
Abstract
Background
Connected health (CH) interventions may improve psychological wellbeing and quality of life (QoL) in caregivers and people with multiple sclerosis (MS); however, this impact has not been rigorously evaluated. This systematic review aims to synthesize the literature assessing CH technology's impact on psychological wellbeing and/or QoL of people with MS (PwMS) and/or their caregivers.
Methods
This systematic review's protocol is registered with International Prospective Register of Systematic Reviews (PROSPERO) with identification number CRD42023402434. CINAHL, Web of Science, PubMed, Embase, and PsycINFO databases were searched with terms relating to (a) CH; (b) MS; (c) psychological wellbeing/QoL; and (d) caregivers/people with MS. Of 2821 screened articles, 47 met the eligibility criteria, with just three including MS caregivers.
Results
Heterogenous interventions supporting self-management (n = 20 studies), education (n = 17 studies), psychological (n = 14 studies) or physical (n = 9 studies) rehabilitation and peer support (n = 5 studies) were found. CH technologies had mixed effectiveness in improving psychological and QoL outcomes, with results potentially impacted by technology type, intervention and target group. The study's findings have limited generalizability to improve access across sub-national locations, with no studies disaggregating between urban and rural residence and the majority conducted in the USA and Western Europe.
Conclusion
CH technologies show promise in improving psychological wellbeing and QoL among PwMS and their caregivers. However, this necessitates further study comparing connected health and MS subtypes to improve reproducibility and effectiveness.
Introduction
Identifying ways to support the psychological wellbeing and quality of life (QoL) in people with multiple sclerosis (PwMS) is of increasing interest to both researchers and clinicians. PwMS may experience lower QoL linked to the variability and progression of multiple sclerosis (MS) symptoms, which may lead to emotional or mental challenges.1,2 Symptoms can include difficulties with cognition, mobility and fatigue, among others, and may be followed by periods of reprieve (relapse and remit), or progressively worsen. 3 Variations in MS or sub-types can result in physical dysfunction and psychological distress, 4 which may impact QoL. 5 Compared to the wider population, PwMS have a greater risk of anxiety and depression, 6 with a reported prevalence of 22.1% and 30.5%, respectively. 7
Beyond the impact of MS on patients themselves, family members, who play varying roles supporting PwMS as informal caregivers, 8 may experience lower psychological wellbeing as a result of their caring role.9,10 In Europe, 46% of PwMS receive informal care, 11 for an average of three hours daily, with a potentially lifelong commitment. 12 Although some research on caregiver burden illustrates both positive and negative effects of caring for PwMS, 13 few studies have explored ways to better support caregivers’ psychological wellbeing and/or QoL.
To address these problems in the context of MS, psychological approaches such as mindfulness 14 or cognitive behavioural therapy (CBT) 15 may help. However, PwMS may be prevented from availing these services. 16 These barriers could be systemic, such as the shelter-in-place COVID-19 measures, 17 which impacted on the psychological wellbeing of PwMS and caregivers. 18 PwMS could also experience reduced mobility and/or disabilities that result in further needs for mobility or transportation accommodations4,19 and service flexibility, 20 that can further hinder access to needed services.
Connected health (CH), an umbrella term involving internet-mediated technologies that enable two-way communication, information processing and analysis, often between two parties, 21 may play a role in improving access to healthcare. 22 CH includes a wide range of technologies such as websites, mobile applications, wearables, social media and messaging applications, among others. Further, numerous other terminologies can be categorized as CH, including digital health, electronic health and wearable devices. 23 Taken together, research in this area has presented a fragmented view of how these technologies have been used among PwMS.
In previous reviews, Scholz and colleagues focused on eHealth excluding mobile applications, social media and gamified technology. 24 They assessed acceptance factors influencing successful use, finding user-centred design was a key determinant of the acceptance of eHealth interventions among PwMS. 24 Hessen and colleagues focused on randomized controlled trials of self-guided mobile applications excluding websites, wearables and other technologies. 25 They found a predominance of pilot studies, with significant results on outcomes including depression, but reported challenges with the methodological rigor of included studies. 25 These provide evidence about the potential for some components of CH technology in this area.
Where CH interventions were assessed in the context of MS, a report focusing on both health workers and PwMS was conducted. 26 However, to our knowledge, no systematic review has broadly examined evidence on the impact of CH interventions on PwMS. Gathering evidence in this area is particularly important for informing the provision of health and social care services, which have increasingly adopted various forms of technology since the COVID-19 pandemic. 17
There is limited assessment of the impact of CH interventions in MS, with either a direct or indirect focus on psychological outcomes. While some technologies have facilitated self-management, 27 symptom management and physical activity promotion, 26 there is paucity of evidence aggregating the impact of CH on psychological outcomes. Finally, to our knowledge, no review has explored the impact of these technologies on informal MS caregivers, who we define as any person providing support (physical, emotional or social) outside healthcare professionals, at home or within the community. Our review addresses these knowledge gaps. Specifically, this systematic review aims to synthesize the literature assessing CH technology's impact on psychological wellbeing and/or QoL of PwMS and/or their informal caregivers.
Methodology
This review employed the Preferred Reporting Items for Systematic review and Meta-Analysis (PRISMA) guidelines. 28 Its protocol is registered with the International Prospective Register of Systematic Reviews (PROSPERO) with identification number CRD42023402434. The systematic review did not deviate from the protocol.
