
Abstract
Documentation of prescriptions and clinical outcomes in routine homeopathic practice is a prerequisite for conducting targeted research in homeopathy. Six homeopathic physicians participated in methodical data collection over a 3-month period in 6 outpatient departments of Mahesh Bhattacharyya Homeopathic Medical College and Hospital, West Bengal, India. A specifically designed Microsoft Excel spreadsheet enabled recording of consecutive appointments—date, patient identity, medical condition/complaint, whether chronic/acute, new/follow-up case, patient-assessed outcome (7-point Likert-type scale: −3 to +3), prescribed homeopathic medication, and whether other medication/s being taken for the condition. Spreadsheets were submitted monthly for data synthesis and analysis. A total of 1972 patients’ follow-up generated data of 2905 appointments, of which 2272 (78.2%) were positive, 183 (6.3%) negative, and 450 (15.5%) showed no change. Strongly positive outcomes (scores of +2/+3) were recorded in osteoarthritis, piles, cough, dysfunctional uterine bleeding, chronic suppurative otitis media, and conjunctivitis. This systematic recording short-listed promising areas of future homeopathic research.
Clinical research in homeopathy has grown to a substantial extent of 1110 clinical studies, including 356 double-blind randomized controlled trials up to 2014. 1 Simultaneously, the necessity for documentation of prescriptions and clinical outcomes in routine homeopathic practice and systematic analysis of relevant data has been highlighted to lay the foundation for conducting targeted research in homeopathy. 2 Critical scrutiny of prescriptions to illustrate favorable clinical responses to prescribed medicines is fundamental for carrying out efficacy trials. On account of absence of control, these observations cannot offer evidence of an effect that can be causally attributed to the homeopathic intervention; still, can be considered as valuable evidence-seeking activity by pointing out probable association between treatment and outcome. 3 It would be a practical input that could be made toward an evidence base, without undertaking the rigorous demands of experimental studies. These outcomes research progresses beyond mere unstructured observation, and still represents clinical findings in the “real-world” setting of homeopathic medical care.
Systematic and targeted large-scale clinical data collection was initiated in multipractitioner homeopathic settings, 2 including dentistry, 4,5 in the past decade. The investigators also successfully piloted a similar project on dental homeopathic practice in a homeopathic hospital setting in West Bengal, India and highlighted promising areas of future research. 6 Now they intend to engage the homeopathic doctors of Mahesh Bhattacharyya Homeopathic Medical College and Hospital to collect clinical and outcomes data over a 3-month period in their outpatient settings. The objectives of such an initiative were to gain insight into the complaints that homeopathic doctors treat in the hospital outpatient setting and for follow-up cases, to determine patient assessed change in severity of the treated medical condition/complaint by comparing the last with the first homeopathic consultation, and thus identifying any specific patterns of disease, clinical responses, and/or homeopathic medicines that may help to target future research in homeopathy.
Materials and Methods
The study was of 3 months’ duration; July to September, 2014. The study design was prospective and observational. Six homeopathic doctors willing to contribute to the study were provided with a specially designed spreadsheet (Microsoft Excel). 2 The doctors had a practicing experience of 10 to 20 years in hospital outpatient settings. Detailed instructions on using the spreadsheet format, and how to ask patients questions about their clinical outcome, were detailed on separate pages of the file. The spreadsheet allowed recording of consecutive appointments, row by row, under the following column headings: appointment date (day, month), unique (anonymized) patient identity number, age and gender of the patient, the condition/complaint treated, system-based category of condition/complaint, whether the condition/complaint is “chronic” or “acute,” whether, in relation to the previous 12 months, that was a new or a follow-up appointment for the same complaint, patient-assessed change in the treated complaint at the current follow-up compared with the initial homeopathic consultation, using a 7-point scale (“no change” or “unsure” = 0; “mild” = ±1; “moderate” = ±2; “major” = ±3), homeopathic medicine/s prescribed, any other medication/s (conventional) being taken for the condition/complaint, and comments, if any.
On receipt of the final spreadsheets at the end of the project, the original data were rechecked and scrutinized for obvious missing data and typographical errors. These were flagged up and rectified where possible. A new master copy of the complete appointments page were then created, into which new columns were added to indicate (a) the appointment number per patient per condition/symptom and (b) whether or not an appointment was the final one for a given condition/symptom in a given patient during the 3 months of the study. These procedures enabled analysis based on final appointments, that is, on the number of individual patient conditions treated, irrespective of whether they were treated by the doctor once, twice, or more often. The term individual patient condition was used because a given patient could present with different conditions on a different, or even the same occasion. Also, if a patient presented at one appointment with more than one condition, each of which was treated separately with homeopathy, the doctor reported each on a different row of the spreadsheet. This approach was adopted because a key purpose of the study was to catalogue the frequency and success rate of treating named conditions, even if a given individual patient exhibits more than one. After the final dispatch of their practice data, doctors were sent a brief questionnaire, designed to gauge their experience of using the spreadsheet and their opinions of the value they attributed to the data it produced.
