
Abstract
Chondroid syringoma is a rare, skin appendageal tumor. It is also known as mixed tumor of skin, as it histologically resembles mixed tumor of salivary gland (pleomorphic adenoma). It is most commonly a benign tumor, but a few malignant counterparts have been described in history. It usually presents as a solid, slow-growing, solitary, and painless nodule in the head and neck region. Malignant counterpart is rare and commonly affects trunk and extremities. Early diagnosis and surgery by wide local excision are the most reliable treatments to date. Recurrences are common and hence close follow-up is advised. In this study, we present a case of malignant chondroid syringoma of face with extensive extension into nose and paranasal sinuses, which was recurrent and managed by surgical excision and radiotherapy. To the best of our knowledge, this is the first reported case with extension and bone destruction into nose and sinuses.
Case Report
A 35-year-old woman presented to the outpatient department with complaints of bilateral nasal obstruction for 1 month associated with intermittent blood stained nasal discharge. The patient also gave history of swelling over the dorsum of the nose which developed rapidly over 1 month. There was no history of headache, facial pain, or visual disturbance. There was history of similar swelling in the past over the same site for which she had undergone a minor surgery 5 years back at a different hospital and the records of the biopsy were untraceable.
On examination, there was a firm, fixed, and well-defined swelling of size 2 × 2 cm over the root of the nose in the midline. On nasal endoscopy, left nasal cavity showed a fleshy mass filling the entire cavity pushing the septum to right lateral nasal wall.
Contrast-enhanced computed tomography of the nose and paranasal sinuses showed a heterogeneously enhancing soft-tissue density over root of the nose with erosion of nasal bone and extension into left nasal cavity and filling left maxillary sinus, anterior, and posterior ethmoid sinuses and extending into right nasal cavity with erosion of bony septum (Figure 1(A) and (B)). There was no skull base or lamina papyracea erosion or any enlarged neck nodes. Fine-needle aspiration of the external nasal swelling and biopsy from the nasal mass showed scattered pleomorphic epithelial cells having hyperchromatic nuclei and scanty cytoplasm with 1 to 2 mitotic figures per high-power field, surrounded by abundant basophilic chondromyxoid stroma suggestive of malignant chondroid syringoma. Patient underwent whole-body positron emission tomography–computed tomography to rule out metastasis in lungs, liver, and skeletal system which failed to show any uptake in the site other than nose and paranasal sinus region.

Contrast-enhanced computed tomography of nose and paranasal sinuses. A, Coronal view showing a heterogeneously enhancing soft-tissue density causing destruction of the midline septum extending into the left nasal cavity, anterior and posterior ethmoid sinuses, and partially filling the left maxillary sinus with retained secretion. There is extension into the right nasal cavity, and there was no skull base or lamina papyracea erosion. B, Coronal view showing soft-tissue density anterior to nasal bone extending into nasal cavity and left maxillary sinus and ethmoid sinuses.
Patient underwent excision of the mass by external approach (lateral rhinotomy incision) along with left medial maxillectomy and excision of the external subcutaneous component (Figure 2). Postoperative biopsy confirmed the diagnosis of malignant chondroid syringoma. Patient received intensity-modulated radiotherapy 60 Gy/30 fractions, 4 weeks after the surgery. Patient was followed up every month in the first 6 months with diagnostic rigid nasal endoscopy, followed by 6 monthly interval for 2 years and found to have no further recurrence.

A, External subcutaneous swelling (white arrow). B, Excised specimen.