Search strategy
CINAHL, Web of Science, PubMed, Embase and PsycINFO were searched for articles published between January 2013 and April 2023, with terms relating to (a) CH; (b) MS; (c) psychological wellbeing or QoL; and (d) patients or caregivers. The selected databases are repositories for medical (CINAHL and PubMed), psychology (Embase and PsycINFO) and general science (Web of Science) articles. Terms were informed by previous literature.21,29–32 Subject headings, MeSH, EMTREE and equivalents were searched, with findings broadened using exploded terms.
Selection criteria
Studies reporting primary data evaluating CH technology in PwMS aged ≥18 years and/or their caregivers, with psychological wellbeing and/or QoL reported as a primary or secondary outcome using validated measures, were included. All study designs evaluating a CH intervention and its effects on psychological wellbeing and/or QoL were included. Reviews, commentaries and other descriptive designs were excluded. Only those published in peer-reviewed journals in English within the past 10 years were included, reflecting the technological advancements within the period. Grey literature were excluded to ensure that conclusions were based on studies with a higher chance of methodological rigor, transparency and reproducibility. The addition of grey literature may improve methodological quality but studies are inconclusive, 33 and the risk of inability to access and retrieve included studies is higher since there are no general repositories for them. 34
Articles were excluded if any of the above inclusion criteria were not met, as were articles focusing on more than one disease that did not conduct a separate analysis on PwMS and/or their caregivers. Formal paid caregivers or healthcare professionals were also excluded (see supplementary materials for detailed search strategy and inclusion/exclusion criteria).
Screening
Database search results were exported to Endnote and then imported into Rayyan. 35 After duplicate removal, two reviewers (JA and AA) independently screened titles and abstracts for eligibility. Full texts of potentially eligible papers were independently reviewed by two reviewers (JA and AA/SS). Conflicts over eligibility were discussed between reviewers or arbitrated by LC or RM to achieve consensus.
Data extraction
JA systematically extracted data from included studies (all studies were cross-checked by AA). Using Microsoft Excel, the following data were collated: general description (including title, author, and publication year), study design and population type (including sample characteristics), CH type, outcome/measures used and results reported.
Methodological quality assessment
JA and AA independently assessed the quality of included studies using the Mixed Methods Appraisal Tool (MMAT: 36 which categorizes studies based on methodology and critically assesses quality based on design). Each study is screened by two questions and five design-specific questions (relating either to qualitative, quantitative randomized controlled trial, quantitative non-randomized, quantitative descriptive or mixed-methods studies). These generally included questions on the rationale; clarity and focus of the research question; appropriateness of the methodological approach, measures and analytical techniques used; completeness of findings and interpretation of results; and others. 36 Included studies were assessed with criteria specific to their methodological design.
Reviewers interpreted studies as high quality with 4–5 criteria met, moderate quality with 3 criteria met, and low quality with 0–2 criteria met, in line with MMAT guidelines. 36 Quality appraisals of each study were conducted to aid readers’ critical consideration of the credibility of their findings. No studies were excluded on this basis.
Synthesis of findings
Articles were initially assessed to determine homogeneity and availability for meta-analysis. The observed study diversity determined thematic analysis as appropriate to further analyse findings. 37 Data were aggregated into themes to identify connections and understand the impact of CH technologies on the psychological wellbeing and/or QoL of PwMS, and/or their caregivers. Analysis was staggered, with coding of outcomes, interventions and CH technologies done sequentially.
