several domains (Finkelhor 2018; Kysar-Moon 2020), we include a broader set of measured adversities. Overall, this work contributes to research on the life course and CI theory by clarifying how adverse experiences co-occur in childhood, and how configurations of these experiences relate to disparate mental health diagnoses in adulthood.
Childhood Adversity and Adult Mental Health
The life course perspective and CI theory (Ferraro and Shippee 2009; Ferraro and Wilkinson 2013) frame early life as a sensitive period for emotional, physical, and mental development (Dunn et al. 2018), meaning that traumatic, stressful experiences during early life may have a significant and lasting impact on health and well-being. CI theory posits this may occur because negative experiences and situations often occur in tandem (i.e., clusters of risk) and predict future exposure to risk (i.e., chains of risk). Conversely, advantaged life experiences augur more positive trajectories (Ferraro and Shippee 2009). In the context of childhood adversities, CI theory would suggest that those exposed to these stressful early life conditions are at greater risk of experiencing additional adversities within childhood and subsequent disadvantages as individuals age into adulthood with consequences for mental health, while those who do not have childhood adversity will have life trajectories more conducive to the accumulation of resources that promote mental health. Although not the focus of this article, it is also important to highlight that CI theory recognizes that exposures to these early life stressors are patterned by macro systems of inequality, such as structural racism and sexism, that put certain children (e.g., girls, Black children) at greater risk of experiencing adversity (Ferraro and Shippee 2009; Kysar-Moon 2020). Nevertheless, the accumulation of risk for some and resources for others leads to diverging mental health outcomes across the life course, and thus adult mental health disparities.
Psychological work on childhood adversity likewise supports this accumulation of risk and resources, finding that childhood adversity in early life can inhibit learning processes, such as fear and reward learning (McLaughlin and Sheridan 2016). Poor programming of fear and reward learning can increase reactivity to stressors, decrease recognition of rewards, and/or harm executive functioning, each of which can influence one’s ability to maintain good mental health in early life and beyond (McLaughlin and Sheridan 2016). At the same time, childhood adversity may shape adult mental well-being through initial increases in symptomology or substance use experienced at the time of the stressors that are enduring (Schafer and Ferraro 2013). Together, these social and psychological indirect and direct pathways combine to link stressful and traumatic early life experiences to symptoms and disorders across the life course.
Yet, CI theory also posits that life trajectories are not entirely based on early life experiences and that individuals may offset the negative impacts of early life through human agency and resource mobilization, resulting in a null relationship between childhood adversity and adult mental health (Ferraro and Wilkinson 2013). Related work suggests that simply the waning salience of early life may lead to a decrease in mental health disparities between those who have and have not experienced adversity (Kamis 2020; Schafer and Ferraro 2013). Therefore, the long-term influence of childhood adversity on adult mental health is not certain, and growing research has suggested that features of the adversity experience (i.e., number, type, and configuration of adversities), as well as the mental health outcomes measured, may shape whether there are significant life-course mental health consequences (Giano et al. 2021; Kim et al. 2021).
Distinguishing Adversity Experiences and Mental Health Outcomes
Research focusing on the heterogeneity of childhood adversity has highlighted how experiences can differ in the number and type of adversity exposures, in addition to which adversities co-occur. For example, research employing LCA finds that socioeconomic adversities (e.g., low parental education, poverty status) tend to cluster together (Wang et al. 2022), whereas the co-occurrence of dysfunctional household experiences (e.g., parental substance abuse, household conflict, and parental depression) emerges as a separate subtype of adversity (Barboza 2018; Lian et al. 2022). Experiences of abuse and neglect, often referred to as maltreatment, likewise tend to occur concurrently, but can also be found in tandem with other types of adversities (Barboza 2018).
These different configurations of adversities may influence adult internalizing disorders, such as depression and anxiety, and/or externalizing disorders (Merrick 2019; Wang et al. 2022). Here, we focus specifically on substance use disorders as a subset of adult externalizing disorders and note that although related, each mental health disorder has a unique etiology and there is evidence to suggest that specific types of adversity are more predictive of certain adult disorders.
Studies examining internalizing disorders have noted that child abuse, as opposed to unstable family structure (e.g., divorce, death, and lack of a male figure) or financial strain, is associated with increased somatic and psychological responses in adulthood (Schafer and Ferraro 2013). Similarly, Giano and colleagues (2021) found that experiencing both family mental illness and abuse is associated with the greatest likelihood of depression diagnosis in adulthood compared to all other domains of adversity. These findings support theories that suggest experiences of abuse or violence will have the strongest relationships with depression and/or anxiety due to the emotional reactivity associated with these high-threat exposures (McLaughlin and Sheridan 2016). Work that has more explicitly compared several internalizing outcomes has also noted that socioeconomic deprivation experiences are more predictive of anxiety as opposed to depressive outcomes (McGinnis, Sheridan, and Copeland 2022).
For substance abuse, Kim and colleagues (2021) noted that abuse and parental substance use have been found to increase the likelihood of adult substance use, highlighting the intergenerational transmission of this disorder. Theories on household dysfunction also suggest that childhoods marked by neglectful or unsupportive parents may lead to unsupervised environments that particularly encourage substance use, setting proclivities that extend into adulthood (Repetti, Taylor, and Seeman 2002). Although these and other studies often collapse substance use disorders into a single outcome (any disorder), studies that examine heterogeneity within substance use outcomes have found that abuse is more strongly related to drug use disorders and that parental discord and violence are more related to alcohol use disorders (Leza et al. 2021). However, there is also tentative evidence that alcohol use, as compared to drug use or other mental health outcomes, may be less influenced by adversity generally (McGinnis, Sheridan, and Copeland 2022).
