
Abstract
Background
IgG4-related disease is a new clinical entity frequently associated with swelling of the submandibular glands (SMGs). The long-term outcome of SMG swelling without steroid therapy remains unknown.
Objective
To examine whether swollen SMGs spontaneously regress without steroid therapy in the context of IgG4-related disease and to identify biomarkers that can predict the spontaneous regression of SMG swelling.
Methods
The SMG volume of 49 patients diagnosed with IgG4-related disease was calculated by measuring the axial and coronal planes of computed tomography scans. The change in SMG volume over time was measured and examined by treatment regimen, clinical data, and serum complement level.
Results
We found 28 of 49 (57%) IgG4-related disease patients to have swollen SMGs, with 15 of 20 (75%) of the swollen SMGs regressing without steroid therapy. The time required for the SMGs swelling to regress was significantly shorter in the steroid therapy group than in the no-steroid therapy group. Serum complement components at the initial visit were significantly lower in the regressed SMG group than in the nonregressed SMG group.
Conclusion
We observed 75% of swollen SMGs spontaneously regressed in patients with IgG4-related disease. The time required for the swollen SMGs to regress was longer in patients without steroid therapy than in those with steroid therapy. Serum complement level could be used as a predictor for the spontaneous regression of swollen SMGs in patients with IgG4-related disease.
Keywords
Introduction
Immunoglobulin (Ig) G4-related disease is a new systemic syndrome, characterized by a high serum concentration of IgG4 and infiltration of IgG4-positive plasma cells into affected organs. 1 IgG4-related disease is known to affect multiple organs including the pancreas,2,3 lacrimal and salivary glands, 4 kidneys, 5 bile duct, 6 prostate, 7 nasal cavity,8–10 skull base, 11 and retroperitoneum. 3 In particular, swollen submandibular glands (SMGs) are one of the most typical manifestations of IgG4-related disease.
It is widely known that steroid therapy is effective for IgG4-related disease and can induce the regression of SMG swelling. 12 However, some IgG4-related disease patients with swollen SMGs do not have any other clinical symptoms or affected organs, and it has been controversial whether these patients should be treated with steroid therapy or not. 12
Some manifestations of IgG4-related disease have been reported to show spontaneous regression.13–16 However, the spontaneous regression of swollen SMGs in the context of IgG4-related disease has not yet been reported. The long-term outcome of SMG swelling in the context of IgG4-related disease also remains unclear.
In this study, we determined the ratio of regression of swollen SMGs in the context of IgG4-related disease. We compared the clinical course of swollen SMGs in patients with IgG4-related disease that were treated with steroids to those that were not treated with steroids. We also examined clinical factors and serum complement levels to identify biomarkers for predicting the spontaneous regression of SMG swelling in these patients.
Materials and Methods
Patients
We retrospectively examined patients diagnosed with IgG4-related disease in the Department of Otolaryngology, Hokkaido University Hospital, between September 2006 and October 2014. A diagnosis of lgG4-related disease was made according to the comprehensive diagnostic criteria for definite IgG4-RD: (1) diffuse or partial enlargement, swelling, nodules, or thickening lesions on single or multiple organs; (2) a serum IgG4 concentration > 135 mg/dL; and (3) histopathological findings including (a) massive lymphocytic and plasmacytic infiltration and sclerosis, (b) increased numbers of IgG4+ plasma cells, and (c) IgG4+/IgG+ plasma cell ratio >40% and >10 cells per high-power field. 1 Patients were excluded if they had been diagnosed other diseases, such as sarcoidosis, Castleman’s disease, granulomatosis with polyangiitis, sialolithiasis, and malignant disease.
Patient age, sex, complications, affected organs, laboratory data, computed tomography (CT) scans, and follow-up period were retrospectively examined on the basis of clinical records. As controls, we also examined 29 healthy subjects (HS) without any symptoms of xerostomia or keratoconjunctivitis sicca and no history of radiation therapy.
This study was approved for Clinical Research (014-0373) by the Institutional Review Board of the Hokkaido University Hospital, Hokkaido, Japan, and complied with the ethical standards of the Helsinki Declaration.
Steroid Treatment
Oral prednisolone was started at 30 to 40 mg per day for 2 to 4 weeks and thereafter reduced gradually (by 5 mg per week) to a daily dose of 5 mg. When patients had rejected the proposal of steroid therapy, they were closely followed without any treatment.