Initial coding frames, informed from the data, were developed by JA and reviewed by RM and LC. With consensus reached, similar codes were thematically grouped, and further consensus was ensured through discussion. Evidence patterns were captured in themes that enabled interpretation through the synthesis of findings on CH technology's impact on psychological wellbeing and/QoL. Themes were described narratively to summarize the general evidence as well as to account for CH technology's impact within each thematic area generated from analysis.
Results
Search outcome
The database searches resulted in 2821 articles retrieved, with 1591 identified for title and abstract screening following de-duplication. Of these, 186 full texts were assessed for eligibility, and 139 were excluded (see Figure 1).
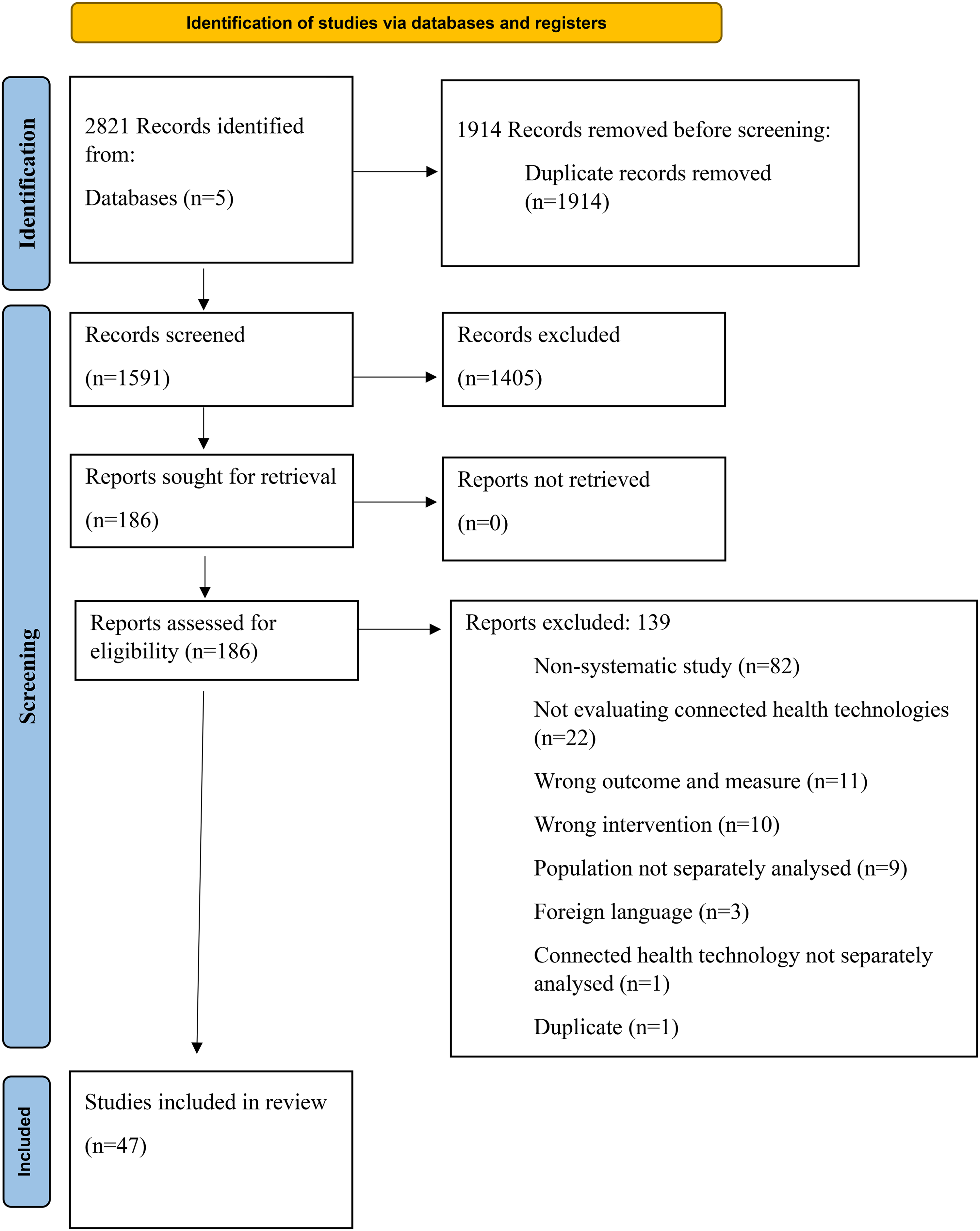
Systematic review PRISMA flow diagram.
Quality appraisal findings
Using the MMAT, 34 studies achieved a high-quality assessment; eight were of moderate quality, while five were of low quality. Evaluation results reflected variability in reported methodology and analysis of included studies. Reasons for studies’ unmet quality criteria included unclear/no information on randomization, lack of assessor blinding and participant compatibility and poor reported participant adherence to the designed intervention. Of the five studies deemed to be of low quality, four were randomized controlled trials (RCT).
Study characteristics
A description of the 47 included studies is presented in Table 1 (see supplementary materials for detailed overview). Of these, 28 were clinical trials, with three single-group trials, one two-group trial, one non-randomized control trial and 23 randomized with controls. Five studies employed a pre–post-experimental design, two used mixed methods and 11 were observational (primarily cohort) studies. One study was a natural experiment. Only six studies reported qualitative findings, largely as open-text responses to survey questions.
Summary characteristics and demography of included articles.

CBT: cognitive behavioural therapy; CT: Clinical trial; diary: for tracking progress or symptom monitoring; HRQoL: health-related quality of life; IG1: intervention group 1; IG2: intervention group 2; IVR: institutional virtual reality; M4MS: mindfulness for multiple sclerosis; MM: mixed methods; MOOC: massive open online course; MSP: MySupportPlus; N or n: numbers; Nr: not reported; QoL: quality of life; RCT: randomized controlled trial; SD: standard deviation; TR: telerehabilitation; VR: virtual reality; O: positive results not sustained at 3-month follow-up; OO: positive results not sustained at 6-month follow-up; X: demography provided for completers; XX: no separate analysis of demography done; *: PPMS; **: SPMS; ***: unsure/unknown MS type; ^: both caregivers and PwMS; !: results sustained at 3 and/or 6-month follow-up; !!: both caregivers and PwMS; !!!: both intervention and control-reported positive changes.
Three quarters of included articles (n = 35) were published since 2019, suggesting increased study on this topic in the past 5 years. Studies were conducted mainly in North America and Europe, with 13 studies based in the USA. Australia was the second most frequent study location, with six papers identified; however, a total of 15 countries were included.
Studies included a total of 4871 participants (ranging from n = 1 to 813), of whom the majority (n = 4165) were PwMS. Three studies included caregivers (total caregiver n = 205). Of these, only one 38 focused on caregivers alone while39,40 including both PwMS and caregivers. A further three studies41–43 compared PwMS to a population without MS (n = 501), while the remaining 41 studies had PwMS as a single population.
Participants were predominantly female and, for studies reporting mean age, ranged from 35 to 65 years old. The average time living with MS ranged from 5 to 41 years. Most (n = 29) studies reported participants’ MS type, with 15 including participants of all phenotypes, relapsing–remitting MS (RRMS), primary progressive MS (PPMS), secondary progressive MS (SPMS) and unknown MS type. Of the remaining 14 studies, eight included only RRMS participants, and a further five included participants reporting either RRMS or SPMS. Just one study only focused on people with progressive MS. Thirty studies reported participants’ disability status, 21 using the Expanded Disability Status Scale (EDSS), with a mean EDSS range of 2.5–6.8. Other studies (n = 9) employed Patient Determined Disease Steps (PDDS) and ambulation status to quantify mobility levels. Full details were provided in the supplementary material.
