
Abstract
Stressful life events are associated with worsening neurological symptoms and decreased quality of life in multiple sclerosis (MS). Mindful consciousness can alter the impact of stressful events and has potential to improve health outcomes in MS. This study evaluated the relationship between trait mindfulness and perceived stress, coping, and resilience in people with MS. Quality of life was assessed as a secondary outcome. One hundred nineteen people with confirmed MS completed the Five-Facet Mindfulness Questionnaire, Perceived Stress Scale, Brief Coping Orientation for Problem Experiences, Connor-Davidson Resilience Scale, and Medical Outcome Study Short Form–36. Greater trait mindfulness was significantly associated with decreased psychological stress, better coping skills, increased resilience, and higher quality of life. After investigators controlled for confounders, mindfulness accounted for 25% of the variation in perceived stress scores and 44% of the variation in resilience scores. Results support further investigation of mindfulness training to enhance psychological resilience and improve well-being for those living with MS.
Introduction
People with multiple sclerosis (MS) have long reported that psychological stress can worsen their symptoms, and studies show that chronic exposure to a wide range of challenging life events is correlated with worsening neurological symptoms in MS and increased lesion burden on brain magnetic resonance imaging 1 –4 (see references 5 and 6 for excellent reviews). Meta-analyses have found a consistent association between stressful life events and subsequent exacerbation. 7,8 While exposure to potentially stressful events is common, not everyone responds with neurological worsening. The response to stress is a dynamic and highly personalized process; innate personality traits, early life experiences, learned cognitive dispositions, and biological factors all influence an individual’s appraisal of potentially stressful events. 9 Moreover, studies show that alterations in stress physiology may affect the stress response in MS (see references 10 and 11 for review). Given that the function of the body’s major stress response systems may be altered in MS, it is particularly important to understand specific factors that influence vulnerability to stress in people with MS.
Trait mindfulness is a personality characteristic associated with psychological well-being in other populations. 12 –15 Broadly conceptualized, mindfulness is a moment-to-moment awareness of one’s present experience in an open, interested, and nonjudgmental way. Being mindful involves paying attention to one’s thoughts and feelings without overidentifying with them and without responding to them in an automatic or habitual manner. In this way, mindfulness creates distance between one’s perception and response and enables people to respond to situations more thoughtfully, potentially reducing susceptibility to the effects of stress. 16
To date, no studies have examined mindfulness as a trait characteristic in MS or how it is associated with emotional resilience. To evaluate the relationship between trait mindfulness, stress, and psychosocial correlates in MS, we conducted a cross-sectional survey (N = 119, any type of MS). Our primary objective was to evaluate the association between mindfulness, perceived stress, coping strategies, and resilience. We hypothesized that those who reported being more mindful in their daily lives (dispositional or trait mindfulness) would also report lower perceived stress, more resilience to challenging situations, and the use of more constructive coping strategies. Because mindfulness is a malleable characteristic, results will inform future interventions to improve resilience and lessen the negative effects of stress in MS.
Materials and Methods
Design, Setting, and Study Participants
Participants were scheduled for 1 visit to Oregon Health & Science University, where they completed several questionnaires. Recruitment began after approval from the institutional review board at Oregon Health & Science University. A convenience sample of men and women were recruited during their outpatient visits to the MS Center at Oregon Health & Science University. The study was also advertised with the National MS Society Oregon Chapter and through MS community events. Inclusion criteria comprised any type of MS, ability to read and write in English, and age 18 to 90 years. Exclusion criteria included a relapse or exacerbation within the previous 90 days. The diagnosis of MS was confirmed by chart review according to 2010 McDonald criteria. 17 Any questions regarding a participant’s diagnosis were discussed with his or her neurologist. Between December 2011 and February 2013, 119 people with MS were recruited, gave written consent, and completed the study.