Measurement of SMG Volume
SMGs were examined on the axial and coronal planes of CT scans. SMG volume was calculated according to the following formula:
17

No cut-off value for the enlargement of the salivary gland lesions of IgG4-related disease has been established. In the present study, the cut-off value for the enlargement of the SMGs was set at the mean volume of the SMGs in the control group + 1.64 standard deviations (SDs) so that 95% of all observations in a healthy population are judged as normal. We judged a SMG to be swollen if the volume of the SMG was over the cut-off value. We defined a SMG as showing regression if the swollen SMG was found to be under the cut-off value in the later CT scan.
Statistical Analysis
All data are expressed as mean ± SD. Categorical variables, such as sex, the presence/absence of DM, hypertension (HT), and hyperlipidemia (HL), and other complicating lesions (lacrimal glands, parotid glands, sublingual glands, pancreas, gall bladder, kidney/retro peritoneum, and lung/mediastinum), were compared using the χ2 test and/or the Kruskal–Wallis test. Continuous variables (age, serum IgG level, serum IgG4 level, complement level, HbA1c, volume of SMGs, and follow-up period) were analyzed using the Wilcoxon test. The correlation between the serum IgG4 and the volume of SMGs was tested using Pearson’s correlation coefficient; r.
The Kaplan–Meier method was applied for the ratio of the regression of the swollen SMGs. The time of interest was the duration from the date of the first visit to regression of the swollen SMGs. The period for the swollen SMGs to regress was analyzed by Log-rank test. P values < .05 were considered statistically significant. All analyses were performed using the JMP® 11 (SAS Institute Inc., Cary, NC).
Results
Clinical Features of Patients With IgG4-Related Disease
We examined 49 patients with IgG4-related disease. Fourteen (28.6%) of the patients were women and 35 (71.4%) were men. The mean age was 68.2 ± 10.8 years (range, 38–81 years). The mean IgG and IgG4 serum level was 2187.8 ± 604.5 and 646.5 ± 501.9 mg/dL, respectively. Twenty-eight patients (57.1%) suffered from autoimmune pancreatitis (AIP) and 21 (42.9%) suffered from sclerosing cholangitis. The follow-up period was 46.3 ± 28.5 months (range, 0–92 months). Twenty-two patients (44.9%) received steroid therapy. The SMG volume in patients with IgG4-related disease was 9.79 ± 4.77 mL. On the other hand, the volume in the HS group was 6.70 ± 1.94 mL. Hence, the cut-off value for swollen SMG was set at 9.9 mL according to the formula given earlier.
Comparisons of Clinical Features Between the Patients With and Without Swollen SMGs
Twenty-eight patients (57.1%) had swollen SMGs, whereas the other 21 patients (42.9%) did not have swollen SMGs. Twelve patients had unilateral SMG swelling and 16 patients had bilateral SMG swelling. Clinical features were compared between patients with and without swollen SMGs (Table 1). The patients with swollen SMGs were significantly younger than the patients without swollen SMGs (65.64 ± 12.25 vs 72.81 ± 7.51, P = .024). The patients with swollen SMGs were less likely to suffer from AIP than the patients without swollen SMG (42.8% vs 76.2%, P = .018). There were no differences in sex, the presence/absence of DM, HT, or HL, other affected organs, serum IgG, serum IgG4, serum complement (one data on a patient treated with steroid therapy for swollen SMGs was missing.), HbA1c, or follow-up period. Serum IgG4 did not have a significant correlation to the volume of SMGs (r = .280, P = .346).
Comparison of Clinical Features Between Patients With IgG4-Related Disease With and Without Swollen SMGs.

Abbreviations: DM, diabetes mellitus; HL, hyperlipidemia; HT, hypertension; PSL, prednisolone; SMG, submandibular gland, *P< .05.
Data are mean ± standard deviation.
Of the 28 patients who had swollen SMGs, 14 patients were treated with steroid, and the remaining patients were not. Only 1 patient treated with steroid for swollen SMGs also used azathioprine. There were no significant differences in any clinical data, except for HT, between the patients with and without steroid therapy (Table 2).
Comparison of Clinical Features in the Patients With Swollen SMGs With or Without Steroid Treatment.
