
Abstract
Stress has become a global public health problem. Yoga offers one possible way of reducing stress. The purpose of this study was to look at studies from 2011 to May 2013 and examine whether yoga can be an efficacious approach for managing stress. A systematic search of Medline, CINAHL, and Alt HealthWatch databases was conducted for quantitative articles involving all schools of yoga. A total of 17 articles met the inclusion criteria. Six of these were from the United States, 3 from India, 2 from the United Kingdom, and 1 each from Australia, Brazil, Germany, Iraq, Sweden, and Taiwan. Of the 17 studies, 12 demonstrated positive changes in psychological or physiological outcomes related to stress. Despite the limitations, not all studies used a randomized controlled design, had smaller sample sizes, had different outcomes, had nonstandardized yoga intervention, and had varying lengths, yoga appears to be a promising modality for stress management.
Introduction
Stress is a widely prevalent phenomenon in modern society and has become a global public health problem. 1,2 It may account for deprived quality of life, lower mental health, reduced work efficiency, greater suffering, and increased physician visits besides being a risk factor for several chronic diseases such as coronary heart disease, hypertension, diabetes mellitus, and others. 3 Stress is conceptualized from 3 perspectives 2 : (a) response based, which has been defined from a physiological point of view by a lead proponent of this approach, Hans Selye, 4 as “a nonspecific response of the body to any demand made upon it”; (b) event based, which is based on the work of Thomas Holmes and Richard Rahe 5 and emphasizes the role of life events as being stressful; and (c) the interactional model of stress, which is based on the work of Richard Lazarus 6 and emphasizes problem focused and emotion focused coping in response to stressors. Based on these perspectives, stress can be conceptualized as the physiological and psychological response (including behaviors) as a result of encountering stressors, interpreting them, and making judgments about controlling or influencing the outcomes of these events. 7
To manage or reduce stress, several approaches are popular. These include (a) enhancing cognitive awareness of stressors and coping 6 ; (b) relaxation techniques such as biofeedback, progressive muscle relaxation, autogenic training, yoga, meditation, visual imagery, self-hypnosis 2 ; (c) improving interpersonal communication by techniques such as assertiveness and understanding behavioral style; (d) learning anger management by techniques such as active listening 8 and transactional analysis 9 ; (e) anxiety reduction techniques such as rational emotive therapy, 10 gestalt therapy, 11 and systematic desensitization 12 ; (f) incorporating healthy eating and regular physical activity 2 ; and (g) managing time. 2 Not many studies have been done to ascertain the relative efficacy of these techniques or even the efficacy of these individually. One of the techniques with which some research has been done is yoga.
The word yoga is derived from the Sanskrit word meaning union. It is an ancient system of physical and psychic practice that originated during the Indus Valley civilization in South Asia. The first written records of this methodology appeared around 200 BC in Yogasutra of Patanjali. 13 The system consisted of the 8-fold path or Asthangayoga. In contemporary literature, yoga has been described in several ways. In a more modern context, yoga has been defined as “a systematic practice and implementation of mind and body in the living process of human beings to keep harmony within self, within society, and with nature.” 14,15
The traditional practice of yoga was quite rigorous, arduous, entailed lifelong devoted practice, and adherence to strict austerities. Today, many schools of yoga have simplified the techniques making these more suitable for users in different walks of life. The 8 conventional steps of Asthangayoga consist of Yama (rules for living in society), Niyama (self-restraining rules), Asana (low physical impact postures), Pranayama (breathing techniques), Pratihara (detachment of the mind from senses), Dharana (concentration), Dhyana (meditation), and Samadhi (complete union with super consciousness). 2 Today, various schools of yoga use one or more of these techniques.
A literature review was published in 2011 that looked at all the randomized controlled trials and clinical trials till that time which has studied the effects of yoga on stress management. 16 The study summarized the results from 8 such trials and found positive effects of yoga though there were methodological shortcomings and the number of studies was too small. Since 2011, several additional studies have been published in this area. Hence, the purpose of this review was to look at these additional studies and examine whether yoga can be an alternative and complementary approach for managing stress.
Questions being addressed in this review include the following: Has yoga been found to be efficacious in alleviating stress in otherwise healthy individuals since the 2011 review? Is there sufficient data available to draw conclusions regarding the efficacy of yoga in stress management? What are the methodological limitations of the present research studies and how can these be addressed in future research? What are the common outcome measures measured by studies and which ones are more important for future studies?