Outcome Measures
All questionnaires used in this study are validated patient-reported outcome measures used in clinical trials involving MS and/or other stress-related disorders. Each measure asks participants to rate their feelings or thoughts on a Likert-type scale; responses typically range from 0 (never, not at all) to 4 or 5 (very often, very much so). Primary outcomes included perceived stress, mindfulness, coping, and resilience. Secondary outcomes included quality of life. The following instruments were used.
Perceived Stress Scale is a 10-question subjective measure of how unpredictable, uncontrollable, and overloaded respondents found their lives over the previous 4 weeks. 18 Total scores range from 0 to 40, and higher scores indicate increased levels of perceived stress.
Five-Facet Mindfulness Questionnaire is a 39-item questionnaire that measures 5 elements of mindfulness: observing, describing, acting with awareness, nonjudging, and nonreactivity. 19 For this study, a summed score of these 5 facets was used; higher scores indicate higher levels of mindfulness.
Connor-Davidson Resilience Scale is a measurement of one’s ability to successfully cope with challenging situations. The scale draws on a number of resilience characteristics, including patience, tolerance to negative affect, commitment, recognition of limits to control, and adaptability. 20 Scores range from 0 to 100; higher scores indicate higher levels of resilience.
Brief Coping Orientation for Problem Experiences is a 28-item questionnaire that asks participants to rate their level of agreement with statements regarding how they have been coping with stress in their lives. 21 There are 14 subscales that assess different coping strategies, acceptance, humor, planning, emotional support, positive reframing, and self-blame. Each subscale contains 2 questions. There is no overall score; each subscale is analyzed separately to identify which strategies subjects rely on. For this study, coping strategies were divided into adaptive and maladaptive strategies a priori. Adaptive strategies include the subscales Acceptance, Humor, Reframing, Emotional Support, Active Coping, Planning, and Instrumental Support. Maladaptive strategies include Denial, Behavioral Disengagement, and Self-Blame. Higher scores on adaptive and maladaptive coping mean greater reliance on those particular strategies.
Medical Outcome Study Short Form–36 is a generic measure of health-related quality of life consisting of 8 subscales. 22 Two summary scores are obtained by grouping the 8 subscales into either the Mental Health Component Summary or the Physical Health Component Summary; higher scores reflect better quality of life. The Medical Outcome Study Short Form–36 is widely used in MS trials, and its reliability and validity are well supported. 23
Covariates
We examined 7 factors that might influence trait mindfulness, perceived stress, or other psychosocial outcomes: age (continuous), gender, education (2 categories), use of MS disease-modifying therapy (yes or no), self-reported disease severity (continuous), stressful life events (continuous), and type of MS (3 categories).
MS includes 3 disease subtypes: relapsing remitting MS, secondary progressive MS, and primary progressive MS. Relapsing remitting MS is characterized by intermittent neurological dysfunction that can last for days to weeks but eventually improves. The majority of people with relapsing remitting MS will convert to secondary progressive MS 10 to 15 years after onset, at which point relapses cease and progressive neurological decline ensues. People with primary progressive MS experience progressive neurological decline from disease onset and typically do not have relapses. We controlled for type of MS because we expect that people with different subtypes will have unique concerns and stressors associated with their diagnosis.
To control for the potential impact of disability on perceived stress, 24 self-reported disease severity was generated from a 6-point scale ranging from “I have no or minimal MS–related symptoms, no limitations in walking ability, and no limitations on daily activities” to “I have many severe MS–related symptoms and am restricted to a wheelchair or bed.” We have previously shown that this self-report scale correlates with Expanded Disability Severity Scale scores (r = 0.85), a neurologist-rated, objective measure of disease severity. 25 The disability scale can be found in the appendix.
Because the experience of recent stressful life events, such as divorce, unemployment, or loss of a loved one, are likely to increase one’s level of perceived stress, 26 we used the Social Readjustment Rating Scale to control for such interactions. 27 The Social Readjustment Rating Scale is a validated checklist of 43 potentially stressful life events. Participants indicate which events they have experienced within the past year. Each event is assigned a value; more stressful events have a higher point value than less stressful events, and a total Social Readjustment Rating Scale score is generated.