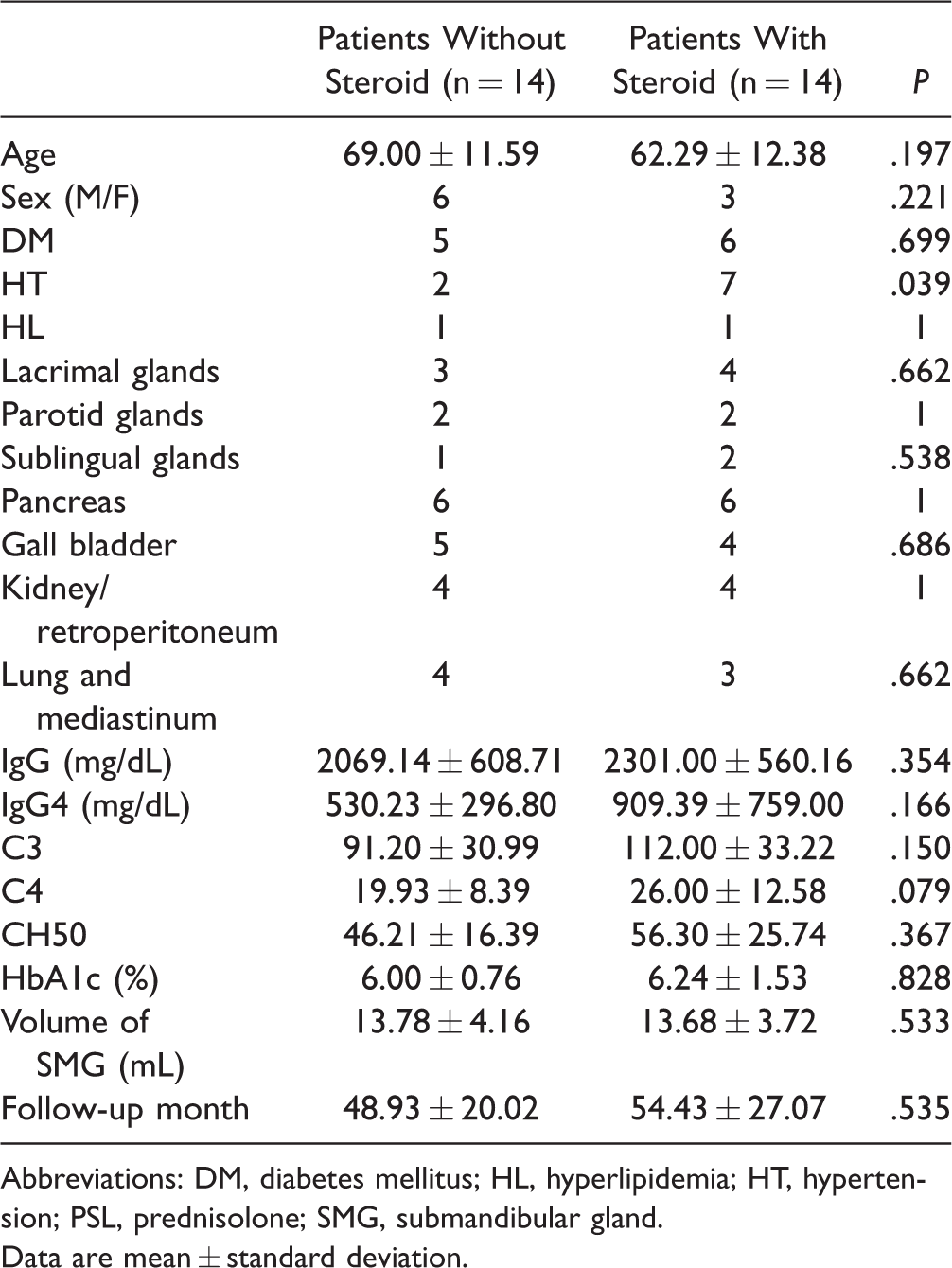
Abbreviations: DM, diabetes mellitus; HL, hyperlipidemia; HT, hypertension; PSL, prednisolone; SMG, submandibular gland.
Data are mean ± standard deviation.
Comparisons of Clinical Features Between Patients in Whom SMG Swelling Regressed and Those in Whom There Was No Regression
Of the 28 patients who had swollen SMGs, 26 patients were examined with CT scans at least twice. Among the 26 patients, 13 patients did not receive any steroid therapy, and in these patients, a total of 20 SMGs were swollen. We found that 15 of the 20 swollen SMGs (75.0%) spontaneously regressed without steroid therapy (regressed SMG group), while the other 5 SMGs did not (nonregressed SMG group). There were no significant differences between the 2 groups in terms of age, sex, the presence/absence of DM, HT, or HL, other affected organs, serum IgG, serum IgG4, HbA1c, or follow-up period (Table 3). There was no significant difference in the change of serum IgG4 (ΔIgG4) between them (479 ± 727.28 mg/dL vs 393.08 ± 501.23 mg/dL, P = .36).
Comparison of Clinical Features Between Regressed SMGs and Nonregressed SMGs Without Steroid Therapy.

Abbreviations: DM, diabetes mellitus; HL, hyperlipidemia; HT, hypertension; PSL, prednisolone; SMG, submandibular gland, *P<.05.