The following principal analyses were then carried out: (a) “final” outcome score by acute/chronic conditions, (b) “final” outcome score by medical category, (c) “final” outcome score by medical conditions/complaints, and (d) enlisting the most frequently used homeopathic medicines in different outpatient settings.
Results
The 6 participating doctors submitted data reliably; each sent an updated spreadsheet for every month for 3 consecutive months. The appointments appeared to be recorded meaningfully. The most common difficulty was in cases where a patient presented with 2 discrete medical conditions; however, notably, in all occasions, single remedy was prescribed. Separate rows were used to describe independent medical complaints for the same patient. Missing values were rectified wherever possible before final analysis.
The presence of other (conventional) medication/s taken for the condition/complaint (including “none”) was noted on just 3.8% of appointments. Some participants made ready use of the column “comments, if any” for additional notes, while others used it sparingly.
While reflecting results, we considered only the patients completing at least 2 or more follow-ups. A total of 1972 patients’ follow-ups generated data of 2905 appointments, of which 2272 (78.2%) were positive, 183 (6.3%) negative, and 450 (15.5%) showed no change. Outpatient distribution of the patients were as follows: medicine (n = 566), surgery (n = 587), pediatrics (n = 140), obstetrics and gynecology (n = 166), otorhinolaryngology (n = 326), and ophthalmology (n = 187). Majority of the patients were aged 41 to 60 years (n = 721, 36.6%; Figure 1) and majority were female (n = 1107, 56.1%; Figure 2).

Age profile of the follow-up patients visiting the 6 outpatient departments (N = 1972).
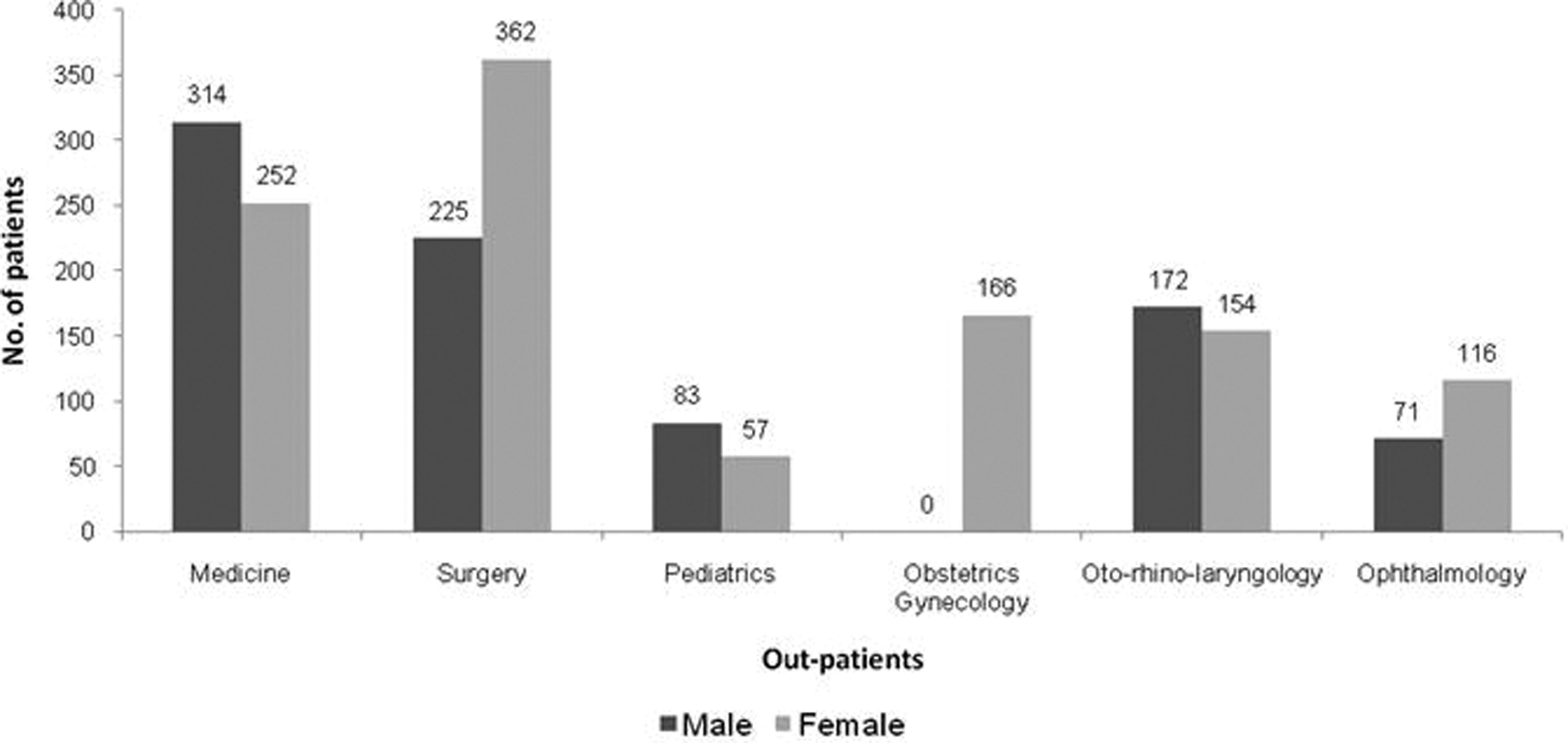
Gender distribution of the follow-up patients visiting the 6 outpatient departments (N = 1972).
