
Abstract
Background
Dementia is widely recognized as a factor that influences the outcomes of total knee arthroplasty (TKA). However, recent studies have not fully elucidated the effects of dementia on perioperative medical and surgical complications, as well as in-hospital resource utilization. The objective of this study is to evaluate the specific impact of dementia on perioperative outcomes in elderly patients undergoing TKA.
Methods
Data on elderly patients undergoing TKA were extracted from the National Inpatient Sample database (2010-2019). Patients were categorized into a dementia group and a non-dementia group. Propensity score matching (PSM) was employed to control for differences in demographics, hospital characteristics, and comorbidities. Multivariate logistic regressions were conducted to evaluate perioperative outcomes.
Results
From 2010 to 2019, a group of 344,200 patients undergoing TKA was identified, among whom 6761 individuals (2.0%) were diagnosed with dementia. Following PSM, dementia remained an independent predictor for several perioperative outcomes, including urinary tract infection (aOR = 2.001, 95%CI = 1.561-2.564, P < 0.0001), pneumonia (aOR = 2.043, 95%CI = 1.244-3.355, P = 0.005), postoperative delirium (aOR = 5.854, 95%CI = 4.418-7.758, P < 0.0001), acute hemorrhagic anemia (aOR = 1.229, 95%CI = 1.128-1.340, P < 0.0001), prolonged hospital stay (aOR = 1.966, 95%CI = 1.785-2.165, P < 0.0001), and increased total healthcare charges (aOR = 1.122, 95%CI = 1.037-1.215, P = 0.004).
Conclusion
Dementia is independently associated with an increased risk of perioperative complications after TKA, underscoring the importance of tailored perioperative care for elderly patients with dementia.
Keywords
Background
Total knee arthroplasty (TKA) is widely recognized as an effective intervention for end-stage knee osteoarthritis (KOA), 1 a degenerative disorder closely associated with advanced age. 2 As the population ages, the prevalence of KOA is expected to rise, leading to an increased demand for TKA. 3 A previous study indicated that the demand for TKA in the United States is anticipated to surge by 673%, reaching approximately 3.48 millions procedures between 2005 and 2030. 4 Despite high implant survival rates of 95-97% over 20 years, 5 medications and comorbidities can significantly impact surgical outcomes and elevate the risk of complications,6,7 highlighting the importance of identifying modifiable and non-modifiable risk factors.
A previous study showed that both osteoarthritis (OA) and dementia are conditions associated with aging, and there exists a correlation between OA and dementia. 8 Dementia is a syndrome of acquired cognitive impairment, characterized by progressive decline in memory, language, and orientation, which impairs independent living and daily functioning.9,10 The global population of individuals with dementia will rise from 57.4 millions in 2019 to 152.8 millions in 2050 due to population growth and aging. 11 Among those over 65 years, dementia prevalence is estimated at 7%, with higher rates observed in developed countries, reflecting longer life expectancies. 10
In one study, patients with dementia experienced significant pain relief following joint replacement. 12 However, dementia was shown to be a risk factor for certain postoperative complications and increased mortality after surgical procedures.13-17
In recent years, there has been a scarcity of large-scale studies examining whether elderly patients with dementia undergoing TKA face higher risks of medical and surgical complications, as well as increased in-hospital resource utilization. We hypothesized that dementia would increase the incidence of specific perioperative complications, prolong length of stay (LOS), and raise total charge (TOTCHG) in this population. Accordingly, we analyzed data from the National Inpatient Sample (NIS) database for the first time, comparing perioperative complications and in-hospital resource utilization between patients with and without dementia.
Methods and Materials
We used the STROBE cross-sectional checklist when writing our report. 18
Study Design
This retrospective study was based on the NIS database and included patients over 65 years old who underwent TKA surgery for primary KOA between 2010 and 2019. According to whether they were diagnosed with dementia, eligible patients were stratified into a dementia group and a non-dementia group.