Discussion
Chondroid syringoma is a rare and predominantly a benign tumor of skin appendage. It is also known as mixed tumor of skin and can be eccrine or apocrine in origin. It is known to represent the cutaneous counterpart of mixed tumor of salivary glands (pleomorphic adenoma). It was first described by Hirsch and Helwig in 1961. 1
Benign chondroid syringoma is more common in males. It presents as a solitary, slow-growing, painless intradermal, or subcutaneous nodule. Tumor size varies from 2 mm to >1 cm. Chondroid syringoma accounts for 0.01% to 0.1% of primary skin tumors. 2 The median age of both benign and malignant chondroid syringoma patients is 49 years, ranging from 13 to 83. In contrast to benign counterpart, malignant cases though very rare, it is more common in females. 2 Only 43 cases of malignant chondorid syringoma have been reported in literature. 3 The site of the primary tumor was the lower extremity in 35%, the head in 28%, and the upper extremity in 23%. 3 The benign tumor usually involves the head and neck region, while the malignant ones involve the trunk and extremities. 4
The patient is a middle-aged woman, who had a small subcutaneous mass over the dorsum of the nose associated with nasal symptoms like obstruction and discharge. Since both developed in the same time frame, this deceived us into thinking it to be a malignant nasal tumor probably squamous cell carcinoma or adenocarcinoma with extranasal extension into subcutaneous tissue. Diagnosis of chondroid syringoma was only confirmed by fine-needle aspiration cytology from the external nasal swelling and biopsy from the nasal mass. Due to their unremarkable clinical presentation, diagnosis of chondroid syringoma can be made only by histopathology.
Histopathological features of chondroid syringoma include (1) nests of cuboidal or polygonal cells, (2) intercommunicating tubule-alveolar structures lined by 2 or more rows of cuboidal cells, (3) ductal structures composed of 1 or 2 rows of cuboidal cells, (4) occasional keratinous cysts, and (5) a matrix of varying composition. Chondroid syringoma may have all 5 features or only some. 1 Histopathological features in the present patient were sheets of polygonal cells arranged in cords with tubule-alveolar structures in between dispersed in a chondromyxoid stroma. The cells were showing hyperchromatic nuclei with atypia and pleomorphism (Figure 3).
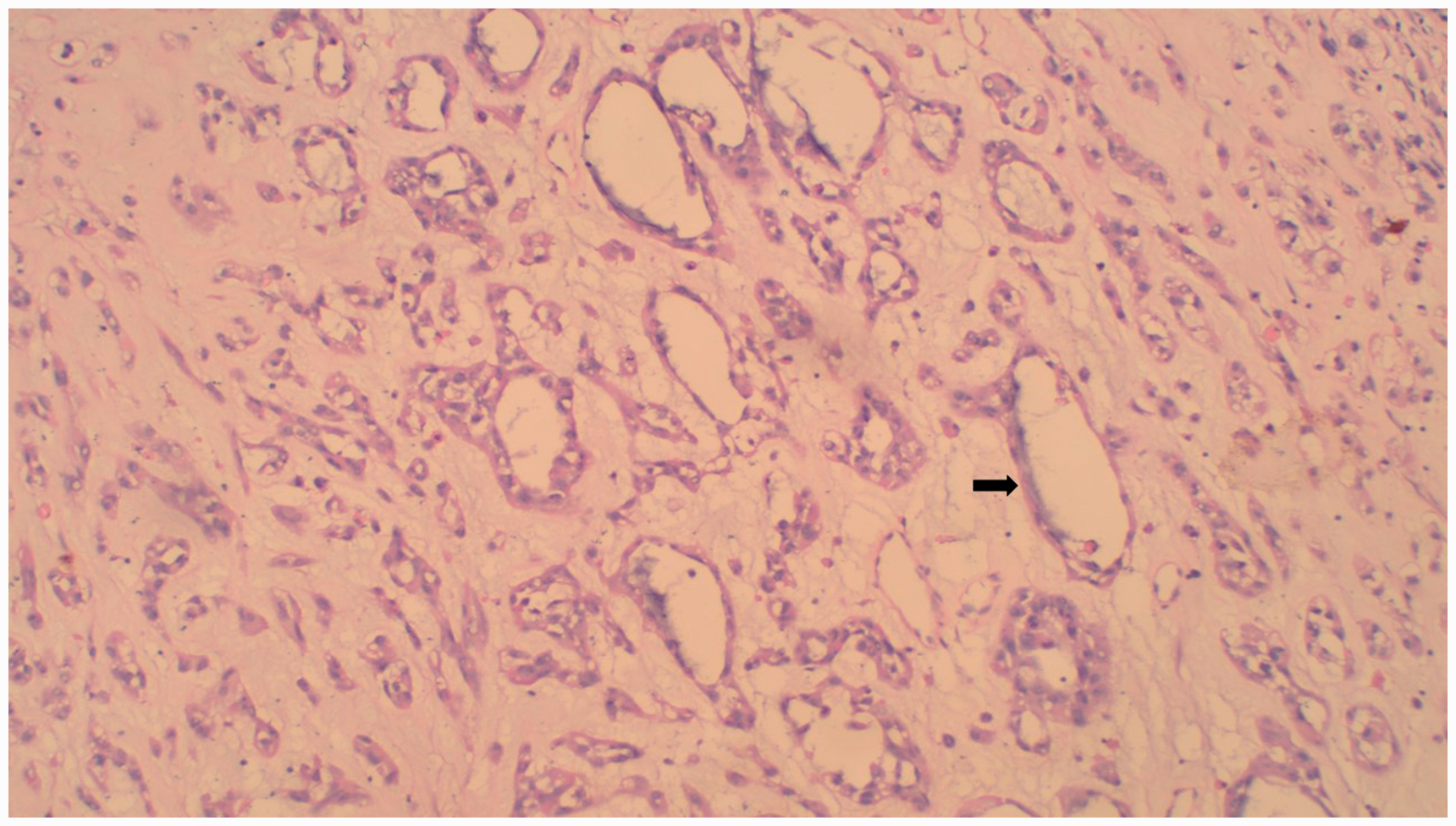
Histopathological picture (hematoxylin and eosin stain, 400× magnification) showing tumor cells arranged in the form of duct-like structure (black arrow) with chondromyxoid background.