Measures
Overall, 16 studies included a measure of psychological wellbeing, 16 a measure of QoL and 15 a measure of both. Twenty-seven studies evaluated anxiety and/or depression, with the most frequently used measure being the Hospital Anxiety and Depression Scale (HADS) in 13, the Patient Health Questionnaire (PHQ-9) in nine, and the Beck Depression Inventory (BDI) in seven studies.
Assessment of QoL or health-related quality of life (HRQoL) was made using the MS Impact Scale (MSIS-29) in 11 studies and the MSQoL-54 in seven. Further details are included in supplementary materials.
Description and nature of interventions
Table 1 summarizes the interventions’ focus. Overall, 13 studies had a physical exercise focus, including six on general exercise, two on physiotherapy and one each on yoga and pilates, fall prevention, walking, Cawthorne–Cooksey rehabilitation and pelvic floor muscle training. Other study interventions delivered, singly or in combination, psychologically based approaches (n = 14), MS symptom management or other telehealth services (n = 20) or were designed as a source of information (n = 17).
Intervention durations ranged from 3 to 312 weeks, with an average duration of 20 weeks. However, most (n = 11) lasted 12 weeks. Of the 29 studies with controls, five had a waitlist, five had usual/standard care and three had an active comparator, while technical support, education and no treatment were controls in one study each. Participant engagement in study interventions varied, ranging from 10- to 90-minute sessions, once to several times weekly.
Connected health technologies
A range of CH technologies were employed in studies. In most cases, one mode of CH technology was deployed; however, seven38,48,49,57,64,68,69 studies deployed an intervention with two CH technologies, and one 83 study deployed three CH technologies. Websites or web-based programs were the most frequently used single CH technology (n = 17). These were used to deliver support groups in two62,65 studies, self-management in five45,61,63,71,82 studies, education in six39–41,51,55,58 studies and various other services (e.g. exercise activity monitoring) in four53,75,76,79 studies. A wide combination of outcomes were targeted here, mainly combinations of anxiety, depression and/or QoL.
CH-mediated teleconference (mediated entirely by the internet) was the second most frequently employed (n = 12), mainly to deliver services (primarily rehabilitation but also provision of psychological support) in ten42,46,47,52,54,60,69,73,77,78 studies. Of these, half 42,47,52,60,77 delivered telerehabilitation, with two other studies supporting learning or education.67,84
Four additional studies deployed teleconference in combination with other CH technologies. These delivered self-management, 49 education, 48 psychological support (mindfulness) 38 and tele-yoga or pilates. 69 Teleconferencing-mediated interventions mainly focused on improving QoL, as well as anxiety and depression.
Other CH technologies used included mobile apps (n = 5), tablet app (n = 1), VR (n = 2) and online computer software (n = 2). Where multiple CH technologies were employed, teleconference was a frequent component (see supplementary materials for further details).
Narrative synthesis
Psychological patient-reported outcomes included anxiety, depression, wellbeing and positive affect, as well as QoL and HRQoL. Several studies targeted these outcomes using a combination of CH technologies (see supplementary materials). The impact of interventions on these outcomes was categorized based on five thematic clusters: (a) self-management; (b) education or information provision; (c) psychological-based interventions; (d) telemedicine and telerehabilitation; and (e) support groups.
Self-management, assessment, diary feedback and symptom monitoring
Twenty studies assessed the impact of self-management/assessment, symptom monitoring and feedback on psychological wellbeing and/or QoL. Many studies delivering self-management and digital diaries utilized online or web-based programs (n = 8),45,56,61,63,71,75,79,82 a combination of website and email (n = 3)57,64,68 or website and study app (n = 1). 83 Mobile apps were the second most frequently used CH technology to promote self-management interventions (n = 4).43,50,59,81
These interventions involved an interface where self-management was promoted and included providing educational materials,45,64,68 virtual coaching or consultation56,61,81–83 or psychological support.57,63 Three studies reported that interventions were supported by telephone calls64,68,79 or reminders that were sent to participants via text message.59,64,81
Overall, the reported impact of self-management interventions on psychological wellbeing and/or QoL/HRQoL was mixed, with some positive effects observed on anxiety, depression and QoL. CH technologies utilizing self-management saw improvements in anxiety in three of five studies, depression in four of six studies and QoL or HRQoL in three of five studies. Digital diary use was associated with improvement in QoL/HRQoL in five of seven studies, although no change in anxiety or depression was observed (see Table 1 and supplementary materials for details).
One study using Fitbit sensors with a mobile app in symptom monitoring noted improvement in depression detection. 50 Another study utilizing sensors on a smartphone and mobile app found no change in QoL between participants and controls. 43 A 12-week RCT evaluating the effectiveness of a web-based personalized program along with a diary on anxiety, depression and QoL noted no improvement compared to usual care. 71 There was, however, an unexpected reduction in anxiety among controls. 71 No studies providing self-management interventions included caregivers.
