
Abstract
Accessibility to and utilization of the hospital health services is a complex and multifaceted issue. This study aimed to assess the knowledge of the patients of health services, current level of access to and utilization of services and to identify barriers and socioeconomic disparities in an Indian homeopathic hospital. A cross-sectional survey was conducted in December 2013 on systematically sampled 377 patients. Responses were analyzed using descriptive statistics and univariate logistic regression. Mean knowledge score and perceived mean difficulties in access to and utilization of services were 68.4% and 78.5%, respectively. Knowledge of the services was influenced by age, residence, education, speaking and reading of Bengali language, and income status (P < .05). Difficulty in access to and utilization of the health services were influenced by residence, understanding of Bengali language, and monthly household income (P < .05). Overall, health service access and utilization appeared promising, but needs improvement.
Keywords
Introduction
The use of health services is defined as the process of seeking professional health care and submitting oneself to the application of regular health services, with the purpose of preventing or treating health problems. 1 The help of regular health services is often only called on after an escalation of the complaints of illness. 2 Although the decision to use health services is stated to be an individual choice, it can be attributed to a variety of factors such as unhealthy lifestyles, social influences, and general socioeconomic conditions, including unequal access to health services. Differences in health care utilization have been long noted among demographic groups. 3 Accessibility to health services is a complex and multifaceted issue. Inequalities in accessibility and in other determinants in health differ within and between countries. Care providers are often oblivious to these barriers, although they may share to some extent the burden of responsibility for them. 1 In order to enlighten care providers, as to the potential pitfalls that may exist, there is a need to explore the different factors in identification of the barriers. Thus, national policies should include specific, realistic, and obtainable goals.
Although researchers are continually dealing with the issue of health care services in homeopathic hospitals, 4 –6 there is no clear evidence about the utilization and accessibility to health care services. Mahesh Bhattacharyya Homeopathic Medical College and Hospital currently runs under the West Bengal University of Health Sciences, Government of West Bengal, under affiliation with the Central Council of Homeopathy, Government of India. The academic section is concerned with running 4½ years of undergraduate course in homeopathy followed by 1 year of rotator internship and 3 years of stipendiary postgraduate course specializing in homeopathic repertory. The hospital section runs 8 daily outpatient clinics, 60-bedded inpatient, 24-hour emergency services, special outpatient clinics on reproductive and child health, dentistry, physiotherapy, ophthalmology, ear-nose-throat, directly observed treatment and short-term chemotherapy for patients with tuberculosis, special research clinics, and various radiographic and biochemical diagnostic tests.
This study aimed to assess knowledge of the patients visiting Mahesh Bhattacharyya Homeopathic Medical College and Hospital on health services, the current level of access to and utilization of services, barriers or obstacles encountered during visits, and sociodemographic disparities in access to health care. This research has the goal of raising awareness about the myriad potential barriers, so that the problem of barriers to health care access becomes transparent and feasible solutions may be sorted out, ultimately leading to improved patient care.
Materials and Methods
Study Design
A cross-sectional, institutional survey was conducted on 377 patients in December 2013 at Mahesh Bhattacharyya Homeopathic Medical College and Hospital. Approval was taken from the institutional ethics committee prior to conducting the study. Survey respondents were distributed information sheet detailing the study and written consent were obtained before participation in the study.
Sample
Considering margin of error 5%, confidence level 99%, population size unknown, and response distribution estimated to be 50%, target sample size was calculated to be 377. Systematic sampling procedure was adapted to screen the patients visiting outpatients of the hospital. Sampling fraction was estimated (and approximated) to be 5/6 (n/N; n = required sample size of 377; N = average number of outpatient patients every day, that is 450); 5 was decided as the sampling unit by simple random sampling, and thus every fifth patient was interviewed.
Study Instrument
No universally accepted standardized questionnaire was available to evaluate access to and utilization of the health care services provided, especially in any homeopathic hospital in India. We developed a semistructured questionnaire consisting of 22 questions—2 were open and the remaining 20 were close-ended, provided with options. The directions to fill up the questionnaire were explained verbally to all the patients in detail by the research assistants. The questionnaire was aimed at assessing the patients’ sociodemographic profile, proficiency in local vernacular Bengali, knowledge of and current status of health and treatment, satisfaction with the services received, difficulties faced and reasons accounted for, and assessed quality of services by the patients. Proficiency in Bengali language and current health status of the patients were assessed on a 5-point Likert-type scale (1 = very poor, 2 = poor, 3 = moderate, 4 = good, 5 = very good). Communication with doctors (1 = very poor, 2 = poor, 3 = fair, 4 = well, 5 = very well), difficulties (1 = not at all, 2 = slightly, 3 = moderately, 4 = quite a bit, 5 = extremely difficult), quality of services (1 = very poor, 2 = poor, 3 = moderate, 4 = good, 5 = very good), and level of satisfaction (1 = very unsatisfied, 2 = unsatisfied, 3 = indifferent, 4 = satisfied, 5 = very satisfied)—all were again assigned with different 5-point Likert-type scales. A separate sheet enlisting the health services provided by the hospital was requested to fill to measure patients’ knowledge of the services.