Data Source
Study data were obtained from the 2010-2019 NIS database, which is component of databases and software tools developed for the Healthcare Cost and Utilization Project (HCUP). As the largest publicly available, fully paid inpatient health care database in the United States, it contains 20.00% of all discharges in the United States, with approximately 8 millions acute admissions annually from 47 states and the District of Columbia. 19 The database collects diagnoses and procedures coded according to the International Classification of Diseases, Ninth Revision (ICD-9) and 10th Revision (ICD-10), along with patients’ demographics, hospital characteristics, primary expected payer, LOS and TOTCHG. 19
Study Cohort
Patients undergoing TKA were identified based on the principal procedure (PR1) using procedure codes from the International Classification of Diseases, Ninth Revision, Procedure Coding System (ICD-9-PCS: 81.54) and 10th Revision, Procedure Coding System (ICD-10-PCS: 0SRC, 0SRD). 20 Patients undergoing primary unilateral or bilateral TKA were eligible for inclusion. Patients were excluded if they had non-primary KOA (eg, secondary osteoarthritis or neoplasm of long bones of lower limb), were under 65 years old, had non-elective admissions, or had missing data for key variables (age, gender, insurance type, admission type, hospital bed size, teaching status, location, region, LOS, TOTCHG, or in-hospital mortality). To minimize confounding bias, 1:1 propensity score matching (PSM) was conducted. After matching, patients were categorized into a matched dementia group and a matched non-dementia group.
Baseline Data
Variables Used in Logistic Regression Analysis and Propensity Score Matching

Outcomes
In this study, perioperative complications were selected as the primary outcomes, while LOS, TOTCHG, and in-hospital mortality were defined as secondary outcomes. The term “perioperative” was defined to encompass the duration from patient admission to discharge. Perioperative complications were identified using ICD-9 and ICD-10 codes (Table S1). Medical complications included acute renal failure, urinary tract infection, acute myocardial infarction, acute heart failure, deep vein thrombosis, pulmonary embolism, septicemia, postoperative