Although the studies reviewed here provide evidence for differential links between types or clusters of adversity and mental health outcomes, theoretical reasoning for why specific configurations of adversity relate to certain outcomes is complex due to the multitude of pathways that may connect each adversity to each mental health disorder. Although we do not cover all potential hypotheses here, we note that the accumulation of risks hypothesized by CI theory (Ferraro and Shippee 2009) may help clarify why some early life experiences are found to be harmful across all outcomes. For example, more severe adversities, such as abuse, may be broadly damaging due to the connection of abuse with a multitude of adulthood stressors (e.g., interpersonal and economic strain) that can accumulate and lead to several mental health disorders (Schafer and Ferraro 2013). This model may also explain why those with the greatest number of adversities, and thus the greatest accumulation of risks across several early life domains, are often found to be at the highest risk of all internalizing and substance use disorders (Barboza 2018; Merrick 2019).
In sum, evidence suggests that the relationship between childhood adversity and adult mental health may be varied, depending on the features of the adversity experience and the health outcome measured. In this study, we build on the growing body of work employing LCA to investigate both the number and types of adversities that co-occur in childhood. We include a wide range of prospective measurements of childhood adversities (both parent and child reported) before age 18 and examine how classes of childhood adversities predict several adult mental health disorder diagnoses, allowing for increased precision in the estimation of how early life influences adult outcomes. In doing so, this work clarifies the long-term risks of childhood adversity on mental health, contributing to research on stress, childhood, life course, and aging.
Data and Methods
Data
Data for this study come from the Great Smoky Mountains Study (GSMS). The GSMS is a longitudinal study representative of children in 11 predominately rural counties of North Carolina. For the first wave of GSMS (1993), three cohorts of children (ages 9, 11, and 13) were selected from a pool of 20,000 children to yield a sample of 1,420 children. The children were then surveyed every year until age 16 and then again at ages 19, 21, 25, and 30 (Costello, Copeland, and Angold 2016). American Indian participants and those screened as being at high risk for psychopathology were oversampled. Sampling weights are applied to adjust for the differential probability of selection into the sample, allowing estimates to be representative of this population despite oversampling (Copeland et al. 2018). For all assessments up until age 16, both parent and child signed informed consent/assent forms approved by the Duke University Medical Center Institutional Review Board (IRB). Only the child was interviewed, and thus consented, after reaching adulthood. Although not a U.S. representative sample, the GSMS provides a unique opportunity to study several years of parent and child prospective reports of a large range of childhood adversities, discussed further below.
Measures
Childhood adversities
The original ACEs study (Felitti et al. 1998) included measures of abuse, neglect, and household dysfunction (e.g., parental incarceration, divorce, mental illness, etc.) before age 18 to capture childhood adversity experience. However, recent work suggests that additional stressful events in childhood can have both short- and long-term consequences for well-being (Finkelhor 2018). Here, we follow past work using the GSMS (Copeland et al. 2009, 2018) and consider a more comprehensive list of childhood adversities that includes socioeconomic disadvantage and stressful life events (e.g., being bullied, experiencing the death of a loved one, and exposure to unsafe environments). We also include a broader range of familial characteristics, covering parenting behaviors (e.g., parents acting harsh, acting overinvolved, scapegoating child, and providing inadequate supervision), the relationship between child and parent (e.g., tension and fighting), and interparental conflict (e.g., dissatisfaction, arguing, and apathy). These characteristics are potentially less severe than those captured in the original ACEs study, but such exposures have been linked to mental health outcomes (Bevilacqua et al. 2021; Wilkinson and Andersson 2019).
All childhood adversity measures were obtained using the structured Child and Adolescent Psychiatric Assessment (CAPA), except for maternal depression (Angold and Costello 2000). For some childhood adversities, respondents were asked each wave if they had ever in their lifetime experienced the event. Lifetime assessments were limited to events labeled as high magnitude in past work on posttraumatic stress disorder (Costello et al. 1998) that are more likely to be recalled. All other adversities were those commonly included in life event scales related to research on depression and anxiety (Costello et al. 1998). To ensure adequate recall of other childhood adversities, respondents were asked each wave whether, in the past three months, they experienced the event (Coughlin 1990). All measures of childhood adversities were measured using both parent and child reports. An adverse experience is indicated when either the parent or the child affirmed the occurrence of an event at any wave through the age of 16 (before age 18). Additional details of the CAPA measurement are described elsewhere (Costello et al. 1998).
We include 21 total measures of childhood adversity. For the sake of clarity, we group these measures into broader categories of Family Characteristics, Parental Risk Factors, Socioeconomic (SES) Disadvantage, and Stressful Life Events. The complete list of measures used with additional information is included in Supplemental Appendix A.
Adult diagnoses
All adult diagnoses were assessed using the Young Adult Psychiatric Assessment (YAPA), which is an extension of the CAPA (Angold and Costello 1995; Angold and Cox 1997), and uses structured clinical interviews grounded in the Diagnostic and Statistical Manual (DSM-5) classifications system. Diagnoses are indicated when a respondent meets the criteria for a given disorder at any assessment during adulthood (age 18+). The internalizing and substance use disorder diagnoses considered in analyses are depression (including major depressive disorder, dysthymia, and depressive disorder, not otherwise specified), anxiety (generalized anxiety disorder, overanxious disorder, obsessive-compulsive disorder, panic disorder, agoraphobia, simple phobia, and social phobia), alcohol use disorder (alcohol abuse/dependence), cannabis use disorder (cannabis abuse/dependence), and other illicit drug use disorder (abuse/dependence of cocaine, methamphetamines, inhalants, heroin, hallucinogens, and/or sedatives).
Background variables
Cohort captures whether a respondent was part of the Young (ref.), Middle, or Old cohorts representing children ages 9, 11, and 13 at Wave 1, respectively, to control for potential differences in experiences across cohorts. Because experiences with childhood adversity and mental health outcomes are patterned by macro systems of inequality (Ferraro and Shippee 2009), we adjust for this differential exposure by including a control for gender as a binary indicator (female [ref.] or male) and a control for race as a set of indicators for whether a respondent is Black, American Indian, or White (ref.).