Data Extraction and Analysis
A specially designed Microsoft Excel sheet was used for data extraction and was subjected to statistical analysis. Descriptive statistics were presented as absolute values and percentages. Univariate logistic regression analyses were performed to identify associations and differences. P values <.05 (2-tailed) were considered as statistically significant.
Results
Patients spanned all decades of age, but most were 40 to 49 years old (90, 23.9%). Majority of them were female (229, 60.7%), Hindu (351, 93.1%), residents of urban families (237, 62.9%), married (259, 68.7%), having educational status of less than high school (132, 35.0%), and had no health insurance (302, 80.1%). Most of the respondents were unemployed (234, 62.1%), and having monthly family income of Indian rupees less than 10 000 (248, 65.8%; Table 1).
Sociodemographic Characteristics of the Study Participants.

Ability and proficiency in the local vernacular Bengali of the patients were good to very good, as was in understanding (348, 92.3%), speaking (364, 96.6%), and reading (351, 93.1%; Table 2).
Ability of Participants in Bengali Language; n (%).

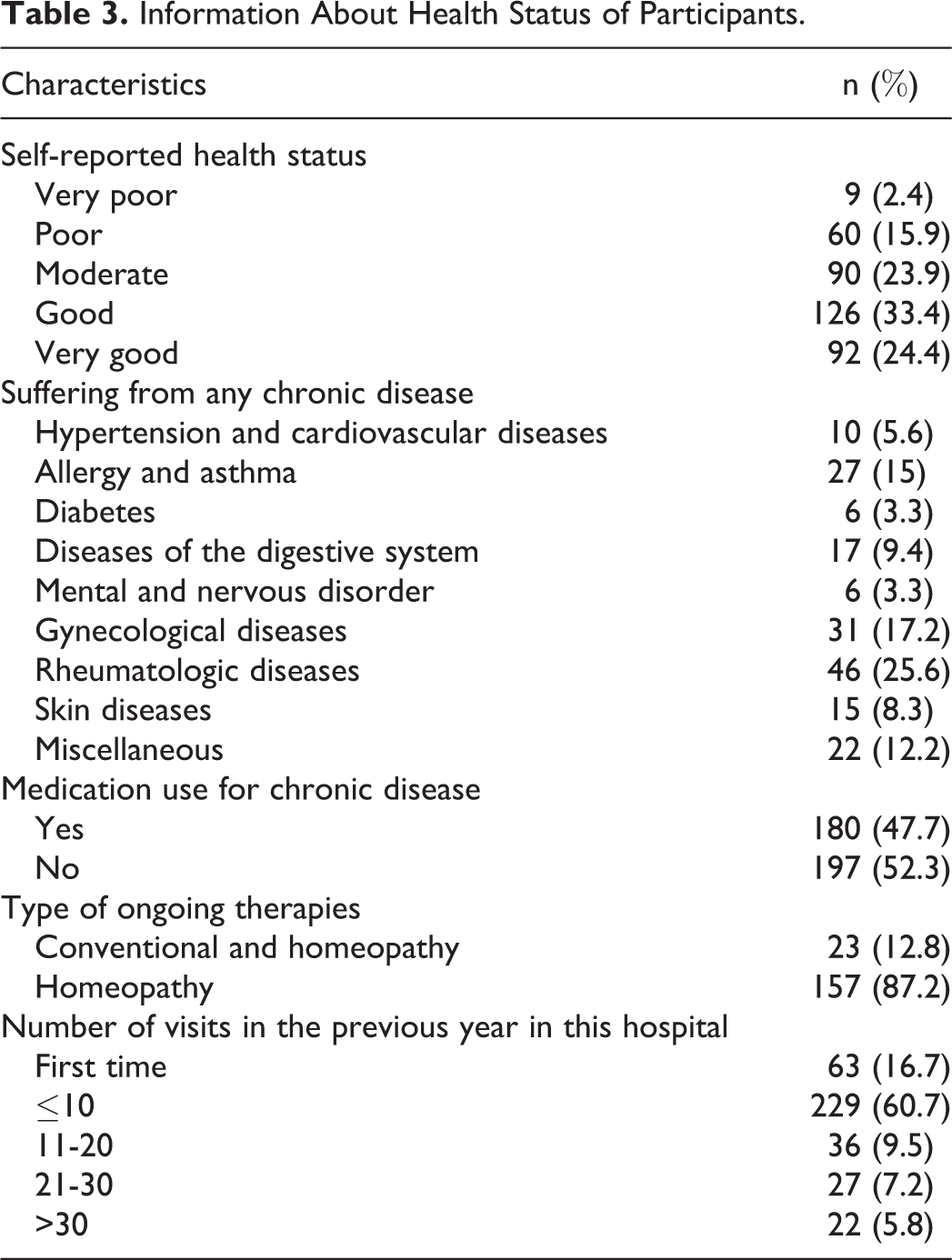
Self-reported health status of the survey participants ranged from good to very good (218, 57.8%). Among the respondents, 180 (47.7%) were suffering from and were undergoing treatment for underlying chronic diseases, mostly rheumatologic complaints (46, 25.6%); gynecologic disorders (31, 17.2%), and allergy and asthma (27, 15%). Strikingly, they preferred homeopathic treatment alone (157, 87.2%) for the chronic disease in comparison with integrated approach (23, 12.8%). Majority (229, 60.7%) reported about 10 times visits in the previous year in the hospital (Table 3).