Data are mean ± standard deviation.
Change in Volume of the Swollen SMGs
In the regressed SMG group without steroid treatment, a significant difference was observed in SMG volume in the pre-CT and post-CT (14.17 ± 4.89 mL vs 4.27 ± 1.71 mL, P < .01; Figure 1(A) and (C)). On the other hand, in the nonregressed SMG group, there was no significant difference in SMG volume in the pre-CT and post-CT (12.96 ± 2.34 mL vs 11.38 ± 1.35 mL; Figure 1(B) and (C)). Further, there was no significant difference in the SMG volume in the pre-CT between the regressed SMG group and the nonregressed SMG group (14.17 ± 4.89 mL vs 12.96 ± 2.34 mL; Figure 1(C)).

Changes in the volume of SMGs in patients with swollen SMGs and no-steroid therapy. A, Change in the volume of each SMG in the regressed SMGs. B, Change in the volume of each SMG in the nonregressed SMGs. C, Change in the mean volume of each SMG in patients with swollen SMGs and no steroid therapy. SMG, submandibular gland, *P < .05.
Comparison of the Time Required for the Swollen SMGs to Regress With/Without Steroid Therapy
The time required for the swollen SMG to regress was significantly shorter in patients who received steroid therapy than in those without steroid therapy (5.03 ± 8.18 months vs 29.76 ± 11.94 months, P < .001; Figure 2(A)). There was also a significant difference in the Kaplan–Meier curve for the ratio of regression of SMGs with and without steroid therapy (P = .003; Figure 2(B)). The median time to regression in patients with and without steroid therapy was 4.2 and 36.5 months, respectively.

Comparison of the time required for the swollen SMGs to regress with/without steroid therapy. A, Comparison of the time required for each SMG to regress between with and without steroid therapy. B, Kaplan–Meyer curve on the ratio of regression of swollen SMGs between with and without steroid therapy. SMG, submandibular gland, *P < .05.
Complement Level Was Associated With the Spontaneous Regression of Swollen SMGs Associated With IgG4-Related Disease
The level of serum C3, C4, CH50 measured at the first visit was significantly lower in the regressed SMG group than in the nonregressed SMG group (C3 88.40 ± 15.41 mg/dL vs 125.40 ± 24.17 mg/dL, P = .004; C4 19.47 ± 4.52 mg/dL vs 28.20 ± 5.63 mg/dL, P = .014; and CH50 46.15 ± 8.45 U/mL vs 64.74 ± 13.10 U/mL, P = .008, respectively; Table 3 and Figure 3(A)).

Complement level was associated with the spontaneous regression of swollen SMGs associated with IgG4-related disease. A, Comparison of complement levels at the initial visits between the regressed SMGs and nonregressed SMGs. B, Change in CH50 level before and after the spontaneous regression of swollen SMGs. SMG, submandibular gland, *P < .05.
In the regressed SMG group, the level of serum CH50 recovered as the SMGs regressed (Pre-CH50 46.15 ± 8.45 U/mL vs Post-CH50 53.53 ± 8.89 U/mL, P = .048). On the other hand, the level of serum CH50 did not change in the nonregressed SMG group (Pre-CH50 64.74 ± 43.48 U/mL vs Post-CH50 66.63 ± 10.23 U/mL; Figure 3(B)).
Representative Case
A 75-year-old man was referred to our hospital due to nasal crusting and swelling of the bilateral SMGs. He had a history of asthma.
Physical examination revealed symmetrical swelling of the SMGs and nasal crusting. There were no other abnormalities in the head and neck region. Immunoglobulin analysis of peripheral blood showed elevated serum IgG (1821 mg/dL) and IgG4 (312 mg/dL) levels. Serum C3, C4, and CH50 levels were 67 mg/dL, 19.0 mg/dL, and 37.5 U/mL, respectively. Autoantibodies, such as rheumatoid factor, proteinase-3–antineutrophil cytoplasmic antibody (ANCA), myeloperoxidase-ANCA, anti-SS-A antibody, and anti-SS-B antibody, were all negative. A cervical CT scan showed bilateral swollen SMGs (right 16.9 mL and left 25.0 mL; Figure 4(A)). Specimens were taken from his labial salivary gland, nasal mucosa, and pancreas. Histopathological examination showed chronic inflammation with dense lymphoplasmacytic infiltrates. Immunostaining for IgG and IgG4 showed numerous IgG4-positive plasma cells (>100/HPF) in both his labial salivary gland and nasal mucosa. The infiltration of numerous IgG4-positive plasma cells was also detected in the specimen from his pancreas (Figure 4(B)). Taken together, he was diagnosed with IgG4-related disease including AIP and bilateral swollen SMGs.