Disease-modifying therapies reduce the risk of relapse and may affect quality of life. 28 Disease-modifying therapies asked about and available for use at the time of this study included glatiramer acetate, interferon-1β, interferon-1α, natalizumab, fingolimod, and mitoxantrone.
Statistical Analysis
Our hypotheses were that higher levels of mindfulness would be associated with (1) lower levels of perceived stress, (2) higher levels of resilience, (3) more use of adaptive coping strategies, (4) less use of maladaptive coping strategies, (5) better mental health–related quality of life, and (6) better physical health–related quality of life in people with MS. Mindfulness was designated as the independent predictor variable; perceived stress, resilience, adaptive coping, maladaptive coping, mental health–related quality of life, and physical health–related quality of life were dependent variables. Bivariate Pearson correlation coefficients between mindfulness and dependent variables were generated, and linear regression analysis was used to examine these associations. Three models were fitted for each dependent variable: model 1, a simple, unadjusted model with mindfulness as the predictor; model 2, a model with the covariates age, gender, education, stressful life events, disability, disease-modifying therapy status, and type of MS as the predictors; and model 3, which included the covariates in model 2 with the addition of mindfulness. Regression coefficients with 95% confidence intervals and P values were generated for mindfulness, and we used the difference in adjusted R2 between models 2 and 3 to determine how much variance in the dependent variable was explained by mindfulness (noted in the text as ▵R2). No attempts were made to replace missing data. A Bonferroni correction adjusted for MS; P values less than .008 were considered significant. All analyses were performed using STATA version 12.
Results
Sample Size and Participant Characteristics