In open-text responses, participants using a website for self-management revealed that connecting remotely was easy or convenient to engage with. 71 Some also discussed disadvantages they found and offered practical suggestions for improvements.71,75
Education or information provision
Seventeen studies assessed the impact of CH-delivered information and/or education on QoL, HRQoL, anxiety, depression, emotional wellbeing and/or mood, with mixed reported efficacies. Websites were the most frequently used CH technology in the delivery of these interventions.39–41,45,48,51,55,57,58,64,68,82,84 However, other media, namely, emails,67,83 software, 72 teleconferences 44 and a call centre, 84 were also used to disseminate information and education. Sixteen studies involved delivery of courses or online programs.39–41,44,45,48,51,55,57,58,64,67,68,72,82,83 Of these, one was a physical or occupational therapist-led course on fall prevention, 67 and the other deployed psychologists delivering positive psychology content. 44 Of 14 studies involving self-directed courses, four employed additional support through telephone calls 68 or website communication 45 with psychologists, remote clinicians 57 or a tele-coach. 83
Providing information or education using CH technologies was shown to have mixed but generally promising positive effects on both anxiety and depression and had a more positive effect on QoL than HRQoL. Overall, 4 of 7 studies reported improvements in QoL,48,51,55,72 1 of 3 in HRQoL 84 and 7 of 10 in anxiety40,45,48,57,58,68,72 and depression.45,48,55,57,58,68,72 Among these, improvements were found in participants with concurrent diagnosis of major depressive and/or anxiety disorder following a 5-week course focused on problem-solving. 45 However, an RCT evaluating the effectiveness of MSexpertise, a psychologist-led program on positive psychology with waitlist control, did not affect anxiety, depression or QoL. 44 Conversely, QoL improved following a longitudinal cohort study using a massive open online course (MOOC) over 6 weeks. 51 Despite other studies reporting improvements in anxiety, depression and QoL following CH technology-mediated education or information provision, effects were not sustained at 6-month follow-up in two studies, including an 8-week group psychoeducation course 48 and a 3-week combined MS education, exercise and psychological treatment program. 72
CH-mediated education or information provision had low efficacy in caregivers, with studies failing to report changes in psychological wellbeing or QoL.39,41 However, a cohort study with participating caregiver–PwMS dyads that delivered web-based education on practical skills and opportunities through role play found improvements in anxiety, emotions and life satisfaction in both groups. 40 Further, through open text, participants shared both self-empowering and relationship-strengthening experiences following their participation in the program. 40
Psychological support, training and rehabilitation
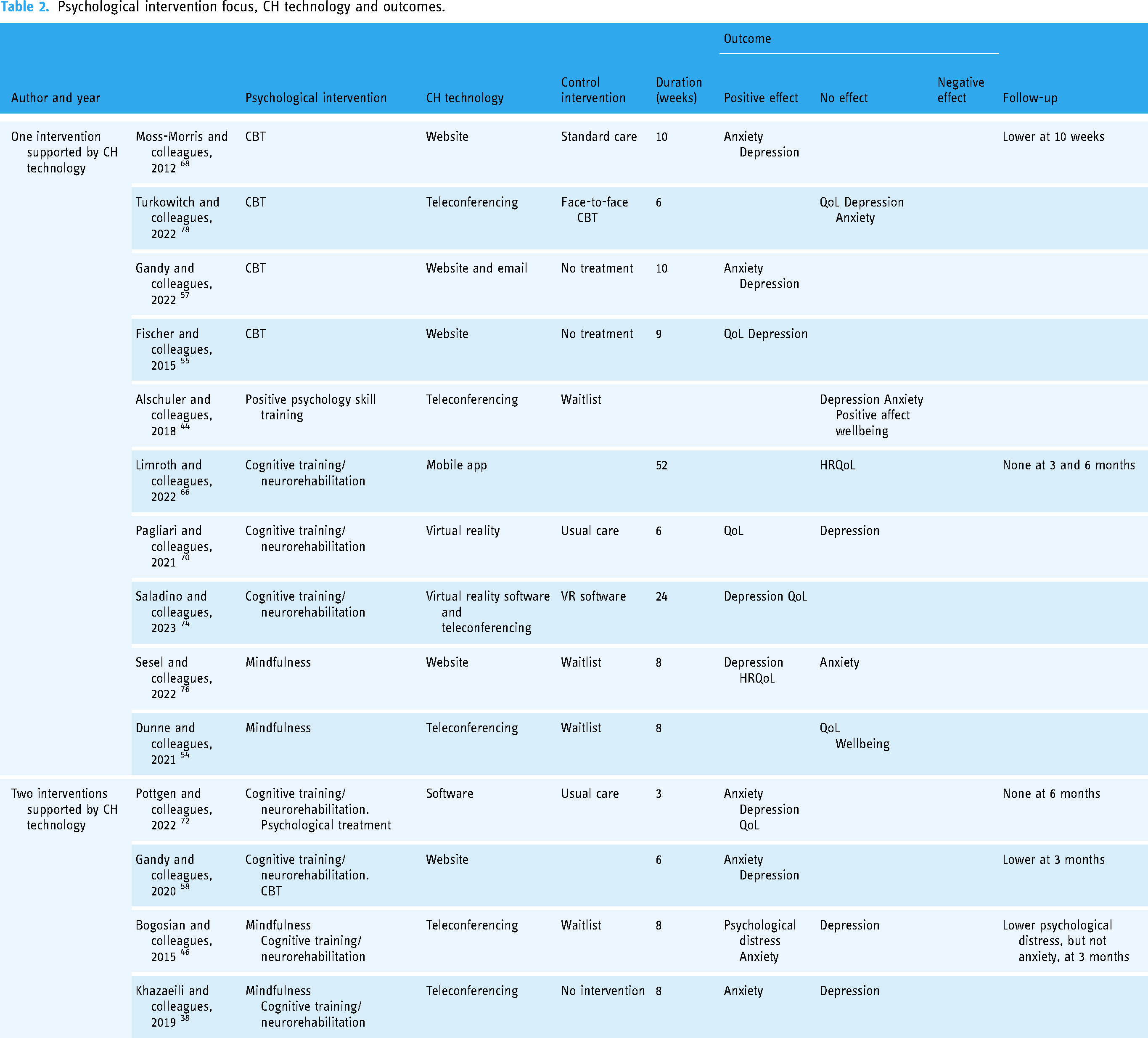
Fourteen studies employed mindfulness, cognitive training, CBT or other psychological support either singly or with other therapies using CH technologies (see Table 2). Five of these utilized websites or online programs,55,57,58,68,76 five used teleconferencing,38,44,46,54,78 three utilized software 72 including VR70,74 and one used mobile app games. 66 In some studies, participants connected with psychology professionals directly (e.g. using teleconferencing) or indirectly (using software). In others, simulations through games or VR were used.