Analytic Strategy
We employ LCA to identify both the number of and characteristics of relatively homogeneous subpopulations (“classes”) that comprise the overall population and examine whether these classes predict adult disorder diagnoses. In the first step of analyses, we estimate an unconditional latent class model, meaning that only adversity indicators are included in the model. A key component of LCA is determining the appropriate number of classes based on several goodness-of-fit indicators that balance parsimony with explanatory power. We determined the number of latent classes by comparing Bayesian Information Criteria (BIC), entropy (i.e., class separation, above .6), size of the smallest class (>5 percent), and substantive differences between classes (see Weller, Bowen, and Faubert 2020).
In the second step, individuals are assigned to latent classes using their highest posterior probability of membership. Because class membership is not exact (individuals typically have a non-zero probability of belonging to each class), there is the potential for misclassification in this step. Thus, in the third step, when class membership is used to predict our outcomes of interest, we adjust for this potential misclassification by employing the BCH method (eponymously named for Bolck, Croon, and Hagenaars 2004), a multi-step approach for associating latent classes with distal outcomes. The BCH method adjusts for potential misclassification with the inclusion of estimation weights obtained from the inverse matrix of the misclassification probabilities that are produced under the unconditional LCA. These weights are explicitly incorporated when modeling the relationship between indicators of class membership and adult diagnoses, controlling for relevant covariates. Several simulation studies have noted that the BCH method is preferable to alternate multi-step (or one-step) methods that associate latent classes with distal outcomes (Bakk and Kuha 2021; Nylund-Gibson, Grimm, and Masyn 2019).
Although the initial unconditional LCA is the same for all models, we estimate separate models for each outcome. Because the outcomes of interest are binary (does/does not meet criteria for diagnoses), the relationships between covariates and outcomes are modeled using logistic regression. Predicted probabilities are calculated holding covariates at their mean values and therefore represent the probability of meeting criteria for diagnoses for each latent class. The statistical significance of latent class differences in the outcomes are assessed by examining differences in coefficients using Wald tests. All models are estimated in Mplus and are adjusted for sampling design. We employ the manual, as opposed to automated, BCH method in Mplus for increased flexibility (see Nylund-Gibson et al. 2019).
The full sample (N = 1,420) was used for assessing latent classes of adversities. However, some attrition occurred as respondents entered adulthood (n = 86) and therefore these individuals were not included in the assessment of adult outcomes (adult sample N = 1,334). The respondents who were not included were more likely to be male and less likely to be American Indian, but had on average experienced fewer adversities compared to those included in adult analyses. There were no missing data on the covariates and because childhood adversity variables were coded as any occurrence across several waves, missingness was low for these indicators. The highest rate of missingness for any childhood adversity was 3.7 percent for Maternal Depression and 3.4 percent for Interparental Violence. Missingness on indicators is handled using the full information maximum-likelihood (FIML) estimation method in Mplus.
Results
Table 1 includes weighted descriptive statistics for study variables. As shown in Table 1, tension between the child and parent, frequent parent-child arguing, and interparental conflict (poor communication, arguing, apathy) are some of the most common adversities, with more than half of respondents indicating these experiences before age 18. Conversely, interparental physical violence and living/attending school/working in an unsafe environment are the least common adversities, occurring among less than 10 percent of the sample.
Weighted Descriptive Statistics. Great Smoky Mountains Study (GSMS; N = 1,420).

Adult diagnoses differed in prevalence across the sample. The most prevalent diagnosis was alcohol use disorder, with 20.3 percent of the sample meeting this criterion during adulthood, and the least prevalent was other drug use disorder (6.7 percent). Both cannabis use disorder and anxiety disorder had middling prevalence with approximately 17.0 percent of the sample meeting diagnostic criteria during adulthood for either disorder. The prevalence of depressive disorder was less than cannabis use and anxiety at around 10.3 percent.
Latent Classes of Adversity
Results from the unconditional LCA suggest that a 5-class model provides the best fit for the data while maintaining substantive clarity (see Supplemental Appendix B for fit statistics). Although 6-class and 7-class models had slightly smaller BIC values, they also included smaller classes (just above 5 percent of the sample) that were not substantively distinct from classes defined in the 5-class model; therefore the 5-class model was preferred. An 8-class model also had a smaller BIC but was not considered because it yielded an extremely small class (<2 percent of the sample). Our 5-class model, and the resulting substantive makeup of classes, overlaps closely with past work that has used the GSMS to define classes of adversity (see Copeland et al. 2009), even with this study including more waves of prospective measurements.