Participating doctors treated 328 different medical conditions in total; 5 most frequently treated complaints per outpatient department are presented. Osteoarthritis (55.1%), piles (82.3%), cough (94.4%), anal fissure/fistula (74.3%), and common cold (96.2%) consisted of the chief conditions reported in the medicine outpatient department. The outpatients of surgery department documented principally osteoarthritis (73.3%), minor injury (49.3%), piles (60.3%), low back pain (54.8%), and anal fissure/fistula (74.3%). The pediatric outpatient setting showed cough (78.3%), common cold (84.2%), fever (72.2%), minor injury (18.2%), and bronchial asthma (40.0%). Dysfunctional uterine bleeding, dysmenorrhea, polycystic ovarian syndrome, urinary tract infection, and uterine fibroid were the most frequently reported ailments in obstetrics and gynecology. The otorhinolaryngology outpatient setting accounted for chronic suppurative otitis media, nasal polyp, deafness, tinnitus, and tonsillitisy. Refractory errors, cataract, conjunctivitis, stye, and dacrocystitis were the mostly encountered conditions in the ophthalmology outpatient department (Table 1).
Outpatient-wise 5 Most Frequently Treated Conditions/Complaints During 3 Months.

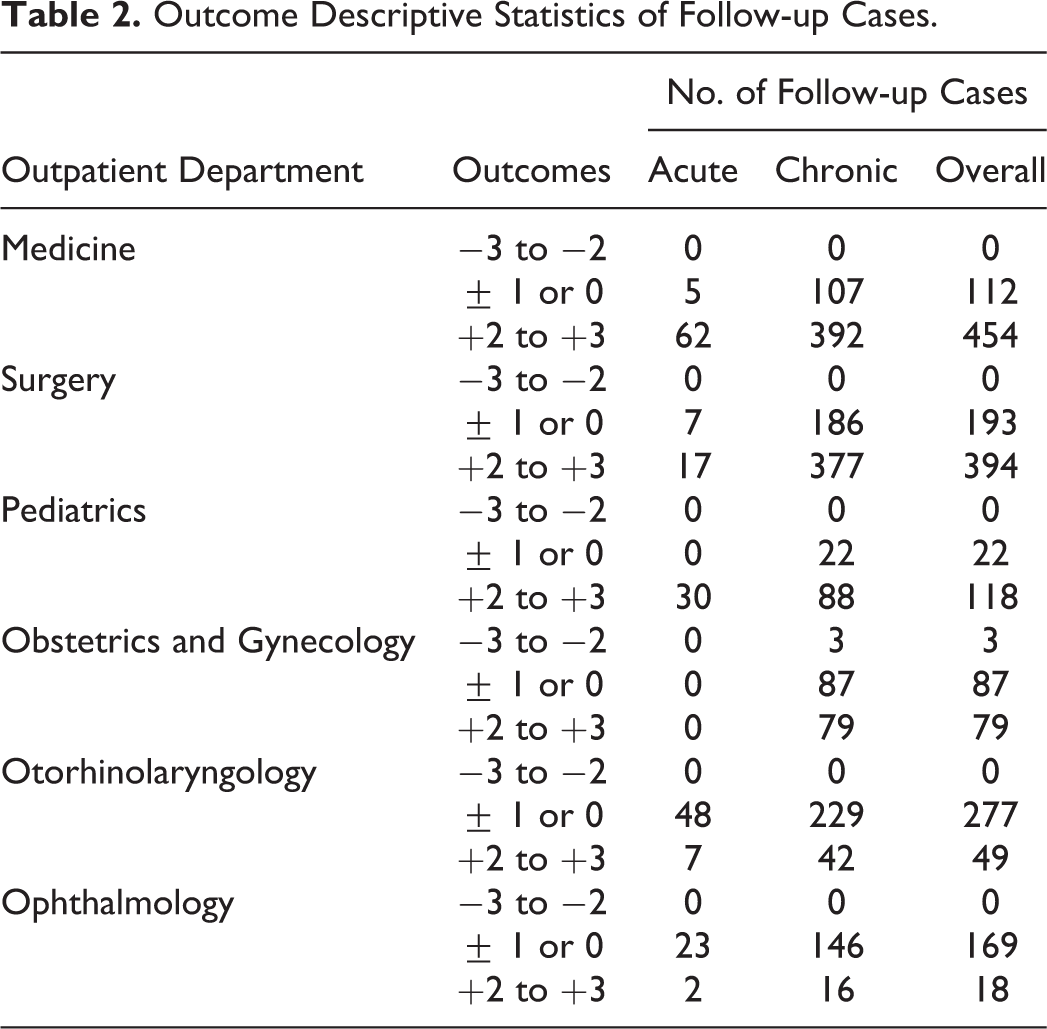
Strongly positive outcomes (+2/+3) were recorded in 80.2% patients of medicine, 67.1% patients of surgery, 84.3% patients of pediatrics, 47.6% patients of obstetrics and gynecology, 15.0% patients of otorhinolaryngology, and 9.6% patients of ophthalmology settings (Table 2).
Outcome Descriptive Statistics of Follow-up Cases.
Strongly positive outcomes (+2/+3) were reported in 65.0% to 97.1% follow-ups in patients suffering from categories of musculoskeletal, gastrointestinal, respiratory, dermatological, and ear, nose and throat in the medicine outpatient setting; 50.0% to 94.1% follow-ups in patients suffering from categories of musculoskeletal, gastrointestinal, respiratory, urogenital, and dermatological in the surgery outpatient setting; 72.7% to 92.3% follow-ups in patients suffering from categories