Methods
A systematic review of studies involving yoga interventions for managing stress was the method used in this study. To be included in this study, the article must meet the following criteria: (a) be published in the English language; (b) included in following databases: CINAHL (Cumulative Index to Nursing and Allied Health), Medline, or Alt HealthWatch; (c) the study was conducted between January 2011 and May 2013; (d) include any form or school of yoga as an intervention; (e) use any quantitative study design for evaluation; and (f) measure at least one of the following psychological or physiological outcomes: perceived stress, positive psychological attitudes, anxiety, heart rate, blood pressure, serum interleukin, salivary cortisol, or blood lipids. Articles were excluded from this review based on the following criteria: (a) studies that did not evaluate the intervention or implemented a quantitative design; (b) did not sample apparently healthy participants; (c) did not include selected outcome measures; and (4) did not index in any of the following databases: CINAHL, Medline, or Alt HealthWatch.
Three phases of data review were conducted for this study (Figure 1). To identify studies meeting these criteria, Medline, Alt HealthWatch, and CINAHL database searches were performed for Phase I. Boolean terms used to identify studies meeting the criteria included “Yoga AND Stress” or “Yoga AND Stress Program” or “Yoga AND Stress Intervention” for the time period January 2011 to May 2013.

Flow chart depicting the three phase data extraction process.
Using the above-mentioned terms/phrases, 307 articles were returned: 129 articles from Medline, 36 from Alt HealthWatch, and 142 from CINAHL. Phase II included preliminary distillation of the articles by eliminating duplicates (n = 41), and review/discussion/other articles (n = 225), and studies not incorporating yoga in the intervention (n = 1). In Phase III, comprising manuscript review of the remaining articles (n = 22), 3 studies did not have quantitative results or did not incorporate at least one of the following outcome measures: perceived stress, positive psychological attitudes, anxiety, heart rate, blood pressure, serum interleukin, salivary cortisol, or blood lipids; one study did not mention yoga specifically; and one study did not involve healthy participants. Hence, the remaining articles (n = 17) satisfied the eligibility criteria.
Results
As a result of the data extraction process, 17 articles were found satisfying the eligibility criteria. Table 1 summarizes the studies including the year of publication, authors/country where the study was performed, study design and sample size, age of participants, intervention modality, intervention dosage, outcome measures, and the salient findings. The studies are arranged by year of publication in the ascending order starting from 2011. Within a given year studies are arranged alphabetically by the last name of the first author.
Summary of Yoga Interventions for Stress Done Between 2011 and May 2013 (n = 17).
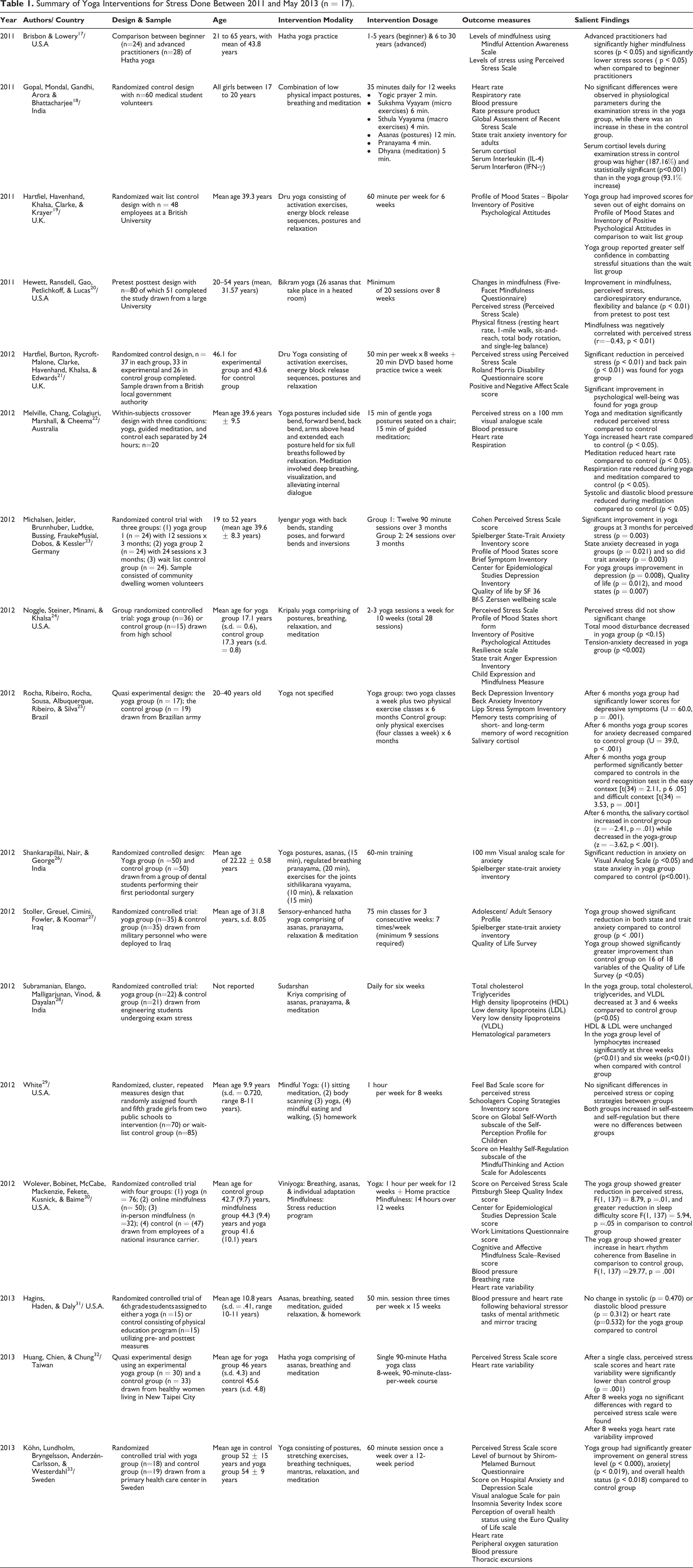
Of the 17 interventions, the majority were done in the United States (n = 6), 17,20,24,29,30,31 followed by India (n = 3) 18,26,28 and the United Kingdom (n = 2). 19,21 One study each was implemented in Australia, 22 Brazil, 25 Germany, 23 Iraq, 27 Sweden, 33 and Taiwan. 32 Of the 17 interventions, 10 were randomized controlled designs, 18,19,21,23,26–28,30,31,33 3 used group randomized controlled design, 24,29,32 2 used quasi-experimental designs, 22,25 1 used a pretest–posttest design, 20 and 1 was a comparative study between beginner and advanced practitioners. 