Psychological intervention focus, CH technology and outcomes.
Cognitive training and neurorehabilitation
Half the studies in this thematic cluster (n = 7) deployed cognitive training or neurorehabilitation, either singly or in combination with other psychological support. In single deployment, cognitive training and neurorehabilitation had mixed effects, generally improving QoL but not HRQoL, and in one of two studies, lowering depression. A cohort study observing the effect of telerehabilitation along with VR exergame software for cognitive training reported lower anxiety and depression symptoms after 24 weeks, compared to VR software alone. 74 However, in another 6-week study employing VR, QoL but not depressive symptoms improved compared to usual care. 70 There was also no change in HRQoL following a mobile app, gamified, cognitive training intervention after 52 weeks or at follow-up 3 and 6 months later. 66
CH-mediated interventions deploying two types of psychological support including cognitive training and/or neurorehabilitation showed promise for improving QoL, anxiety and psychological distress, but not for depression. Anxiety and depression symptoms were reduced in two studies, including a software-mediated psychoeducation program with neuropsychological exercises and treatment, 72 and a website deploying CBT and neurorehabilitation in a single-group open trial. 58 Both studies recorded sustained impacts at 6- and 3-month follow-up. In contrast, an RCT evaluating effectiveness of teleconferencing-enabled cognitive training and mindfulness resulted in reduced anxiety and psychological distress but not depression, compared to a waitlist control. 46 Similarly, a quasi-experimental study evaluating teleconference-mediated mindfulness and cognitive therapy on caregivers alone reduced anxiety but not depression. 38
Cognitive behavioural therapy or other psychological support
Six studies employed interventions involving CH-mediated CBT or positive psychology. Most involved the study of a single psychological intervention or CBT modality, while one was combined with cognitive training. Interventions involving CH-mediated CBT alone using websites or software led to positive effects on anxiety, depression and QoL. These included a 10-week self-managed CBT program, which demonstrated improvements in anxiety and depression compared with standard care, sustained at 10-week follow-up, 68 and a 10-week website-mediated CBT intervention, supported by email or telephone support, which resulted in lower anxiety and depression compared to no treatment. 57 However, one study found teleconference-enabled CBT had no effect on QoL, depression and anxiety compared to face-to-face delivery after 6 weeks. 78
Only one study utilized website-mediated CBT along with cognitive training, with positive effects on anxiety and depression, sustained at 3 months. 58 There was no effect on anxiety, depression, positive affect and wellbeing where teleconferencing-mediated positive psychology skills training was compared to waitlist intervention. 44
Mindfulness
Four studies examined the efficacy of CH-mediated mindfulness intervention either alone (n = 2) or in combination with cognitive therapy (n = 2). Teleconferencing was employed in three studies evaluating mindfulness, with mixed effects. Mindfulness delivered as a single CH-mediated psychological intervention had low efficacy in improving psychological outcomes.54,76
Where delivered in combination with another psychological intervention, CH-mediated mindfulness therapy was efficacious in reducing anxiety but not depression. 46 Similarly, anxiety but not depression improved following a teleconference-mediated mindfulness and cognitive therapy intervention with caregivers. 38
Telemedicine and telerehabilitation
Nine studies explored the impact of CH technology-supported medical, exercise or other physical activity-related telerehabilitation services on psychological wellbeing and QoL. Teleconferencing was solely employed in six of these studies,42,47,52,69,77 including one involving teleconsultation. 73 Participants received exercise instructions or physical activity through teleconferencing, websites or software or consultations from therapists live or through video recordings.
The impact of CH-mediated rehabilitation or care provision on psychological outcomes was mixed, but improvements in QoL were observed most frequently. An RCT evaluating web software to plan and record physical activity improved HRQoL after 12 weeks compared to usual care, sustained at 3- and 6-month follow-up. 56 Further, a trial of pelvic floor muscle training improved QoL following completion compared to controls, 47 while a case study reported QoL improvements of a participant receiving diplopia rehabilitation exercises (Cawthorne–Cooksey) through teleconference. 52
Conversely, a trial providing teleconsultation through teleconferencing in addition to standard care did not improve HRQoL, anxiety or depression compared to controls over 52 weeks. 73 Another RCT exploring the efficacy of teleconference-delivered structured exercise compared to controls receiving rehabilitation with a physical therapist found no difference in QoL after 12 weeks. 77
Support groups
Five studies evaluated the impact of CH-mediated support groups on psychological outcomes including mood, 65 QoL,62,67 HRQoL, 81 anxiety,38,62 and depression.38,62 CH modalities included teleconference or online meetings62,65,67 (n = 3), anonymous interactions on study app 81 (n = 1) and social media using Telegram software 38 (n = 1). The efficacy of CH-mediated support group interventions varied across studies and outcomes, with some effect in alleviating either anxiety or depression symptoms but not QoL.