Two hundred fourteen people with MS were approached to participate in this study (Figure 1). Sixty-four people declined to participate or did not meet inclusion criteria; 150 people completed the study visit. The Stressful Life Events Checklist (Social Readjustment Rating Scale) was added to the study after the first 27 participants had completed their visits. Because stressful life events were included as a covariate, a Social Readjustment Rating Scale score was required for analysis, and these missing data reduced our final sample size. In addition, 4 participants were dropped from analysis and some participants were unable to complete all the questionnaires (typically due to survey fatigue). Missing and excluded data resulted in final sample sizes that varied between 116 and 119.
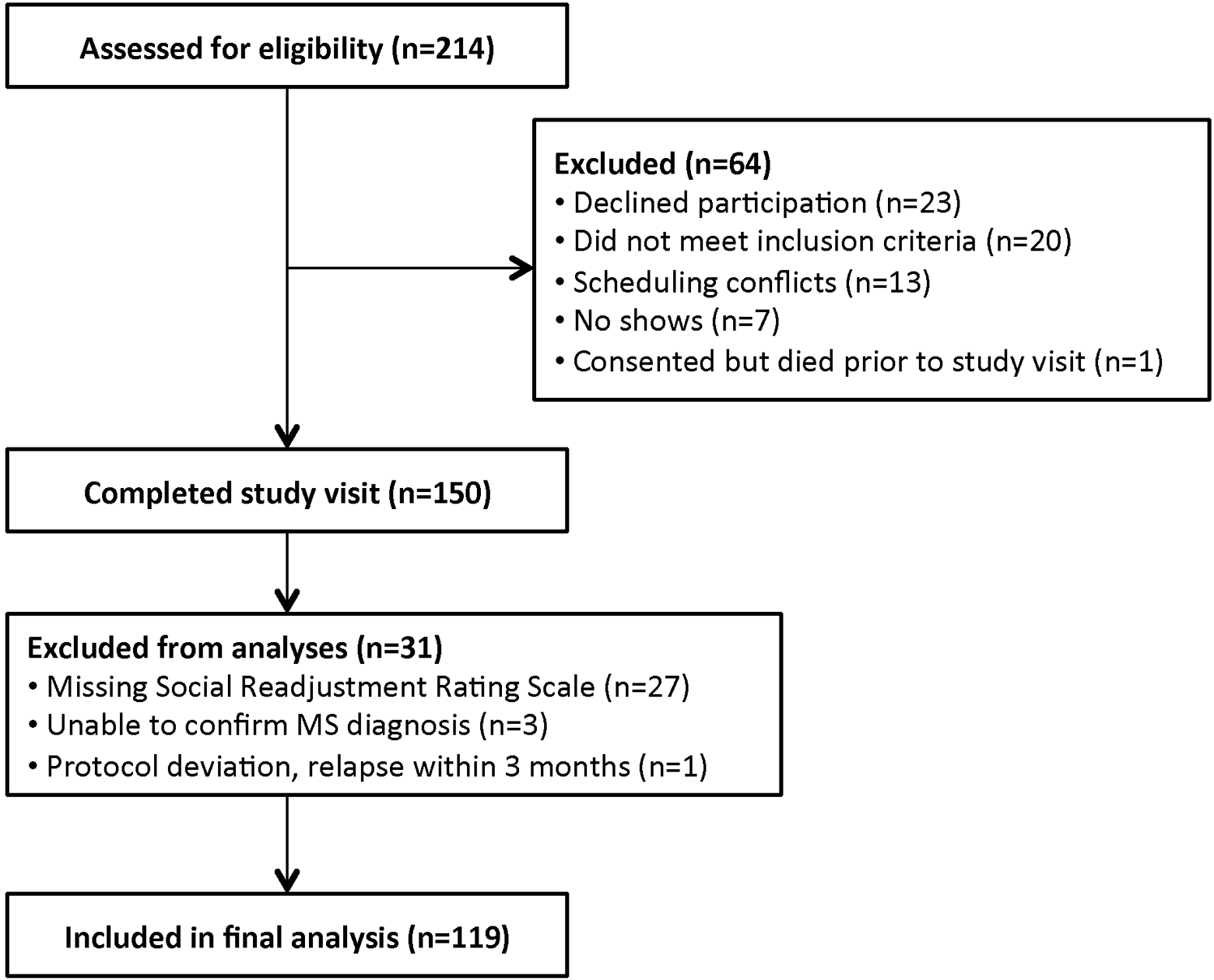
Study flow diagram.
Demographic data are displayed in Table 1. There were 86 participants (72.27%) who had relapsing remitting MS, 22 (18.49%) with secondary progressive disease, and 11 (9.24%) with primary progressive disease. The average age of participants was 51.58 ± 12.88 years, and their ages ranged from 19 to 81 years. Ninety-one percent of respondents had at least some college education and 62% had a college degree or higher. Seventy-five people (63%) were using disease-modifying therapies at the time of the study visit, including glatiramer acetate, interferon-1β, interferon-1α, natalizumab, and fingolimod. The majority of participants (69.75%) were able to walk without aid. Most of the subjects had little or no prior experience with meditation (85.7%). Descriptive data are presented for those participants who scored in the lowest and highest quartiles of the Perceived Stress Scale. Those respondents with the highest perceived stress scores (Perceived Stress Scale score ≥23, n = 33) reported less experience with meditation, higher levels of disability, and fewer years of formal education than those with the lowest perceived stress scores (Perceived Stress Scale score ≤10, n = 32). Due to the limited number of respondents in these subanalysis groups, these data should be viewed as descriptive, and future studies should confirm results with larger numbers of participants.
Demographic Data (N = 119)a.