Information About Health Status of Participants.
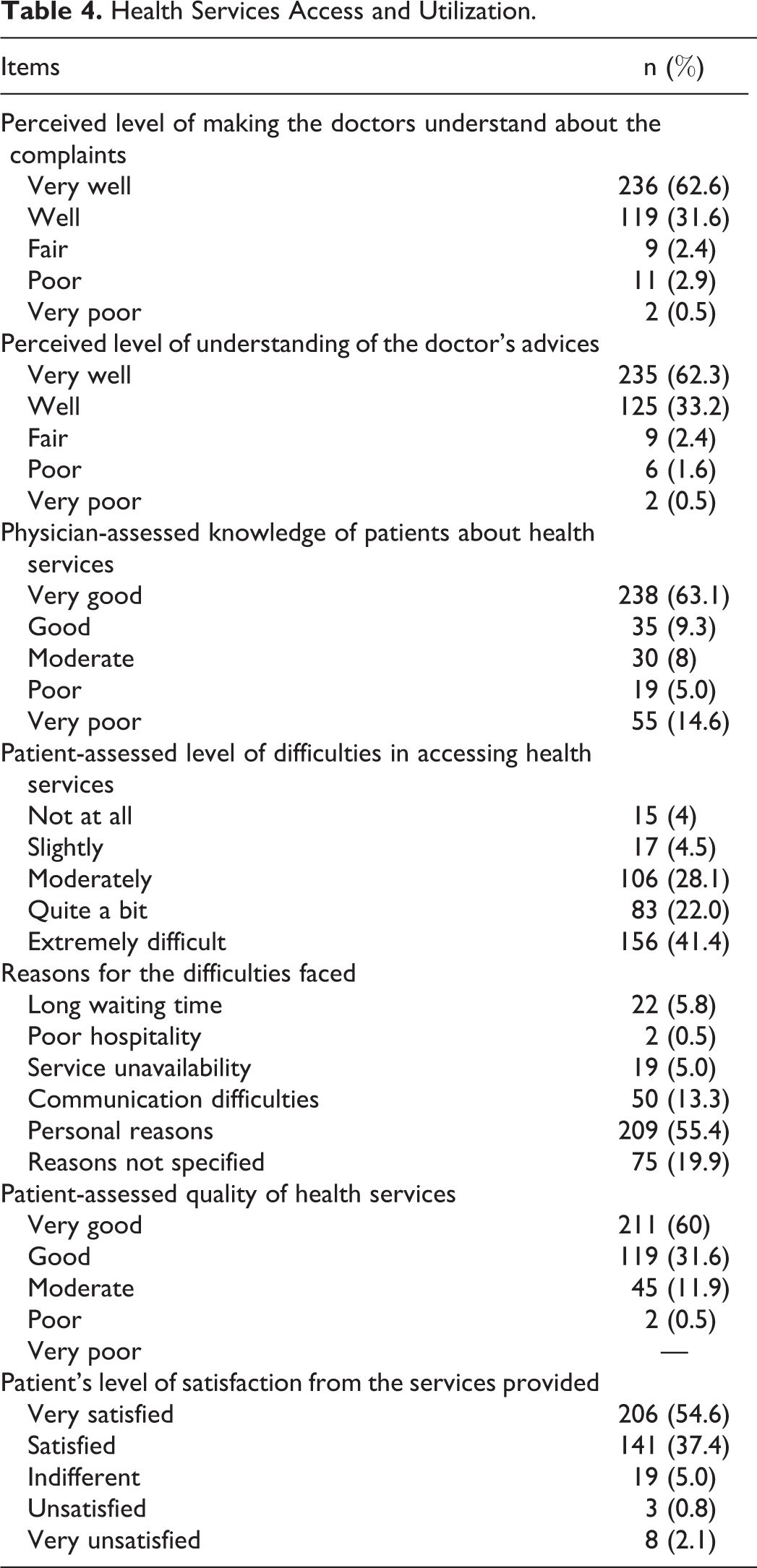
Patients’ perceived level of making the doctors understand about the complaints (355, 94.2%) and understanding the doctor’s advices (360, 95.5%) ranged from well to very well. Knowledge of the patients about health services was good to very good (273, 72.4%). Patient-assessed level of difficulties in accessing health services was moderate to extremely difficult (305, 91.5%). Most frequently cited reasons for the difficulties faced were personal reasons (209, 55.4%), reasons not specified (75, 19.9%), and communication difficulties (50, 13.3%). Patient assessed quality of health services was good to very good (330, 87.5%) and the level of satisfaction from the services provided ranged from satisfied to very satisfied (347, 92.0%; Table 4).
Health Services Access and Utilization.
Knowledge of health services (mean percentage 68.4; standard deviation = 33.9) was influenced significantly by age, residence, education, speaking and reading Bengali, and monthly household income more than Indian rupees 30 000. Age was positively correlated with knowledge score; that is, higher the age in comparison with ≤20 years, knowledge increased significantly (21-40 years, coefficient 0.055, odds ratio [OR] = 1.057, 95% confidence