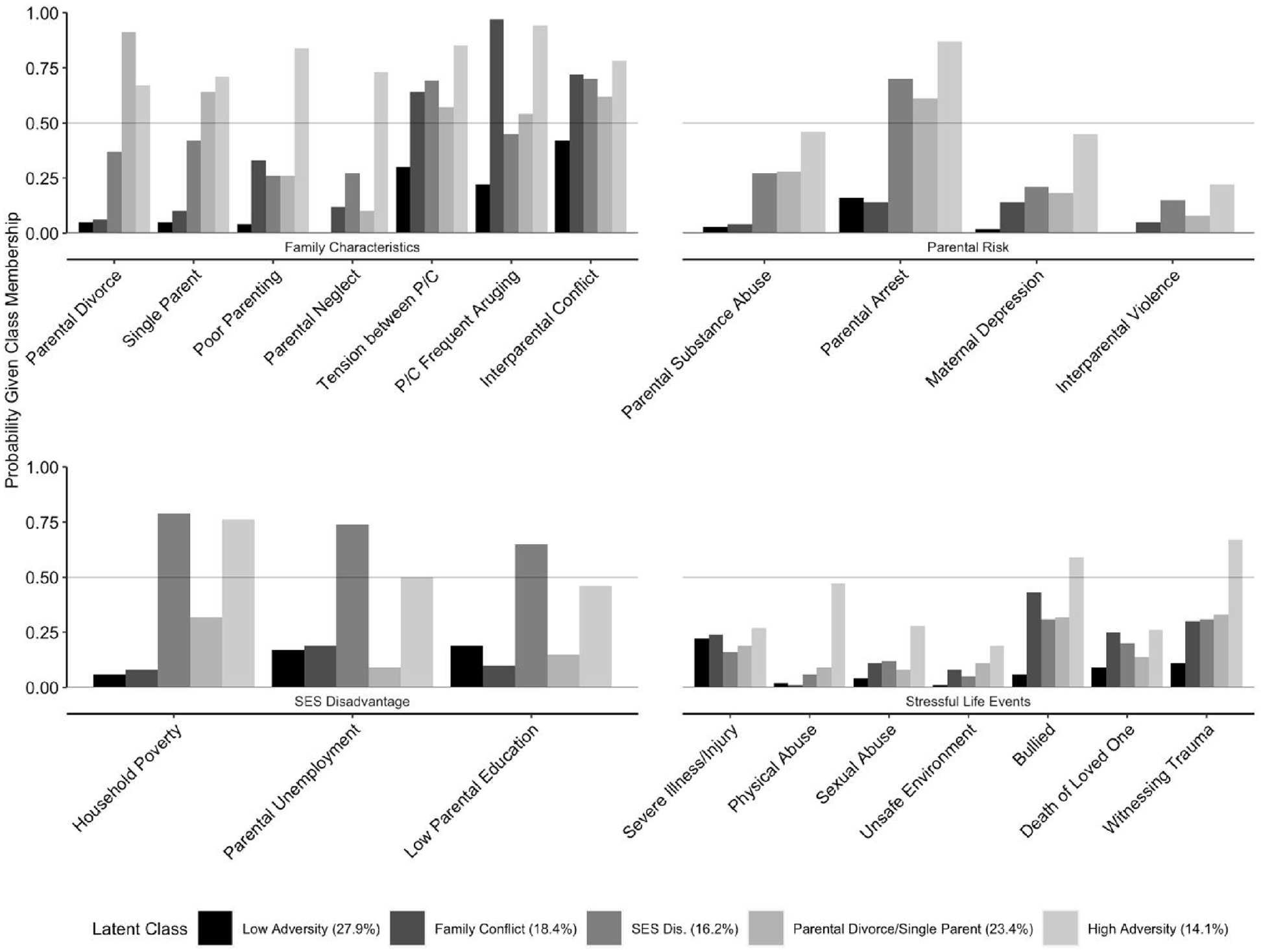
Figure 1 shows the results from the 5-class model. Like past research (Barboza 2018; Curran et al. 2018; Heidinger and Willson 2019), a sizable proportion (27.9 percent) belongs to a “Low Adversity Class” (Class 1), in which members have a low prevalence of most adversities (average number of adversities = 1.70), and no item endorsement probability greater than 50 percent. That is, in this class, the probability that a member experienced a particular adversity was less than 50 percent for all adversities measured. We call the second class (18.4 percent of respondents), the “Family Conflict” class (average number of adversities = 5.40), because its members evidence a high prevalence of parent-child conflict, tense parenting, and interparental problems. The remaining three classes similarly had a high prevalence of tense parenting and interparental problems, but also a high prevalence of other types of adversities. Classes 3 and 4 had about six adversities with an item endorsement probability of greater than 50 percent and a somewhat similar average number of adversities (7.97 and 6.38, respectively). However, these classes differed in the types of adversities experienced. Class 3 (16.2 percent of respondents), the “Socioeconomic (SES) Disadvantage” class, includes respondents who experienced a high prevalence of poverty, parental unemployment, a parent without a high school degree, and parental arrest. Class 4 (23.4 percent of respondents), the “Parental Divorce/Single Parent” class also had a somewhat heightened prevalence of parental arrest, but especially high item endorsement probability of experiencing parental divorce and single parenthood and low endorsement probability of socioeconomic disadvantage.
Results from the unconditional latent class model.
The final class, Class 5 (14.1 percent of respondents), is labeled the “High Adversity” class as this class has an item endorsement probability of greater than 50 percent for 12 adversities and an average of 12.86 adversities. Notably, this group has a high prevalence of several adversity experiences not prevalent in other classes, including being bullied, witnessing trauma, poor parenting, and parental neglect, and an elevated prevalence of both physical and sexual abuse.
Ancillary analyses that examined the composition of the five classes suggested that there were no differences in gender composition, with all classes having approximately 50 percent females. However, there were significant differences in the racial composition of classes. The Low Adversity and the Family Conflict classes had a higher proportion of White respondents compared to the High Adversity and SES Disadvantage class (p < .05), with approximately 95 percent of respondents identifying as White in either class. The SES Disadvantage class had the highest proportion of Black respondents (14.9 percent; significantly different than Low Adversity, p < .05) and American Indian respondents (9.7 percent; significantly different from all other groups, p < .05). The High Adversity class had the next highest proportion of American Indian respondents (4.8 percent; significantly different from all other groups, p < .05).
Latent Classes of Adversity and Adult Diagnoses
Table 2 presents results predicting diagnoses by latent class of adversity, controlling for cohort, race, and gender. For both internalizing (depressive and anxiety) disorders (Models 1 and 2, Table 2), the High Adversity class has much greater odds of meeting the criteria for diagnoses (7.57 and 6.40 times, respectively) compared to the Low Adversity class. The Family Conflict class has 4.72 times greater odds than the Low Adversity class of experiencing depressive diagnoses but does not differ from the Low Adversity class in odds of meeting the diagnostic criteria for an anxiety disorder.
Odds Ratios and 95 Percent Confidence Intervals for Models Predicting Meeting Diagnostic Criteria by Adult Mental Health Disorder. Great Smoky Mountains Study (GSMS; N = 1,334).