Cervical computed tomography and pathological findings of the representative case. A, A cervical CT scan showing bilateral swollen SMGs (right 16.9 mL and left 25.0 mL). B, IgG4 immunostaining of pancreas specimens from the representative case. C, A cervical CT scan 50 months later reveals regression of the bilateral swollen SMGs (right 3.4 mL and left 5.2 mL) without steroid therapy. CT, computed tomography; SMG, submandibular gland.
The patient, who presented with only mild symptoms, did not accept steroid therapy for fear of its side effects and was closely followed without steroid therapy. The bilateral swollen SMGs gradually regressed.
Fifty months later, a cervical CT scan revealed regression of the bilateral swollen SMGs (right 3.4 mL and left 5.2 mL; Figure 4(C)). Laboratory examination revealed that the serum C3, C4, and CH50 levels were also recovered (C3 78 mg/dL, C4 29.0 mg/dL, and CH50 45.3 U/mL).
Discussion
There are some case reports in which the lesion affected by IgG4-related had spontaneously regressed.13–15 Seki et al. have described a 67-year-old man with chronic sclerosing sialadenitis and lung lesions, which regressed after resection of the SMG lesion without steroid therapy. 14 Ozden et al. have reported spontaneous regression of AIP. 13 Kase et al. have reported a 65-year-old woman with bilateral IgG4-related dacryoadenitis, which spontaneously regressed after excision of the left lacrimal gland. 15 However, spontaneous regression of the swollen SMGs in IgG4-related disease has not been reported to date.
It has been widely assumed that swollen SMGs in patients with IgG4-related disease were persistent and that only steroid therapy could shrink swollen SMGs. 12 However, in this study, 75.0% of swollen SMGs later regressed without steroid therapy. This discrepancy might depend on the observation period. In this study, the patients with IgG4-related disease were followed for a relatively long period of 46.3 ± 28.5 months. Furthermore, it took much longer for the swollen SMGs to regress without steroid therapy than with steroid therapy. These results imply that the swollen SMGs could shrink even without steroid therapy long term, but steroid therapy could reduce to time required for the swollen SMGs to regress.
Our data on low serum complement component in the regressed SMG group implied that serum complement level could be a biomarker to predict spontaneous regression of swollen SMGs in IgG4-related disease. Despite the small sample number in this study, receiver operating characteristic curve on spontaneous regression and serum complement level showed high area under the curve, sensitivity, specificity, positive predictive value, and negative predictive value for the cut-off value of 57 U/mL (0.913, 93.3%, 80.0%, 93.3%, and 80.0%, respectively, data not shown).
It is unclear how low complement levels might affect the evolution of IgG4-related disease.18,19 It has been reported that complement system is activated in some patients with IgG4-related disease.20,21 Immune complexes comprising complement components have been found in specimens from organs affected by IgG4-related disease.22–24 Furthermore, serum IgG4 from some IgG4-related disease patients has been shown to bind to C1q in vitro. 20 Taken together, it is thought that the low complement levels seen in this study reflect the activation and consumption of the complement components. We also found that serum complement levels recovered along with the spontaneous regression of SMG swelling, which corresponds well with previous reports that low complement levels reflect IgG4-related disease activity.19,21,25
In this study, some patients with IgG4-related disease had low complement levels, whereas others did not, as reported in different studies.19,25 We also compared clinical data between the patients with low and normal complement levels, but there were no significant differences in age, sex, serum IgG, serum IgG4, or follow-up period (data not shown). It is unknown why complement system is activated and consumed only in some patients with IgG4-related disease. In vitro study showed that serum IgG4 from IgG4-related disease patients with low complement levels has been shown to bind to C1q, while IgG4 from those with normal complement levels did not. 20 The affinity of IgG4 to C1q might be a reason for variety of serum complement level in IgG4-related disease. Further studies are needed to clarify the role of complement system and immune complex formation in the pathophysiology of SMG swelling and its spontaneous regression in the context of IgG4-related disease.
Conclusion
The majority of swollen SMGs in patients with IgG4-related disease spontaneously regressed without steroid therapy, although steroid therapy reduced the time required for the swollen SMGs to regress. Furthermore, we found low serum complement levels in the patients with regressed SMGs. The low serum complement levels could be used as a biomarker for predicting the spontaneous regression of swollen SMGs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by our institutional review board.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by JSPS KAKENHI Grant (Numbers 17H06491 and 18K16871), the Akiyama Life Science Foundation Grant, and GSK Japan Research Grant 2015 to M. S.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.