17 The mean sample size calculated for all 17 studies in this review was 67.76, with a standard deviation of 46.87 and range of 20 to 205. Total sample sizes (n) were typically between 30 to 100, with 2 studies having sample sizes less than 30, 22,31 and 2 studies had sample sizes more than 100. 29,30 The sites of the yoga intervention for stress management were in colleges/universities (n = 5), 18–20,26,28 community settings (n = 3), 17,22,32 worksites (n = 2), 21,30 with military personnel (n = 2), 25,27 and 1 each in elementary school, 29 middle school, 31 high school, 24 and primary health care center. 33 The school of yoga was not identified by 6 studies. 18,22,25,26,31,33 It was identified as Hatha yoga by 3 studies, 17,27,32 as Dru yoga by 2 studies, 19,21 and there were 1 each of Bikram yoga, 20 Iyengar yoga, 23 Kripalu yoga, 24 Sudarshan Kriya, 28 Mindful yoga, 29 and Viniyoga. 30
The duration of yoga interventions varied from 30 minutes 22 to 6 months. 25 The mode of duration was 8 weeks (n = 4) 20,21,29,32 and 12 weeks (n = 4). 18,23,30,33 The most common outcome measure was score on a perceived stress scale, which was used by 10 studies. 17,20–24,29,30,32,33 Cohen’s Perceived Stress Scale was most commonly used to measure perceived stress. 34 Besides these, Feel Bad Scale 35 for Children and Visual Analogue Scale for perceived stress 22 were also used. Psychological outcome measures were used by all studies except for one, 28 which only used physiological measures. Physiological measures were measured by 9 interventions and included heart rate, 18,22,30–33 respiratory rate, 18,22,30 blood pressure, 18,22,30,31,33 serum cortisol, 18 salivary cortisol, 25 serum interleukin, 18 serum interferon, 18 physical fitness, 20 blood lipids, 28 hematological parameters, 28 thoracic excursions, 33 and peripheral oxygen saturation. 33
Discussion
The aim of this review was to look at studies published from 2011 to May 2013 and examine whether yoga can be an alternative and complementary therapeutic approach for managing stress. A total of 17 studies met the inclusion criteria. The first question that this review addressed was: “Has yoga been found to be efficacious in alleviating stress in otherwise healthy individuals since the 2011 review?” From the 17 studies, a majority (n = 12) 17,19–23,25–27,30,32,33 demonstrated positive changes in psychological or physiological outcome measures related to stress. Only 2 studies 29,31 showed no change in stress-related outcome measures, while 3 studies had mixed results. 18,24,28 These findings are in consonance with the previous review published in 2011, which found that 7 out of 8 studies had positive results. 16 Of the 12 studies that have shown positive results, only 8 have used randomized controlled designs. 19,21,23,26,27,30,32,33 This type of design is considered the most rigorous as it enlists pretests and posttests, randomizes the participants or their group into a control group and an experimental group, and minimizes threats to internal and external validity. In this design, changes in pretest and posttest scores can be contrasted by levels of intervention. This can be seen in the randomized control trial from Germany, 23 which had 3 groups: (a) yoga group that received 12 sessions over 3 months, (b) yoga group that received 24 sessions over 3 months, and (c) control group. The findings showed significant decrease in both the yoga groups at 3 months when compared to control group for perceived stress (P = .003), state anxiety (P = .021), and trait anxiety (P = .003) and significant improvement in scores for depression (P = .008), quality of life (P = .012), and mood states (P = .007).