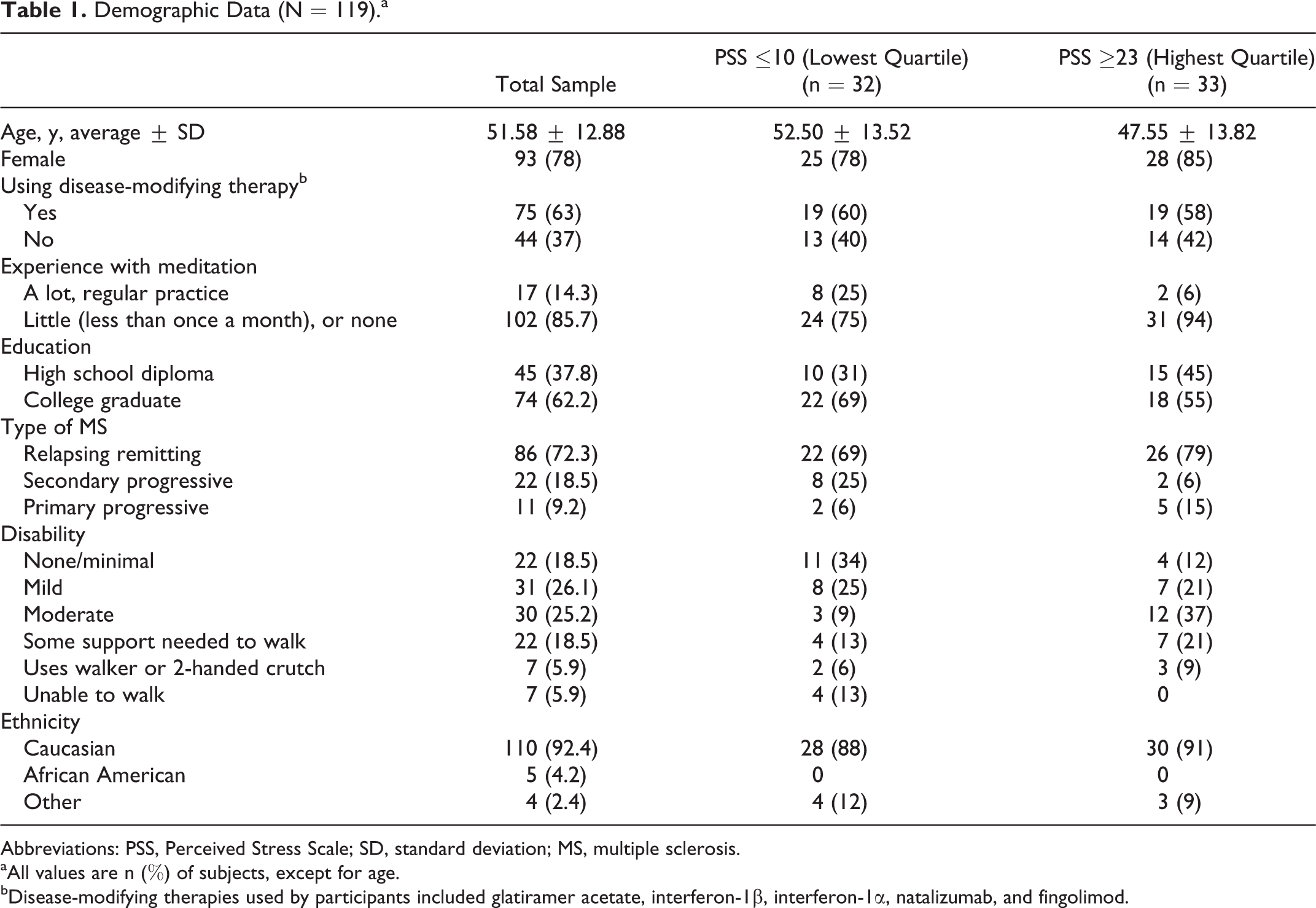
Abbreviations: PSS, Perceived Stress Scale; SD, standard deviation; MS, multiple sclerosis.
aAll values are n (%) of subjects, except for age.
bDisease-modifying therapies used by participants included glatiramer acetate, interferon-1β, interferon-1α, natalizumab, and fingolimod.
Mean scores for all outcome questionnaires are presented in Table 2.