In one study involving only caregivers of people with RRMS, social media was used for 8 weeks to provide educational materials complementing teleconference mindfulness-based therapies, resulting in lower anxiety but not depression in the intervention group. 38 In another study, an app, WalkWithMe, designed to promote physical activity through walking and alleviate fatigue and cognitive symptoms used anonymous support to enhance participation and motivation over 10 weeks and was not associated with a change in HRQoL. 81
In two of the three studies using teleconferencing, participants were encouraged to share positive and negative aspects of living with MS and in one 62 discussions were also led by a psychologist. While no change in QoL was observed in either of these studies,62,67 Kever and colleagues (2022) reported lower anxiety but not depression. Another study using teleconferencing with a 12-week-long private online group did not impact QoL. 65
Generally in open-text responses, participants shared positive feelings of connectedness to peers through support groups.40,44,65,75 Support groups provided a safe and intimate space, as well as an opportunity to learn from others. 65
Discussion
This is the first systematic review to examine the impact of CH technologies on the psychological wellbeing and QoL of PwMS and their caregivers. A wide variety of CH technologies were employed across the 47 studies included, but these were mostly limited to websites and teleconferencing either alone or in conjunction with other technologies. Overall, findings suggest that CH technologies could be successful in improving psychological wellbeing and/or QoL in PwMS. However, there is a need for further robust evaluation, given the diversity of CH technologies, interventions, measures and outcomes utilized across studies. Further, only three studies included caregivers as participants, revealing a paucity of evidence supporting the effectiveness of CH technology-driven interventions in promoting psychological wellbeing in this population.
We found that interventions delivered using CH technologies have potential to support the psychological wellbeing and/or QoL of PwMS, but this was nuanced by several factors. First, the type of CH technology employed appeared to influence the impact of interventions. For instance, CH-mediated mindfulness-based interventions delivered using web programs were more effective in improving depression in PwMS than teleconferencing. Second, CH technology was more effective in delivering some types of interventions than others. For example, teleconference-mediated telemedicine and telerehabilitation focused on physical exercise or rehabilitation frequently improved QoL, while CH-mediated support groups reported no such effect. Similarly, CH-mediated interventions may have a comparable effect to traditional (in-person) approaches. For instance, CH-mediated psychological support had positive effects on psychological outcomes compared to standard care. Finally, the effects of CH-mediated interventions may depend on whether the end user is a PwMS or caregiver. For example, we found that CH-mediated education or information provision had lower efficacy in improving caregiver QoL, anxiety or depression, whereas this was often associated with improvements in anxiety, depression and QoL/HRQoL in PwMS.
Our review builds on existing knowledge about CH technology use and impact in MS. We found that QoL often improved in PwMS following telemedicine or telerehabilitation focused on exercise and physical activity. In another review, higher engagement in physical activity was found to be increase the likelihood of participants using mHealth interventions, 27 suggesting that our findings could be explained by the inclusion of relatively mobile participants in the included studies. Of studies reporting EDSS in our review, 16 had a mean participant EDSS of less than 4.5 (equivalent to the ability to walk unaided), with only five reporting a mean EDSS score of 4.5–7.5 (see supplementary materials for more details). Given that ambulation or mobility status is a key component of EDSS and an estimate of appraised disability, 85 we cannot be sure if CH technologies enabling physical activity-based telerehabilitation are as effective in improving the QoL of people with higher mobility challenges. This is an important area for additional research, given the potential of CH technologies in overcoming existing barriers to accessing in-person support for those with mobility issues, consequent inhibitive transportation or costs, 4 or those living in rural areas. 86
In their review, Gromisch and colleagues (2020) reported that mHealth was commonly used by PwMS for symptom management or to improve lifestyle and some psychological outcomes. 27 Correspondingly, we found CH-mediated self-management interventions to be the most common focus of the studies reviewed, with mixed efficacy tending towards positive impacts on anxiety, depression and QoL. Another systematic review similarly reported promising effects of mHealth-mediated self-assessment and rehabilitation tools on QoL in PwMS, although the strength of evidence was limited given the low number of included studies. 87 These mixed findings may result from the diverging methodological designs of studies conducted, revealing a need for more rigorous evidence with consistent controls. Additionally, given variability and progression in symptomatology and disability resulting from MS, our findings may not be reflective of how effectively these interventions meet MS sub-type needs, with participants predominantly reporting RRMS. There is a need for comparative studies between MS phenotypes and at different levels of disability, to garner more robust evidence about the effectiveness of CH technologies in delivering interventions to this population.
Our findings also suggest that CH-delivered CBT and cognitive training were more effective than mindfulness-based approaches in improving psychological outcomes and QoL when delivered as a lone intervention. Further, CH-mediated CBT or psychological treatment shows promise in alleviating symptoms of anxiety and depression and enhancing QoL and may be comparable to non-CH-delivered CBT. Websites or web-based programs compared to teleconferencing appear to be more effective.
A systematic review evaluating the influence of online-delivered psychological interventions on psychological outcomes and QoL in PwMS reported similar effectiveness of CBT delivered online. 88 Converse to our findings, however, they found mindfulness-based interventions equally effective and online-delivered cognitive training less effective in reducing depression and anxiety and enhancing QoL. This may be due to the variety of intervention controls employed across the studies reviewed, which may have redirected effects. These inconsistencies show that while promising, there is a need to further explore and compare the effects of different technologies on specific psychological outcomes.
The paucity of studies on caregivers found is reflective of the limited body of research focusing on MS caregiver needs20,89,90 and supportive interventions. 8 Nonetheless, we found that participating in support groups had positive effects on caregiver anxiety, 38 mirroring findings of a systematic review exploring the effectiveness of web-delivered peer support on psychological outcomes in caregivers of people with various neurological diseases excluding MS. 91 Overall, our findings indicate the potential benefit of CH-mediated support groups for caregivers of PwMS, but this requires further evaluation.