of respiratory, dermatological, gastrointestinal, central nervous system and psychiatry, and endocrinology in the pediatric outpatient department; 46% follow-ups in patients suffering from category of obstetrics and gynecology in the obstetrics and gynecology outpatient department; 8.6% to 31.8% follow-ups in patients suffering from categories of ear, nose, and throat, musculoskeletal, gastrointestinal, respiratory, and dermatological in the otorhinolaryngology outpatient setting; and 9.7% follow-ups in patients suffering from categories of eye in the ophthalmology outpatient department (Table 3).
Summary of Outcome Scores of Follow-ups by Category.

Abbreviations: CNSP, central nervous system and psychiatry; DERM, dermatological; ENDO, endocrinology; ENT, ear, nose, and throat; GI, gastrointestinal; MSK, musculoskeletal; OG, obstetrics and gynecology; RESP, respiratory; URO, urogenital.
Among the medical conditions, strongly positive outcomes (+2/+3) were reported in 55.1% to 96.2% follow-ups in patients suffering from osteoarthritis, piles, cough, anal fissure/fistula, and common cold in the medicine outpatient department; 49.3% to 73.3% follow-ups in patients suffering from osteoarthritis, minor injury, piles, low back pain, and anal fissure/fistula in the surgery outpatient department; 18.2% to 84.2% follow-ups in patients suffering from cough, common cold, fever, minor injury, and bronchial asthma in the pediatric outpatient setting; 35.3% to 58.6% follow-ups in patients suffering from dysfunctional uterine bleeding, dysmenorrhea, polycystic ovary, urinary tract infection, and uterine fibroid in the obstetrics and gynecology outpatient setting, 4.0% to 20.9% follow-ups in patients suffering from chronic suppurative otitis media, nasal polyp, deafness, tinnitus, and tonsillitis in the otorhinolaryngology outpatient setting; and 15.0% to 23.5% follow-ups in patients suffering from conjunctivitis, stye, and dacrocystitis in the ophthalmology outpatient department (Table 4).
Summary of +2/+3 Outcomes of Final Follow-ups by Medical Condition/Complaint.