Mean Outcome Scores.

Abbreviations: B-COPE, Brief Coping Orientation for Problem Experiences; CD-RISC, Connor-Davidson Resilience Scale; FFMQ, Five-Facet Mindfulness Questionnaire; PSS, Perceived Stress Scale; QOL, quality of life; SD, standard deviation; SF-36 MCS, Mental Health Component Summary score of the Medical Outcome Study Short Form–36; SF-36 PCS, Physical Health Component Summary score of the Medical Outcome Study Short Form–36.
Linear Regression Modeling
Correlation coefficients are presented in Table 3; the results of regression analyses are presented in Table 4. Mindfulness was significantly correlated with all outcomes except for physical health–related quality of life (Medical Outcome Study Short Form–36 Physical Health Component Summary), even after adjustment for age, gender, education, use of disease-modifying therapy, type of MS, stressful life events, and disability status. Adjusted regression analyses indicated that mindfulness accounted for 25% of the variation in perceived stress scores, 44% of the variation in resilience scores, 11% of the variation in adaptive coping strategies, 29% of the variation in maladaptive coping strategies, and 20% of the variation in mental health–related quality of life scores (as measured by ▵R2).
Raw Correlations for Mindfulness, Perceived Stress, Coping, Resilience, and Quality of Life (QOL) in Multiple Sclerosis (N = 116-119).
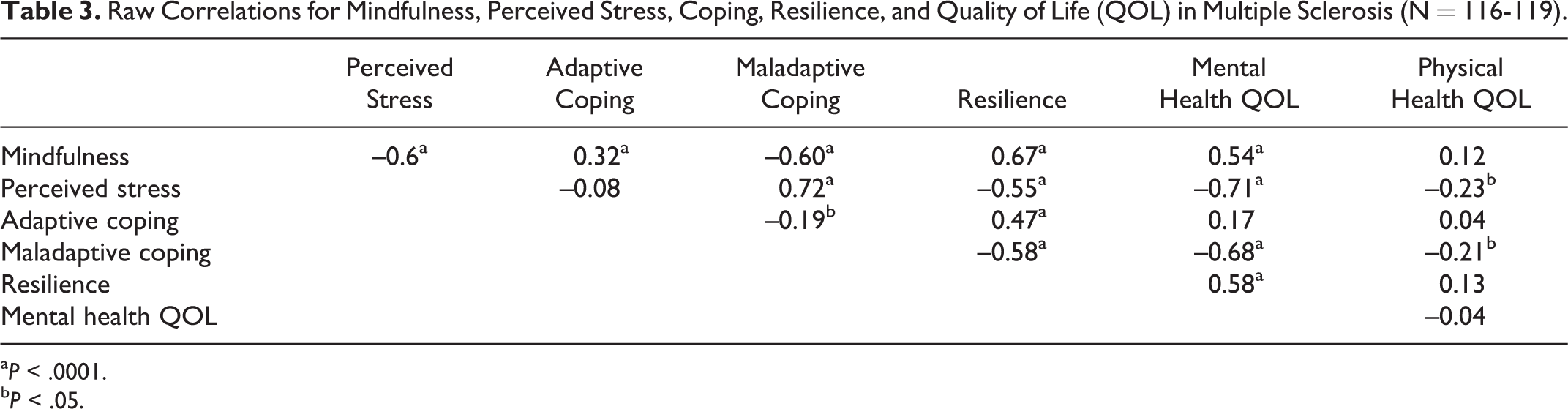
a P < .0001.
b P < .05.
Linear Regression Analyses of Mindfulness Predicting Psychosocial Outcomesa.