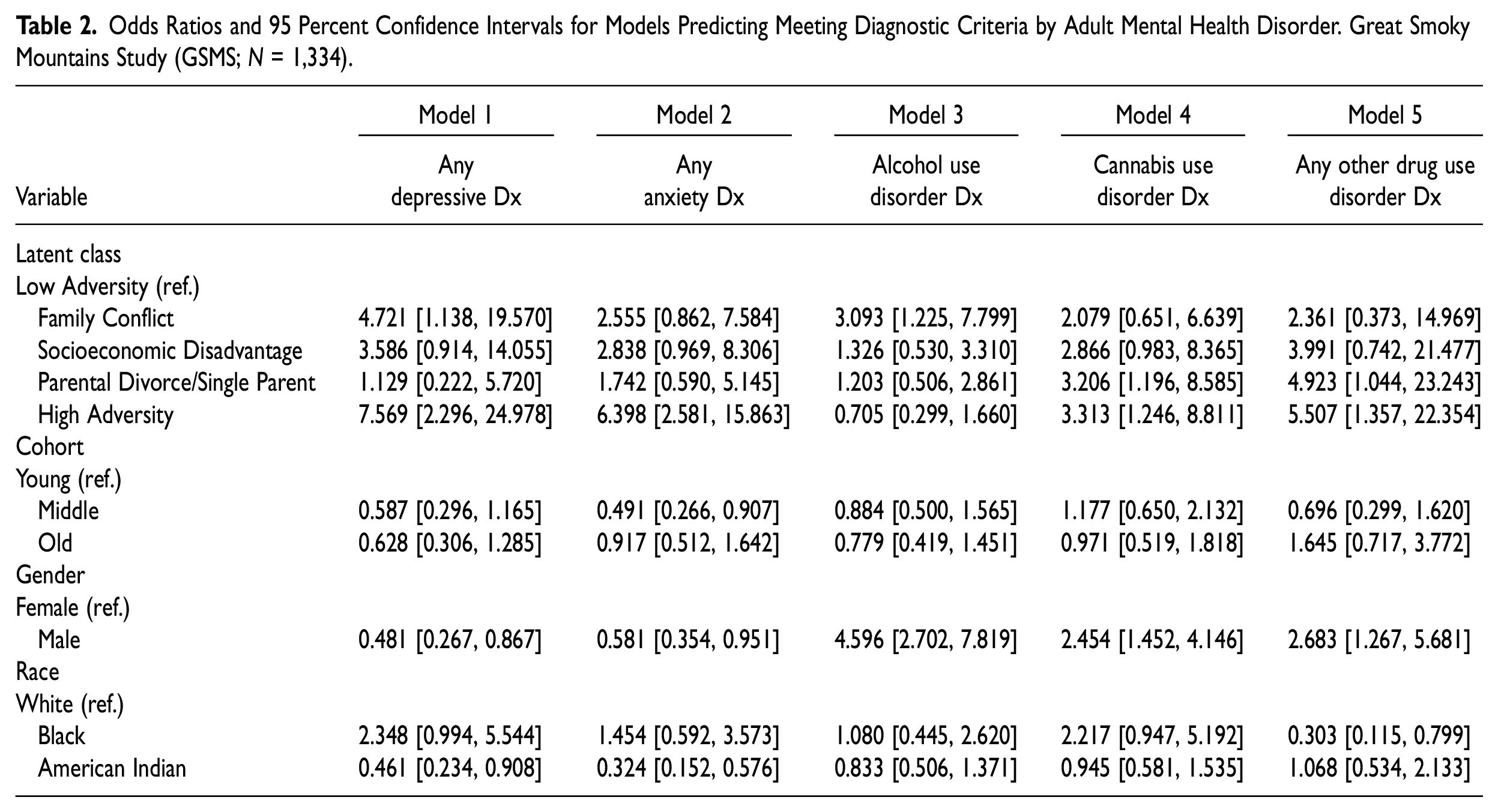
Results of models examining the three substance use disorders are presented in Table 2, Models 3 to 5. Model 3 suggests that the only class with greater odds of meeting the criteria for alcohol use disorder compared to the Low Adversity class is the Family Conflict class (odds ratios [OR] = 3.09). For the two drug-related outcomes (Models 4 and 5) the High Adversity and Parental Divorce/Single Parent classes have greater odds of meeting the criteria for cannabis use disorder and other drug use disorders compared to the Low Adversity class.