shock, blood transfusion, thrombocytopenia, respiratory failure, pneumonia, postoperative delirium, acute hemorrhagic anemia and hemorrhage/seroma/hematoma. Surgical complications included surgical site infection, wound dehiscence, fracture and revision surgery. In-hospital resource utilization was assessed using LOS and TOTCHG, with values above the 75th percentile defined as prolonged LOS and higher TOTCHG.
Statistical Analysis
Continuous variables were compared using the unpaired t-test, and categorical variables using the Chi-square test. Multivariate logistic regressions were employed to assess the association between dementia and perioperative outcomes, with 95% confidence intervals (95%CI), unadjusted odds ratios (uOR), and adjusted odds ratios (aOR) reported. For the matched groups, two logistic regression models were constructed: Model 1 included dementia and propensity score provided by PSM, while Model 2 was adjusted for dementia, all patients’ demographics, 30 comorbidities, and the number of comorbidities (Table 1). Further, the Hosmer-Lemeshow test was employed to evaluate model goodness-of-fit. All tests were considered statistically significant at P < 0.05. All statistical analyses were conducted using IBM SPSS Statistics version 26.
1:1 PSM was conducted to align demographics, hospital characteristics, all pre-existing comorbidities and the number of comorbidities in both dementia and non-dementia groups (Table 1). The caliper value was set at 0.01. Standardized mean differences (SMD) for all variables were <0.10 after PSM, indicating satisfactory balance between the matched dementia and matched non-dementia groups.
Results
Study Cohort
Between 2010 and 2019, a total of 1 339 936 patients underwent TKA. After applying the eligibility criteria and performing PSM, the final analysis comprised 6726 matched patients with dementia and 6726 matched patients without dementia (Figure 1). Procedures for cohort inclusion and exclusion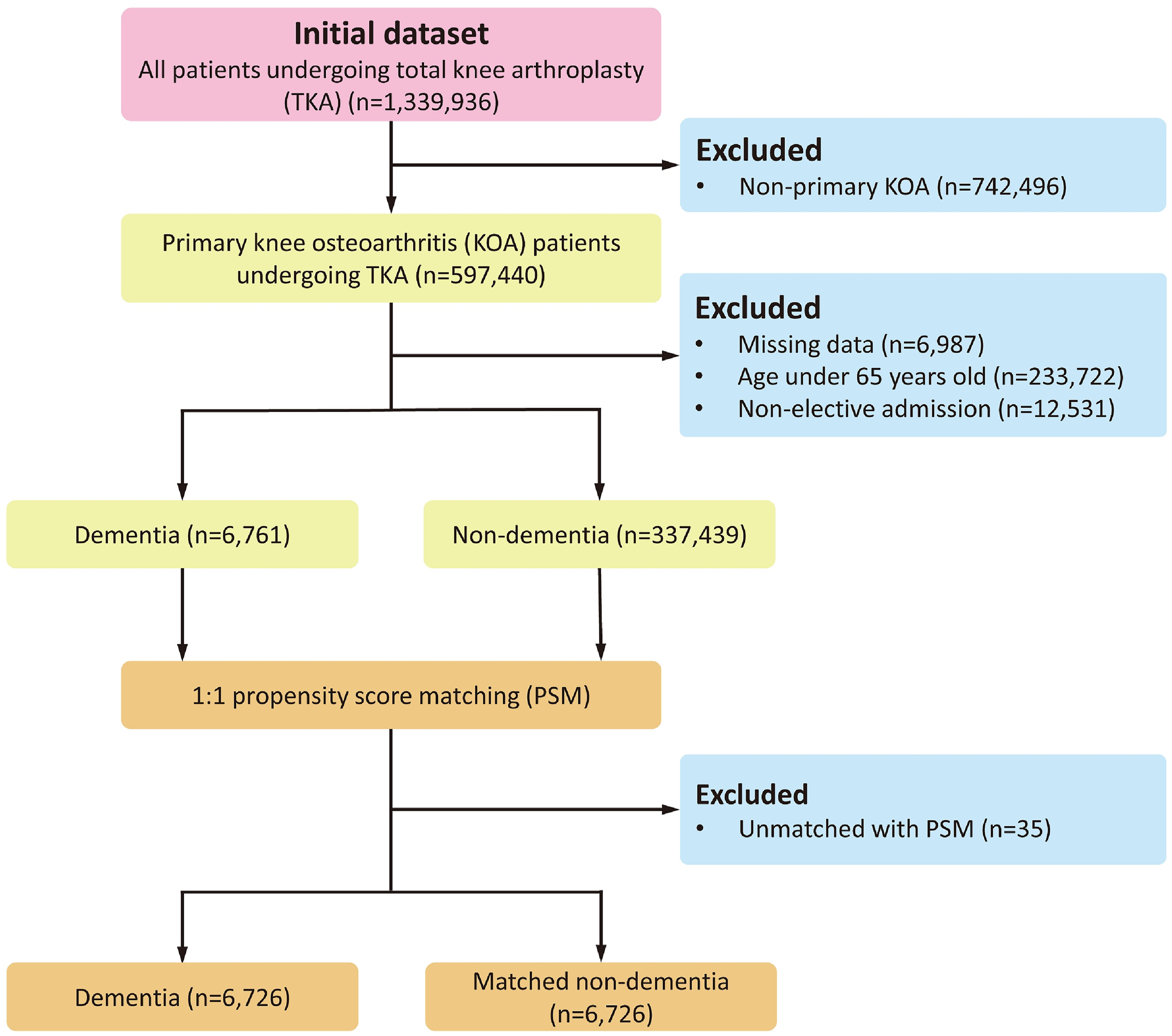
Occurrence of Dementia in Elderly Patients Undergoing TKA