Abbreviations: CI, confidence interval; QOL, quality of life; SE, standard error.
aModel 1 is an unadjusted model that includes mindfulness as the predictor variable and perceived stress, resilience, adaptive coping, maladaptive coping, mental health quality of life, or physical health quality of life as the dependent variable. Model 2 predicts the dependent variable from the covariates age, gender, education, use of disease-modifying therapy, type of multiple sclerosis, stressful life events, and disability status. Model 3 includes model 2 plus mindfulness as the primary predictor variable. B is the unstandardized regression coefficient for mindfulness. ▵R2 is the difference between adjusted R2 for models 2 and 3.
Discussion
This is the first study to investigate the relationship between trait mindfulness, perceived stress, and psychosocial outcomes in MS. Those who reported being more mindful in their daily lives were more likely to report lower levels of perceived stress, the use of more constructive coping strategies, increased resilience, and better mental health–related quality of life, and the significance of these relationships was maintained after adjustment for age, gender, education, disability status, use of disease-modifying therapy, and type of MS. Our results echo findings from previous studies demonstrating that high trait mindfulness is associated with improved psychological factors in healthy and diseased populations 12,14,15,29 and extend this work by replicating results in MS. Given that the physiology of stress response systems may be altered in MS, 10,11 these findings are notable.
Stress and stress management are important topics for MS research. Current medical management of MS includes disease-modifying and symptomatic therapies, both of which have limitations in compliance due to side effects and cost. 30 While disease-modifying therapies may delay physical progression of MS, they do not completely address the psychosocial challenges faced by those living with chronic illness. 30 Many aspects of the disease process are stressful, and several MS studies show that chronic stress can lead to poorer health outcomes. 1 –4,8,31,32 Notably, Mohr et al 33 recently demonstrated in a randomized controlled trial that stress management training had a significant effect on disease activity and reduced the occurrence of new brain lesions in people with relapsing MS. Thus, identifying specific factors that may affect the susceptibility to psychological stress in people with MS is essential. While causal relationships cannot be inferred, our data suggest that trait mindfulness may influence stress perception and the response to challenging situations in people who have MS.
Mindfulness may strengthen the stress response through a relationship with coping. We found that mindfulness was related to type of coping strategy; participants who reported higher levels of mindfulness were less likely to rely on maladaptive coping strategies such as denial, disengagement, and self-blame and were more likely to use adaptive strategies such as information gathering, planning, and seeking out instrumental and social support. Being mindful involves attending to the present moment with acceptance and nonreactivity. Any thoughts, feelings, or sensations that arise are observed with curiosity and allowed to “be.” Acceptance of painful or unpleasant thoughts and feelings may change the context in which those thoughts and feelings are experienced, and in turn the subjective experience of emotional distress may become less threatening. 16 In this way, mindfulness may lessen the need to distance oneself from distressing situations and could lead to reductions in the use of avoidant coping strategies like denial or disengagement. 16 An attitude of openness and acceptance does not imply that a mindful practice is content with all distressing events; mindfulness should not be confused with complacency. On the contrary, by accepting that a distressing event is happening and observing one’s internal response with curiosity, a mindful person may be empowered to purposefully choose a response or action rather than react with automatic thought patterns and behaviors. Mindful acceptance can lead to movement and change and in this manner may enhance the use of active, adaptive coping strategies.
Interventions that can improve coping are important for MS. Several studies have found MS patients to disproportionately rely on maladaptive coping strategies, leading to adjustment difficulties, future distress, reduced quality of life, and depressive symptoms. 34 –38 Alternatively, the use of adaptive strategies by people with MS is related to improved psychological health, including lower levels of depression and better social adjustment. 34,39 Few studies have evaluated the ability of mindfulness-based interventions to influence coping style, and our results support future investigation in this area. Because the relationship between mindfulness and maladaptive coping was substantially stronger than that between mindfulness and adaptive coping, future work should evaluate the ability of mindfulness practice to disengage maladaptive coping strategies as a potential mechanism of action. Future longitudinal studies should also examine the ability of mindfulness to improve resilience.