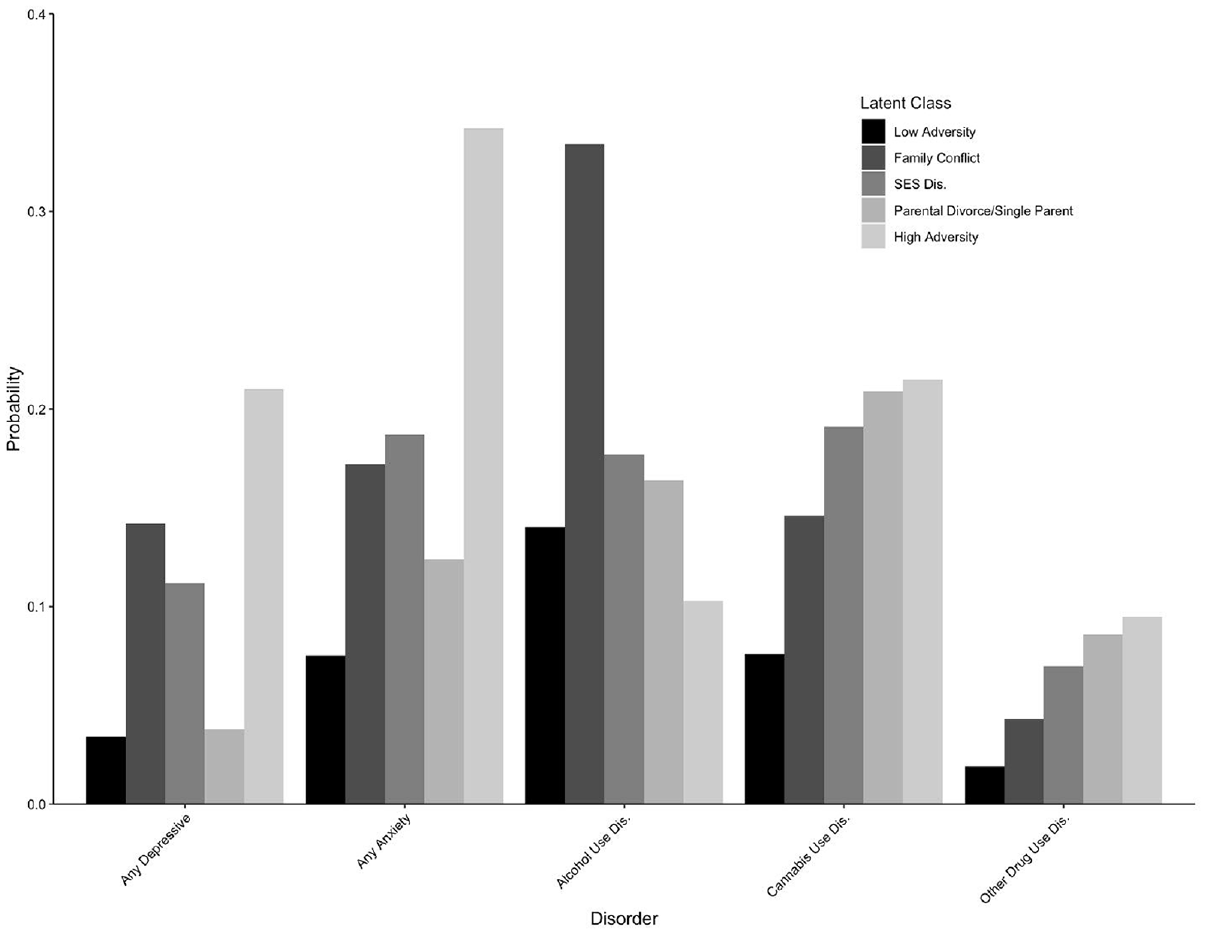
Figure 2 plots the predicted probability of meeting a disorder diagnosis during adulthood for each disorder and each class, adjusting for covariates. Although the results above are discussed mostly in reference to the Low Adversity class, the predicted probabilities in Figure 2 provide information on the predicted prevalence of these disorders for each class. This figure shows the stark contrast between the Low Adversity class compared to the other groups. In general, the highest predicted probability of meeting diagnostic criteria for this group was alcohol use disorder at 14.0 percent, with all other predicted probabilities for disorder diagnoses falling below 8 percent.
Predicted probability of meeting diagnostic criteria by adult mental health disorder and latent class.
The Family Conflict and SES Disadvantage classes have middling probabilities of meeting diagnostic criteria across all disorders, but the Family Conflict class has a somewhat elevated probability of depressive disorder diagnoses (14.2 percent) and a very elevated probability of alcohol use disorder diagnosis in adulthood (33.4 percent). The Parental Divorce/Single Parent class has a relatively lower probability of meeting the criteria for depressive and anxiety disorders but predicted probabilities of meeting the criteria for cannabis use and other drug use disorders that are similar to the High Adversity class. Unsurprisingly, the High Adversity class has the greatest probability of meeting most disorder diagnoses (except for alcohol use), with a particularly high probability of depressive (21.0 percent) and anxiety (34.2 percent) disorders.
As the relationship between childhood adversities and adult mental health may operate through baseline increases in symptomatology (Schafer and Ferraro 2013) and childhood symptoms may happen concurrently with adversities, we conducted supplementary analyses controlling for childhood diagnoses. In the waves before adulthood, in which respondents were children (<18 years old), the GSMS conducted structured clinical interviews for depressive and anxiety disorders using the CAPA. We include meeting diagnostic criteria in childhood for a specific internalizing (depressive or anxiety) disorder as a control in ancillary analyses of the concordant adult disorder. Predicted probabilities for models with and without adjusting for childhood diagnoses are presented in Supplemental Appendix C. When controlling for past symptoms, latent class differences remain in odds of meeting diagnostic criteria in adulthood (shown in Supplemental Appendix C).
We conducted similar analyses for substance use disorders (also shown in Supplemental Appendix C), with some additional considerations. Only alcohol use and cannabis use disorders were assessed in childhood, and the prevalence of these disorders was very low (below 5 percent). Therefore, we created a single measure of meeting the criteria of any substance use disorder (alcohol/cannabis use) in childhood (before age 18) and used this as a control in ancillary analyses of all substance use disorders in adulthood. Including this control does not alter latent class differences in meeting alcohol use disorder in adulthood, with the Family Conflict class continuing to have much greater odds compared to the Low Adversity Class.
However, controlling for meeting any substance use disorder diagnostic criteria in childhood does somewhat alter results for adult cannabis use and other drug use disorders. There are no longer significant differences in the odds of adult cannabis use disorder between the High and Low Adversity classes, and no longer significant differences in the odds of other drug use disorders between the Parental Divorce/Single Parent and the Low Adversity class. This suggests that early substance use related to and occurring in tandem with specific adversity experiences may partially explain these latent class differences in adult drug use.
Discussion
Consistent with CI theory and the life course perspective, research on childhood adversities has continued to demonstrate the predictive nature of early life experiences on adult well-being. This research has consistently shown that those who experience more childhood adversity (greater number of negative events) have worse mental health in adulthood. Yet, growing research suggests this relationship is not certain, and that features of adverse childhood experiences (e.g., the number, type, and co-occurrence of adversities), as well as the type of outcome assessed, may determine the long-term health consequences of early life (Giano et al. 2021; Kim et al. 2021; Wang et al. 2022). This study joins a growing line of research employing LCA (Barboza 2018; Curran et al. 2018; Heidinger and Willson 2019), to examine how configurations of adversities shape adult outcomes. Here, we expand this growing work by leveraging prospective data over several years of childhood (reported by both parent and child) and adulthood, including a broader range of childhood adversities, and examining the relationship between adversity experience and several different mental health disorder outcomes. Our study reveals several important findings.