Individualized prescription was the rule in all of the appointments. A total of 282 different homeopathic medicines were reported. “Polychrest” remedies were frequently prescribed. Per outpatient setting, the most frequently used medicines were as follows: medicine, Rhus toxicodendron (10.8%); surgery, Calcarea fluorica (17.0%); pediatrics, Bryonia alba (10.2%); obstetrics and gynecology, Sulphur (6.3%); otorhinolaryngology, Rhus toxicodendron (9.7%); and ophthalmology, Rhus toxicodendron (5.6%). Mother tinctures, decimal, centesimal, and 50 millesimal potencies were prescribed in 7.8%, 12.3%, 58.4%, and 21.5% occasions. Placebos accounted for 18.9% of prescriptions. Several instances of matching between a specific medical condition and a particular homeopathic medicine were found. Some of the following medicine-condition pairings were most noticeable: Rhus toxicodendron and Calcarea fluorica for osteoarthritis (41.3% and 39.6%, respectively), Sulphur in piles (32.0%), Rhus toxicodendron in cough (44.2%) and common cold (32.6%), Arnica montana for injury (69.2%), Sulphur (27.8%) in dysfunctional uterine bleeding, and so on (Table 5).
Five Most Frequently Used Homeopathic Medicines per Outpatient Department.

Five of the 6 participating homeopathic doctors used Excel spreadsheet previously. All of them found the spreadsheet, though a bit time-consuming, really practical to use and easy to enter data into that. It seemed to all the doctors that the outcome question sequence was understood by the patients and it was also easy to score the stated outcome on the 7-point scale. Still, everyone thought that this scoring had a positive bias. They found it convenient to return data on a monthly basis through e-mail. All expressed their interest in taking part in future controlled research. Including “trustworthy” physicians in the work was stressed by one doctor. It was also suggested to conduct larger scale data collection by the doctors working in “State Homeopathic Dispensaries” and “Homeopathy Specialty Clinics” in West Bengal, India.
Discussion and Conclusion
This methodical and meaningful documentation of clinical outcome of homeopathic appointments in different outpatient settings identified promising areas of future clinical research. In spite of its inherent limitations, it laid the groundwork for conducting targeted research. Pick-listing the most frequently used medicines and conditions/complaints treated most often and with greatest apparent success identified the areas where initiation of efficacy trials seemed to be reasonably feasible, both by predefining probable medicines, and also by imposing no restrictions on the physicians allowing them to choose from a wide range of remedies. Though individualized prescribing was the norm, it was equally apparent that few homeopathic medicines tended to be selectively used for specific medical conditions.
This study assessed only changes from a recalled baseline—a potential source of bias. The noncontrolled outcome statistics refer only to patients who were reassessed at follow-ups, thus not executing intention-to-treat analysis. Selection bias, interaction bias, and empathy bias may also equally be inflicted on the results. Seasonal variation may have also affected the outcomes.
The overall rate of positive outcome in 78.2% of follow-up patients in our study is similar to that reported in other homeopathy outcome studies in primary care. 2,7,8 and in hospital settings. 9–11 Although the use of 7-point Likert-type scale was previously validated in homeopathy outcome audits, and was expedient to use, it would be still be more acceptable to have validated outcome scales for specific medical conditions. Considerable changes were noted in the prescription pattern of physicians. All the prescriptions were individualized, a finding quite higher than 2 earlier studies, 12,13 thus indicating substantial incorporation of corrective measures to curtail rampant prescriptions. The use of centesimal potencies decreased from 74.8% to 58.4%, while that of others increased simultaneously. No prescription of external application was documented during these 3 months. Most frequently reported medical conditions/complaints also varied to some extent. Use of other conventional medications, though reported sparingly, was mostly over-the-counter drugs, a finding that supported a previous report. 14
Finally, this clinical outcome study may act as fundamental in informing well-targeted and controlled future research in homeopathy feasible in the hospital outpatient setting.
Footnotes
Acknowledgments
The authors hereby acknowledge Dr Nikhil Saha, Acting Principal of Mahesh Bhattacharyya Homeopathic Medical College and Hospital for allowing us to carry out the project successfully at his institution. The authors are also grateful to Dr Goutam Nag, Dr Amila Modak, Dr Subrata Saha, Dr Monojit Kundu, Dr Ramkumar Mondal, and Sk Swaif Ali for their sincere cooperation in data collection. The authors are also thankful to the patients for their participation in this study.
Author Contributions
SS, MK: concept, design, literature search, data interpretation, statistical analysis, manuscript preparation. SG, MG, AD, RG: clinical study and data acquisition. All the authors edited, reviewed, and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The Institutional Ethics Committee of Mahesh Bhattacharyya Homeopathic Medical College and Hospital approved the study prior to its initiation.