Several mindfulness-based intervention studies use the term resilience loosely in their reporting, although few, if any, have formally assessed resilience as an outcome. We used the novel Connor-Davidson Resilience Scale to measure resilience in our sample and found a strong correlation with trait mindfulness (r = .67). Qualitatively we found little similarity between questions on the Five-Facet Mindfulness Questionnaire and the Connor-Davidson Resilience Scale, suggesting that the strength of the correlation is not due to psychometric overlap but is due to a genuine relationship that should be further explored.
There are several possible pathways by which mindfulness might improve the capacity for resilience in MS. Being mindful focuses one’s awareness on current experience. Observing and attending to the here-and-now may lead to a sense of being fully present during stressful situations with increased clarity and focus for dealing with crisis. When one purposefully focuses on the present moment, it is impossible to agonize over what should have happened or anxiously anticipate what might occur. This leads to a “slowing down” of one’s experience and is often described as room to breathe or room for choice. In this way, psychologically distressing self-talk is reduced and the mindful brain may be more able to consider a variety of solutions to complex situations.
This study examined trait mindfulness in MS, and while almost everyone has the capacity for self-reflection in this way, people differ in their tendency and ability to sustain mindful awareness; some are naturally more mindful than others. Mindfulness can be cultivated and enhanced through a variety of factors, including meditation, mind-body practices, and training programs such as mindfulness-based stress reduction. 40 Mindfulness-based stress reduction is a formalized program and the most widely researched mindfulness intervention in Western medicine. Participants take part in 1 class a week for 8 weeks in which they are instructed in mindfulness meditation, breath work, yoga postures, self-reflection, and awareness. To our knowledge, only 1 study using mindfulness-based stress reduction has been conducted in MS. Grossman et al 41 found that mindfulness-based stress reduction led to significant improvements in depression, anxiety, fatigue, and quality of life. In light of these findings, our data support further research of mindfulness training as a stress management tool for MS. Specifically, investigation of the potential for mindfulness-based interventions to improve coping strategies and enhance resilience in MS is warranted.
This study has limitations. Most participants came from a single center, and convenience sampling may have led to under- or overrepresentation of certain factors within our sample. Indeed, our participants reported higher levels of education compared with a large survey study by the North American Research Committee on MS (N = 9107). 42 Even so, education was included as a covariate in our analysis and was not found to significantly affect outcomes. Furthermore, our cross-sectional design does not allow us to determine the direction of the observed relationships. We have predicted mindfulness effects on psychosocial outcomes, but alternative models and explanations should not be ruled out. Despite potential limitations, we found highly significant relationships that warrant further investigation.
Conclusions
Trait mindfulness is significantly associated with decreased psychological stress, a more constructive coping profile, increased resilience, and better quality of life in MS. Whereas some people are naturally mindful, mindfulness is a trait that can be developed, and our data support further investigation of mindfulness training to enhance well-being and improve the experience of living with MS.
Footnotes
Acknowledgments
Results of this work were presented at the Symposium for Portland Area Complementary and Alternative Medicine Research annual meeting, May 4, 2013.
Author Contributions
AS is the principal investigator for this work; she participated in the overall design of the study, conducted the study visits, executed the analysis, and took primary lead in drafting the manuscript. DH provided statistical support and contributed to the writing of the manuscript drafts. LS and VY are co-investigators and, along with DB, provided support and mentorship necessary for the success of this work, including critical review of and contributions to the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Oregon Clinical and Translational Research Institute (grant no. UL1 RR024140 from the National Center for Research Resources and the National Center for Advancing Translational Sciences of the National Institutes of Health); the National Center for Complementary and Alternative Medicine of the National Institutes of Health (grant nos. AT002688 and 2R25AT002878-05A1); and the Agency for Healthcare Research Quality (grant no. 5T32HS017582-05). The content of this paper is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Ethical Approval
This work was approved by the institutional review board (IRB) at Oregon Health & Science University, IRB no. 7989.
Appendix
The following disability scale was included in the study:
From the choices below, check the box that best fits your condition.