interval [CI] = 1.024-1.091), χ2 = 11.680, P = .001; 41-60 years, coefficient 0.049, OR = 1.051, 95% CI = 1.018-1.084, χ2 = 9.694, P = .002; ≥60 years, coefficient 0.048, OR = 1.049, 95% CI = 1.011-1.090, χ2 = 6.675, P = .009). Residence was correlated negatively, that is, higher distance was associated with decrease in knowledge score (semiurban, coefficient −0.032, OR = 0.968, 95% CI = 0.945-0.992, χ2 = 6.607, P = .010; rural, coefficient −0.044, OR = 0.957, 95% CI = 0.932-0.982, χ2 = 10.475, P = .001). Education was positively correlated (less than higher secondary, coefficient 0.044, OR = 1.045, 95% CI = 1.014, 1.076, χ2 = 8.422, P = .004; higher secondary, coefficient 0.057, OR = 1.058, 95% CI = 1.026-1.091, χ2 = 13.692, P = .0002; more than high school, coefficient 0.057, OR = 1.058, 95% CI = 1.023-1.095, χ2 = 11.324, P = .001. Patients speaking Bengali with good ability (coefficient 0.069, OR = 1.071, 95% CI = 1.006-1.140, χ2 = 4.670, P = .031), reading Bengali with good ability (coefficient 0.042, OR = 1.043, 95% CI = 1.002-1.086, χ2 = 4.109, P = .043, and monthly household income more than 30000 Indian rupees per month (coefficient 0.048, OR = 1.049, 95% CI = 1.000-1.101, χ2 = 4.641, P = .031) were found to have significantly higher knowledge score about the health services provided by the hospital (Table 5).
Influence of Variables on Knowledge of Health Services.

Abbreviations: SE, standard error; OR, odds ratio; CI, confidence interval; ref., reference category.
a P < .05 (2-tailed, statistically significant).