First, by expanding the range of childhood adversities studied beyond those included in the original ACEs study (Felitti et al. 1998), we revealed several distinct adversity classes. Consistent with past work, we identified both “Low” and “High” Adversity classes (Barboza 2018). We also found evidence of Family Conflict, SES Disadvantage, and Parental Divorce/Single Parent classes. These classes can be seen as falling under a larger umbrella of “household dysfunction” (Felitti et al. 1998). However, by measuring an extensive set of measures of childhood adversities, we parse out experiences within household dysfunction to separate those who experience just family conflict versus socioeconomic disadvantage versus those advantaged financially but experiencing divorce and single parenthood. This specification revealed interesting demographic differences in adversity experience, with a higher proportion of Black and American Indian respondents in the Socioeconomic Disadvantage class and a higher proportion of White respondents in the Family Conflict class. We also note here that although only one class emerged as having very low adversity experience (average number of adversities <2) this group made up less than a third of the sample. Thus, despite differences in types of adversity, a majority of respondents indicated several experiences with adversity in childhood, confirming past estimates that childhood adversity is not rare (Felitti et al. 1998; Merrick 2019).
Second, in line with life course theories of childhood as a sensitive period, and CI theory suggesting that early life influences disparities in adult outcomes (Ferraro and Wilkinson 2013), we found that distinct configurations of childhood adversity predicted meeting diagnostic criteria for specific adult mental health disorders. Those in the Low Adversity class had the lowest predicted probability of meeting diagnostic criteria across all disorders, suggesting that this class’s lower exposure to adversity likely resulted in an accumulation of resources, such as economic capital associated with financial stability in childhood (Schafer, Ferraro, and Mustillo 2011), social capital through continued interpersonal success (Schafer and Ferraro 2013), and/or normative emotional regulation and development of self-esteem as a result of a stable home environment (McLaughlin and Sheridan 2016), which promoted mental wellbeing in adulthood. Conversely, consistent with work suggesting greater exposure to adversities is detrimental to well-being (Merrick 2019), the High Adversity class had the greatest predicted probability of meeting diagnostic criteria for most disorders. As opposed to children exposed to little/no adversity, those with high exposure to adversity, particularly in more serious domains such as abuse, likely accumulated a plethora of health-harming risks including continued interpersonal/financial strain or heightened reactivity to stressors across the life course (Schafer and Ferraro 2013; McLaughlin and Sheridan 2016), as well as missed out on health-promoting resources discussed above, contributing to poor mental health across outcomes.
However, such a relationship was not evident for alcohol use disorder. Although past work finds a similar lack of relationship (McGinnis et al. 2022), this was somewhat surprising given that this class had one of the highest occurrences of parental substance abuse in childhood, and research supports the intergenerational patterning of such disorders (Kim et al. 2021). Although CI theory does suggest that individuals may be able to offset the health impacts of negative experiences in early life (Ferraro and Shippee 2009), this would still not explain why individuals in the High Adversity class are resilient to developing alcohol use disorders, and not any other diagnoses.
Interestingly, those experiencing Family Conflict had the greatest likelihood of alcohol use disorder diagnosis, as well as an elevated likelihood of experiencing depressive affect. Given this group’s relatively high prevalence of interparental conflict and parent/child arguments, future work should explore the role of family conflict in shaping alcohol use. Some studies suggest that lack of parental support and supervision associated with familial conflict may increase adolescents’ risk of substance use (Repetti, Taylor, and Seeman 2002) and that alcohol abuse (as opposed to substance use generally) may be predicted by a severe form of family conflict (i.e., domestic violence) (Leza et al. 2021). These studies offer potential explanations, but why this group turns to alcohol, as opposed to cannabis or other drug use should be further explored.
Results also highlight the specificity of those experiencing Parental Divorce/Single Parenthood in drug use disorders. We also note that this finding was consistent across cannabis and other drug use, suggesting this group may turn to drugs generally instead of specific substances. This finding is consistent with a history of past work that underscores the role of parental conflict and divorce in shaping risky outcomes, particularly cannabis use, for adolescents that extend into adulthood (Gustavsen, Nayga, and Wu 2016). Although this group has a moderately-high experience with adversity, they do not experience a high prevalence of household poverty, parental unemployment, or low parental education. Future research focusing on specific mechanisms linking these classes to adult disorders should pay particular attention to the role financial access in tandem with stressful home environments plays in shaping drug use as opposed to alcohol use or internalizing disorders. No matter the exact pathway, the distinct outcomes for this class compared to the SES Disadvantage class (despite a similar overall number of adversities) underscores the importance of distinguishing the type of adversities experienced beyond the total number of adversities when predicting adult outcomes.
The lack of significantly elevated prevalence of any diagnoses for the SES Disadvantage class compared to the Low Adversity class was consistent with past work teasing apart different types of adverse experiences (Heidinger and Willson 2019; Schafer and Ferraro 2013). It may be that those who experience financial-related adversity accumulate less risk over the life course or can alter the trajectory of disadvantage through human agency and resources attained because of more positive childhood experiences across other domains (Ferraro and Shippee 2009). For example, if the lack of threatening or violent exposures allowed this group to build more social capital or develop psychosocial resources, like the low adversity group, that offsets any harm of financial strain. There is also a suggestion that exposure to some adversity, if not overwhelming, can help develop critical coping skills that could be employed to buffer the impact of stressors experienced across the life course to benefit mental well-being (Schafer, Ferraro, and Mustillo 2011). This type of adversity could also simply have a waning impact with age (Kamis 2020; Schafer and Ferraro 2013).