On the other hand is the pretest–posttest design. Pretest–posttest design is the least costly and simplest, but is unable to minimize threats to internal validity such as maturation and history without a control group for comparison. In this review, 1 study used this design and was able to demonstrate positive changes in stress-related outcomes. This was the study from United States using Bikram yoga, 20 which demonstrated from pretest to posttest improvement in mindfulness, perceived stress, cardiorespiratory endurance, flexibility, and balance (P < .01). But without having a control group the findings can only be interpreted with caution. With regard to design, future studies should use the robust randomized control design, or it that is not feasible, as in school settings, the group randomized control design must be used.
The second and third questions this review examined were the following: “Is there sufficient data available to draw conclusions regarding the efficacy of yoga in stress management?” and “What are the methodological limitations of present research studies and how can these be addressed in future research?” The review looked at 17 studies of which 10 were randomized controlled designs. Based on these studies, some conclusions can be made but one would need to consider the limitations. Besides the design, some other shortcomings that need to be kept in mind while interpreting the efficacy of yoga in stress management are the small sample sizes used in the studies, the lack of standardization of the yoga interventions, and varying dosages of the interventions. The sample sizes have generally been small with only 2 studies having sample size more than 100. Power calculations and sample size justifications are generally missing from most of the reviewed studies. There have been no multicentric studies or large-scale studies that have been done with this research problem. Future research should look at the possibility of conducting large-scale studies. The yoga interventions have been from a variety of schools of yoga and substantial numbers do not even identify any particular school. It is essential to identify at least a few asanas, a few breathing techniques, relaxation pose (shava asana), and meditation that are common to all yoga interventions. While most interventions did mention use of these techniques, it will be important for the field to develop a checklist of essential ingredients that can be replicated. There has been a wide variability of intervention dosage that has ranged from 30 minutes to 6 months. The 30-minute intervention from Australia 22 has successfully demonstrated that yoga and meditation were able to reduce perceived stress in a short duration of time. However, long-term sustenance of effect is questionable in this short approach. Duration of yoga was not found to be linked with efficacy in this review. But most of the interventions have ranged from 6 to 12 weeks (n = 10) and that seems to be ideal both for feasibility as well as practicality. Future research should aim at developing interventions that are in the range of 6 to 12 weeks.
The final question that this review attempted to answer was the following: “What are the common outcome measures measured by studies and which ones are more important for future studies?” Both psychological and physiological measures were used by the studies though psychological measures were more common and were used by all except for 1 study. The most common outcome measure was the score on a perceived stress scale, which was used by 10 studies. There were 3 ways by which perceived stress was measured: (a) Cohen’s Perceived Stress Scale, 34 (b) Feel Bad Scale 35 for children, and (c) Visual Analogue Scale for perceived stress. 22 Cohen’s Perceived Stress Scale is in the public domain and is certainly a useful measure to use in studies examining yoga and stress. If the target population is children, then the Feel Bad Scale can be used. The common physiological measures that can be used in future studies are heart rate (and its variability), blood pressure, respiratory rate, and, if possible, salivary cortisol.
Conclusions
Stress is a major public health problem and one of the approaches to address this problem is through yoga. A total of 17 interventions from 2001 to May 2013 looked at yoga and its efficacy in alleviating stress. Of these only 12 interventions were able to find positive effects in psychological or physiological outcome measures related to stress. Despite the limitations of not all studies using a randomized controlled design, having smaller sample sizes, having different outcome measures, having nonstandardized yoga intervention, and having varying lengths of intervention, yoga is a promising modality for stress management. All practitioners teaching stress management should teach yoga as one of the approaches to stress reduction.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study did not warrant institutional review board review as no human subjects were involved.