Difficulties in health service access and utilization (mean percentage 78.5, SD = 22.1) were influenced significantly by residence, understanding Bengali, monthly income. Residential distance was negatively correlated with the assessed level of difficulty, that is farther the the distance, more difficult was access to and utilization of the health care services (semiurban, coefficient −0.688, OR = 0.502, 95% CI = 0.394-0.641, χ2 = 34.359, P = .0000; rural, coefficient −0.531, OR = 0.588, 95% CI = 0.452-0.766, χ2 = 15.813, P = .0001). Understanding of the local vernacular Bengali and monthly income of Indian rupees 10 000 to 20 000 and more than 30 000 was also significantly correlated (P < .05, 2-tailed; Table 6).
Influence of Variables on Difficulties in Health Service Access and Utilization.

Abbreviations: SE, standard error; OR, odds ratio; CI, confidence interval; ref., reference category.
a P < .05 (2-tailed, statistically significant).
Discussion and Conclusion
Documentation regarding the patients’ health status, the needs and access to and use of health services is a crucial area of research. Among the main findings of this study was that the knowledge and use of health services was quite promising; however, the perceived barriers caused considerable difficulties in health service access and utilization. The study findings also highlight the necessity to consider the simultaneous influence of sociodemographic variables when considering health service access and utilization. This research suggests that there is a gradient for age, educational level, residence, language proficiency and income status within the variables considered.
Selection bias is the main limitation in this type of investigation. The study sample was composed chiefly of local people from Bengali community visiting the homeopathic hospital. This may not be representative of the entire Bengali community or of India. Despite the limitations, this study offers an insight into an extremely important issue, which is supposed to be a matter of extensive discussions with a view to formulate a common policy. We employed a small area analysis and our information was based on self-report and did not include independently documented objective measures. The cross-sectional design of our study could not capture temporal changes in the ability of patients to use and access of health services. Also, data about utilization of health services were based on self-assessments and therefore this information may be subject to recall bias. Additionally, inevitable incorporation of central tendency bias and acquiescence bias arising from the use of Likert-type scale responses into the analysis could not be eliminated. Larger scale studies including other homeopathic hospitals in India should be conducted to better understand health services knowledge and utilization among the patients.
Based on our findings, the empowerment and facilitation of the health care access and provision for patients is necessary. Depending on the needs of the population, simple measures such as comprehensive information regarding the available health services and the legal frame regarding the access is an important step toward enabling better access to needed services. Description of certain patient journeys in the system may also be proven useful. Health care professionals should be better trained in order to understand the special needs and right of patients to quality services. Public health policy measures related to appropriate coverage and adaptation of existing best practices should be taken in order the system to be better able to respond to increasing numbers of patients. Until today, no policy has been formed regarding the access and use of health care services in homeopathic hospitals in West Bengal, India mainly because of a lack of sound data. Therefore, the development of any health care policy must be evidence-based on health care needs of the patients attending the homeopathic hospital. Additionally, information is needed regarding the extent that the patients have access in health services and if that access is of satisfactory quality. Inevitably, studies regarding the health literacy and use of health care services are essential. There is a need to understand better how to ensure access to health services and how to deliver appropriate care by minimizing the obstacles faced. Appropriate care is delivered on a continuous and integrated basis, with greater attention to disease prevention and health promotion. 7 Coordinated action of government and researchers, based on best practices may succeed to improve further the ease of access of patients to health services.
There is a need for further research. On one hand, there is a need for qualitative case studies to be commissioned contextualizing the potential barriers; conversely, there is a need for quantitative research determining recommendations to solve the problems. From a theoretical perspective, the findings of this study add evidence to the role of the capability perspective in health care research. Future research should attempt to investigate on a larger scale through population surveys the representativeness of the identified factors on the patient population and link these to investigations of health-related quality of life and perceived health care needs. This will provide a more valid understanding of the importance of these factors in hindering health functioning, guide policy development and identify areas for improvement. More qualitative research should attempt to explore individual patients understanding of required health services. This research provides a starting point for assessing possible factors of accessibility problems of patients to health services provided by a homeopathic hospital. Future studies will recruit subgroups of population, subgroups with particular needs, and examine their specific accessibility problems from the viewpoints of both health service users and health professionals.
Footnotes
Acknowledgments
The authors would like to acknowledge Dr Nikhil Saha, Principal in-Charge, Mahesh Bhattacharyya Homeopathic Medical College and Hospital for allowing us to carry out the project successfully in his institution.
Author Contributions
Concept and design of study, data acquisition, interpretation of data, revising manuscript: SG. Concept and design of the study, interpretation of data, computations, drafting, and revising manuscript: SS, MK. Data acquisition: MK, RM, SP. All authors read and approved the final article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Clearance was obtained from the Institutional ethics committee prior conduct of the study.