Malignant chondroid syringoma can occur de novo or rarely develop in a preexisting benign chondroid syringoma tumor. 2 There is no known predisposing risk factors for malignant transformation. Our patient had history of similar swelling 5 years back over the dorsum of the nose without history of nasal obstruction or discharge at that time. This indicates the tumor was confined to the subcutaneous plane and hence it was excised by a minor procedure. The tumor has recurred 5 years later with a malignant potential causing bone destruction and extension into nasal cavity and paranasal sinuses. Recurrence in our case could probably be due to improper excision at the first time. Recurrence of the lesion alerts the clinician to the possibility of malignancy. 5 Approximately 49% of malignant chondroid syringoma patients have local recurrence. The incidence of nodal and distant metastasis was approximately 42% and 40%, respectively. The period of recurrence ranges from 1.5 months to 6 years with average time period being 23 months, 50 months, and 66 months for local recurrence, nodal metastasis, and distant metastasis, respectively. 3
Treatment of chondroid syringoma is complete excision. Adequate disease-free margin is essential for disease control and to prevent recurrence.5,6 Complete excision of the mass was done by lateral rhinotomy approach to gain access into nose and paranasal sinuses. Medial maxillectomy was done to remove the mass from maxillary antrum and ethmoids. Clinically and radiologically, there was no nodal involvement and hence neck was not addressed in the management.
Radiotherapy and chemotherapy have no proven value in treatment, and adequate surgical excision with wide disease-free margins is the best way to achieve disease control. Chemotherapy and radiotherapy are administered to patients with advanced disease.
Barnett et al. recommended adjuvant radiotherapy for all chondroid syringomas showing signs of aggressiveness or cytologic atypia, regardless of whether it is an initial presentation or a recurrence, because of the seemingly unpredictable nature of this disease and the difficulty faced in removing it completely by excision in areas like face. 7 The present patient received intensity-modulated radiotherapy 60 Gy/30 fractions, 4 weeks after the surgery since it was an aggressive and advanced disease.
Malignant chondroid syringoma follows an unpredictable clinical course. The most common site for distance metastasis is lung, followed by bone and brain.6,8 Fortunately, our patient did not have any nodal or distant metastasis.
In conclusion, the diagnosis of malignant chondroid syringoma should be kept in mind in case of nasal mass associated with a skin swelling around the face. Treatment involves early and complete excision of the tumor. Patients should be kept on close follow-up, as this condition has high propensity for recurrence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by our institutional review board.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was obtained from the patient involved in the study.