Future work should more specifically investigate whether and how those with socioeconomic disadvantage buffer the effect of these childhood adversities on adult mental health outcomes. This work could also be extended to assessing how individuals may offset the impact of childhood adversity more broadly, across latent classes of adversity experience. For example, through individual therapies and trauma-informed care associated with mental health disorders (Leza et al. 2021). Research in this vein may also include how policies can support individuals’ mental well-being during the transition into adulthood, as work using the GSMS has shown the benefits of early life family cash transfers on mental and physical functioning in adulthood (Copeland et al. 2022).
We note that the results presented here were mostly robust to the inclusion of childhood diagnoses. This emphasizes the long-term influence of childhood experiences, even net of any initial or concurrent relationship between childhood adversities and symptoms. Latent class differences in cannabis and other drug use disorders were slightly attenuated when accounting for childhood substance use disorders. This suggests that those with high experiences of adversity and those experiencing Parental Divorce/Single Parenthood may increase their drug use in childhood/adolescence with lasting dependence into adulthood. However, there is some specification in this finding, as substance use disorders in childhood appear to be the pathway for the High Adversity class for cannabis use only, whereas differences between the Low Adversity and the Parental Divorce/Single Parent class are attenuated only for other drug use disorders. It is important to mention that all childhood disorder diagnoses are measured in tandem with childhood adversities; therefore, any results here cannot specify temporal order. Consistent with CI theories of risk accumulation, future work with clearer temporal ordering should explore other pathways across the life course outside of (or in addition to) early internalizing and substance use diagnoses that can help explain the long-term consequences of childhood adversity.
Results here are presented considering several limitations. Importantly, we do not account for other features of adversity, such as the timing of events, frequency and duration of exposure, or severity of adversity. Such components have been shown to shape life course mental health (Kamis 2020), and thus future research should use this study as a necessary stepping stone to further explore the nuances of these long-term relationships as they relate to adversity characteristics.
Due to the study design, those in different cohorts were not observed for the same number of waves in childhood. For example, those in the young cohort (age 9 at baseline) were observed for at most seven waves but those in the old cohort (age 13 at baseline) were only observed for at most four waves before age 18. Furthermore, the youngest age of prospective measurement is nine years old, thus adversities measured “within the past three months” may be underestimated if they occurred at younger ages or underestimated for those with fewer waves of observation. However, this lower age bound does not impact the measurement of lifetime adversities, and having more than one wave of childhood observed for any cohort is still an improvement on studies that focus on retrospective measurements and/or measures of childhood adversities from a single wave. We also control for cohort membership to adjust for differences in the number of waves measured.
Growing research building on CI theory recognizes that the distribution of risks, such as childhood adversity, is unequal and based in macro systems of inequality (Ferraro and Shippee 2009; Kysar-Moon 2020). Indeed, we do find evidence of racial/ethnic patterning of exposure to adversity, with White respondents being more privileged via their representation in the more advantaged typologies (e.g., Low Adversity class). Although outside the scope of the present study and somewhat limited by the predominately white sample (89.40 percent), future work should consider whether the results presented here are consistent across salient social characteristics, such as race/ethnicity and gender. Finally, the GSMS sample is not representative of the United States as a whole. This sample has a higher proportion of American Indians and a lower proportion of Black respondents than would be expected for a nationally representative sample. This sample is also based in an area with higher levels of rurality. Despite the lack of U.S. representativeness, this sample does provide the unique opportunity to include individuals who are often at higher risk of stressful life events yet underrepresented in studies and work has shown that the rates of mental health disorders in the GSMS are similar to that of other U.S. studies (Copeland et al. 2011).
Despite these limitations, this study makes important contributions to the exploration of childhood adversities and the impact of adversities on life course mental health. As shown here, experiences with adversity are not rare and specific configurations of adversities are uniquely related to mental health outcomes in adulthood. This is important as poor mental health impacts not only one’s quality of life but also their ability to fulfill and maintain social relationships and roles in adulthood (George 2013). The findings here should be considered when developing screenings for adversities in childhood and retrospective screenings in adulthood. These screenings should aim to measure a broad spectrum of adversities and interventions moving forward should be informed by distinct connections between configurations and specific outcomes. At the same time, following recommendations made by David Finkelhor (2018), screenings should be pursued when there are also adequate resources to accommodate children/adults identified as at-risk. Moreover, efforts should be made to reduce the occurrence of childhood adversities in the first place, as this study and others have enumerated the many costs of such experiences that extend beyond mental health diagnoses to physical health, adult functioning, and even mortality (Finkelhor 2018).
Conclusion
Childhood adversity has long-term consequences for adult well-being. However, those consequences depend on the number, and importantly the type, of co-occurring adversities in early life. This article underscores the importance of adequately capturing adversity experiences when predicting adult mental health disorder diagnoses, suggesting unique connections exist between early life experiences and health outcomes. Future work should continue to explore ways of measuring childhood adversity, to identify which experiences predispose individuals to diagnoses over the life course.
Supplemental Material
sj-pdf-1-smh-10.1177_21568693231197746 – Supplemental material for Associations between Configurations of Childhood Adversity and Adult Mental Health Disorder Outcomes
Supplemental material, sj-pdf-1-smh-10.1177_21568693231197746 for Associations between Configurations of Childhood Adversity and Adult Mental Health Disorder Outcomes by Christina Kamis, Scott M. Lynch and William E. Copeland in Society and Mental Health
Footnotes
Authors’ Note
Christina Kamis is currently affiliated with Department of Sociology, University of Illinois Urbana-Champaign, Urbana, IL, USA.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the grant T32 AG00129, awarded to the Center for Demography of Health and Aging at the University of Wisconsin-Madison by the National Institute on Aging. This research was also supported by the National Institute of Mental Health (R01MH117559), the National Institute on Drug Abuse (R01DA036523 and R01DA011301), and the National Institute of Aging (R01AG072459).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.