An interesting finding was that the efficacy of CH-mediated support group interventions for PwMS varied across studies and outcomes, with some alleviating either anxiety or depression symptoms but not QoL.62,65,67 In another systematic review, online peer support for PwMS was seen to provide convenience in emotional support, particularly for those living in rural areas. 92 There is a potential for CH-mediated peer support to improve psychological wellbeing; however, this requires further evaluation across multiple contexts, particularly comparing rural to urban settings, not highlighted in the studies reviewed.
Findings suggest CH-mediated interventions offer an efficacious solution to improving access for PwMS. Among studies with usual or standard care controls, findings suggest equal efficacy with telerehabilitation,73,77 self-management 71 and CBT-based psychological approaches. 78 Further, greater efficacy was observed for website-mediated CBT self-management compared to face-to-face CBT, 68 VR compared to standard cognitive training, 70 and software-based 72 or teleconference-mediated education 84 interventions in improving psychological and/or QoL compared to standard care. Overall, our findings indicate that CH technology has significant potential for the delivery of interventions to improve psychological wellbeing and/or QoL in PwMS and/or their caregivers.
Strengths and limitations
Our review has a number of strengths. Articles were generally observed to be of high quality, following systematic rigour. We also broadly examined CH technologies rather than focusing on specific types, aggregating evidence gathered during the past decade, a rapid phase of technology adaptation encompassing the COVID-19 pandemic. More importantly, we aggregated evidence in relation to both PwMS and their informal caregivers.
However, though our findings are encouraging, they only suggest possible effectiveness since causation and direction of effects cannot be attributed to specific components of the studies. Equally important, given that the CH technology field is relatively new and rapidly developing, defining its boundaries and delineating overlaps with similar concepts such as telehealth may have impacted article eligibility and inclusion in this review. Furthermore, our criteria excluded studies reported in languages other than English. With the rapid deployment of CH technologies since COVID-19, we might have missed important evaluations of these technologies reported in languages other than English. Additional studies and reports that might have been identified from backward search of citations and grey literature may also have been missed. The included studies not only differed in terms of the design and aims of the interventions, but in the outcomes measured. Even when the same outcomes were measured, different assessments were often used. The combined effect of CH technologies on psychological outcomes could therefore not be computed through a meta-analysis. There are also difficulties in comparing studies that have used different measures of the same construct, despite these measures being validated among PwMS. Thus, there is limited generalizability of findings. This is also noteworthy where no studies disaggregated between urban and rural residence, and the majority were conducted in the USA and Western Europe, making it difficult to interpret its potential to improve access across sub-national or rural/urban locations. Finally, most studies examined psychological outcomes as secondary or incidental outcomes, were primarily focused on improving mobility or fatigue, had varying population sizes and were inconsistent in evaluating the long-term impacts of CH-mediated interventions. Consequently, the conclusions reached in this study require caution and should be considered tentative due to these limitations. These also present an opportunity for further rigorous research, which follows CH concept and practice consensus. Future systematic reviews in this area should update the search to explore recent changes in a rapidly developing area.
Conclusions
Technology has been widely adopted and adapted to supplement health service provision since the COVID-19 pandemic. Technologies that enable bidirectional communication (CH technologies) have equally been employed in response to barriers limiting access to care. Our review found several pilot interventions since 2019, reflecting increasing demand and interest in these interventions, however few examined long-term effects. There is a need for policies highlighting strategic needs or areas of interest where CH technology can be employed to improve psychological outcomes in PwMS, which would encourage more robust evaluations with appropriate follow-ups to strengthen the evidence base.
The use of CH technologies to deliver interventions shows promise in improving psychological wellbeing and QoL among PwMS and their caregivers. There is, however, a need for rigorous comparative research to generate further evidence for the effectiveness of CH-mediated interventions across different MS types and for informal caregivers. Larger-scale RCTs and qualitative studies will be beneficial to drive the prioritization and scalability of relevant CH-mediated interventions to address psychological wellbeing and QoL in those affected by MS. Likewise, there is a need for development of policies to guide the deployment of CH technologies to improve outcomes for people affected by MS.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251326230 - Supplemental material for Impact of connected health on the psychological wellbeing and quality of life of people with multiple sclerosis and their caregivers: A systematic review
Supplemental material, sj-docx-1-dhj-10.1177_20552076251326230 for Impact of connected health on the psychological wellbeing and quality of life of people with multiple sclerosis and their caregivers: A systematic review by Joan Alaboson, Laura Coffey, Sowmya Shrivastava, Adeola Ade-Alao and Rebecca Maguire in DIGITAL HEALTH
Supplemental Material
sj-doc-2-dhj-10.1177_20552076251326230 - Supplemental material for Impact of connected health on the psychological wellbeing and quality of life of people with multiple sclerosis and their caregivers: A systematic review
Supplemental material, sj-doc-2-dhj-10.1177_20552076251326230 for Impact of connected health on the psychological wellbeing and quality of life of people with multiple sclerosis and their caregivers: A systematic review by Joan Alaboson, Laura Coffey, Sowmya Shrivastava, Adeola Ade-Alao and Rebecca Maguire in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors wish to acknowledge the people with living with MS as well as the MS Ireland staff, who contributed to prioritizing the focus of this study in a discussion of potential areas for research.
The authors also acknowledge the contribution of Vivienne Howard in the search process.
Contributors
All authors have equally and significantly contributed to the planning, implementation, and reporting of this study.
Data availability statement
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not required for this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication has emanated from research conducted with the financial support of Science Foundation Ireland under Grant number 18/CRT/6222.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.