Finally, a total of 344 200 patients who underwent TKA were retrieved from the NIS database between 2010 and 2019. Overall, there were 6761 cases of dementia, resulting in an overall prevalence rate of 2.0% (6,761/344,200) (Figure 2). Importantly, our findings found a significant increase in the annual incidence of dementia among elderly inpatients undergoing TKA, particularly after 2011 (Figure 2). Annual incidences of dementia in patients undergoing total knee arthroplasty
Patients’ Demographics, Hospital Characteristics, and Comorbidities
Patients’ Demographics and Hospital Characteristics
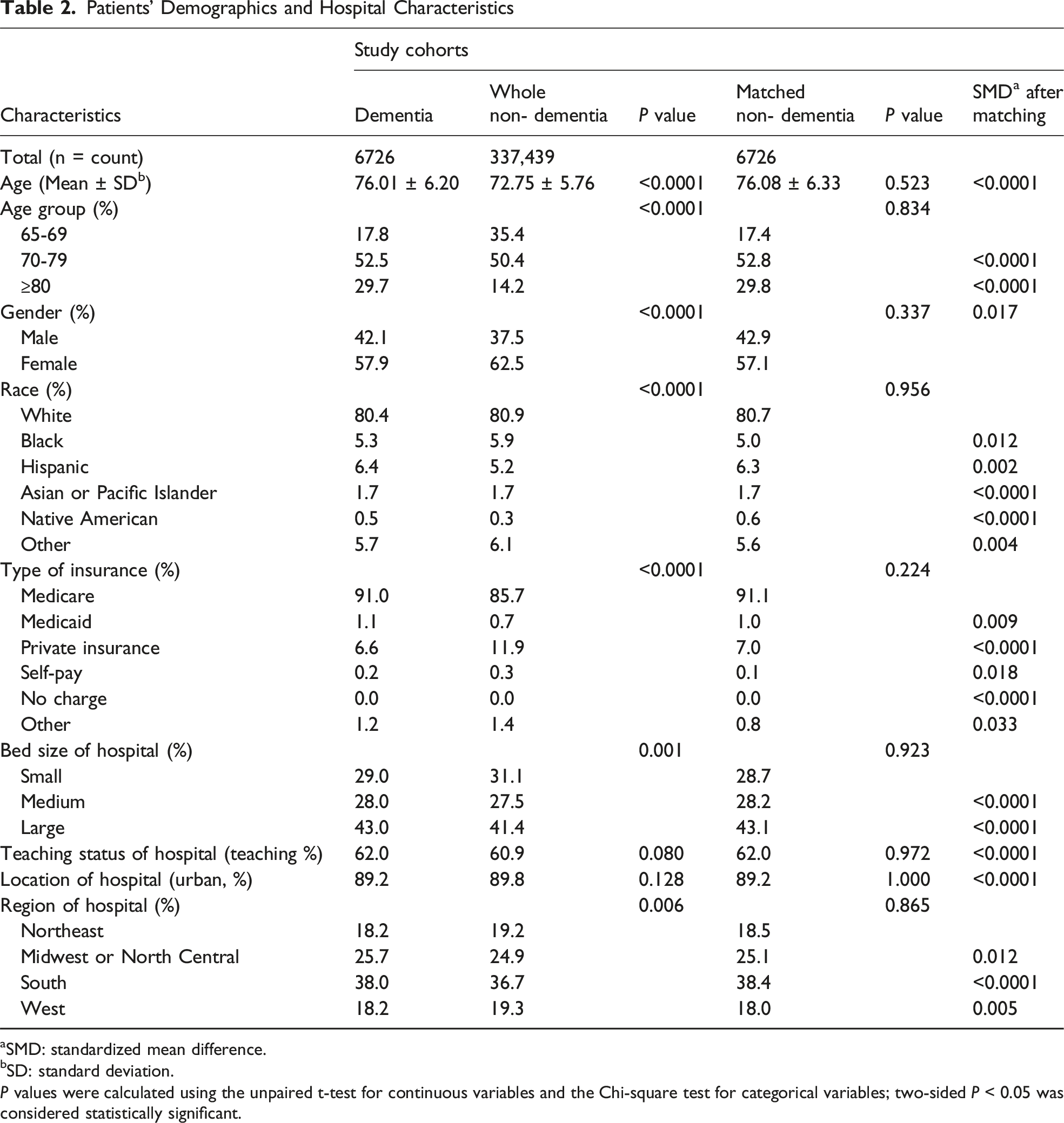
aSMD: standardized mean difference.
bSD: standard deviation.
P values were calculated using the unpaired t-test for continuous variables and the Chi-square test for categorical variables; two-sided P < 0.05 was considered statistically significant.
Several hospital characteristics also differed significantly between the groups. Most patients were covered by Medicare, with Medicare and Medicaid more prevalent among dementia patients (P < 0.0001). Dementia patients were more frequently treated in hospitals with larger bed sizes (P = 0.001) and were more often hospitalized in the Midwest or North Central and Southern regions (P = 0.006) (Table 2).
Patients’ Pre-existing Comorbidities

aSMD: standardized mean difference.
P values were calculated using the Chi-square test; two-sided P < 0.05 was considered statistically significant.
After 1:1 PSM, all baseline differences, including demographics, hospital characteristics, and comorbidities, were eliminated, resulting in two well-balanced matched groups (SMD <0.1) (Tables 2 and 3).
Perioperative Complications
Perioperative Complications of Total Knee Arthroplasty

P values were calculated using the Chi-square test; two-sided P < 0.05 was considered statistically significant.
In the logistic regression analysis of the unmatched groups, dementia was associated with a higher risk of several perioperative complications, whereas most other complications did not differ significantly from the non-dementia group (Figure 3). Unadjusted odds ratios of perioperative outcomes for the dementia and the whole non-dementia groups. uOR: unadjusted odds ratio, 95%CI: 95% confidence interval, LOS: length of stay, TOTCHG: total charge. uOR (squares) with 95%CI (horizontal lines) were estimated by multivariable logistic regression; two-sided P < 0.05 indicates significance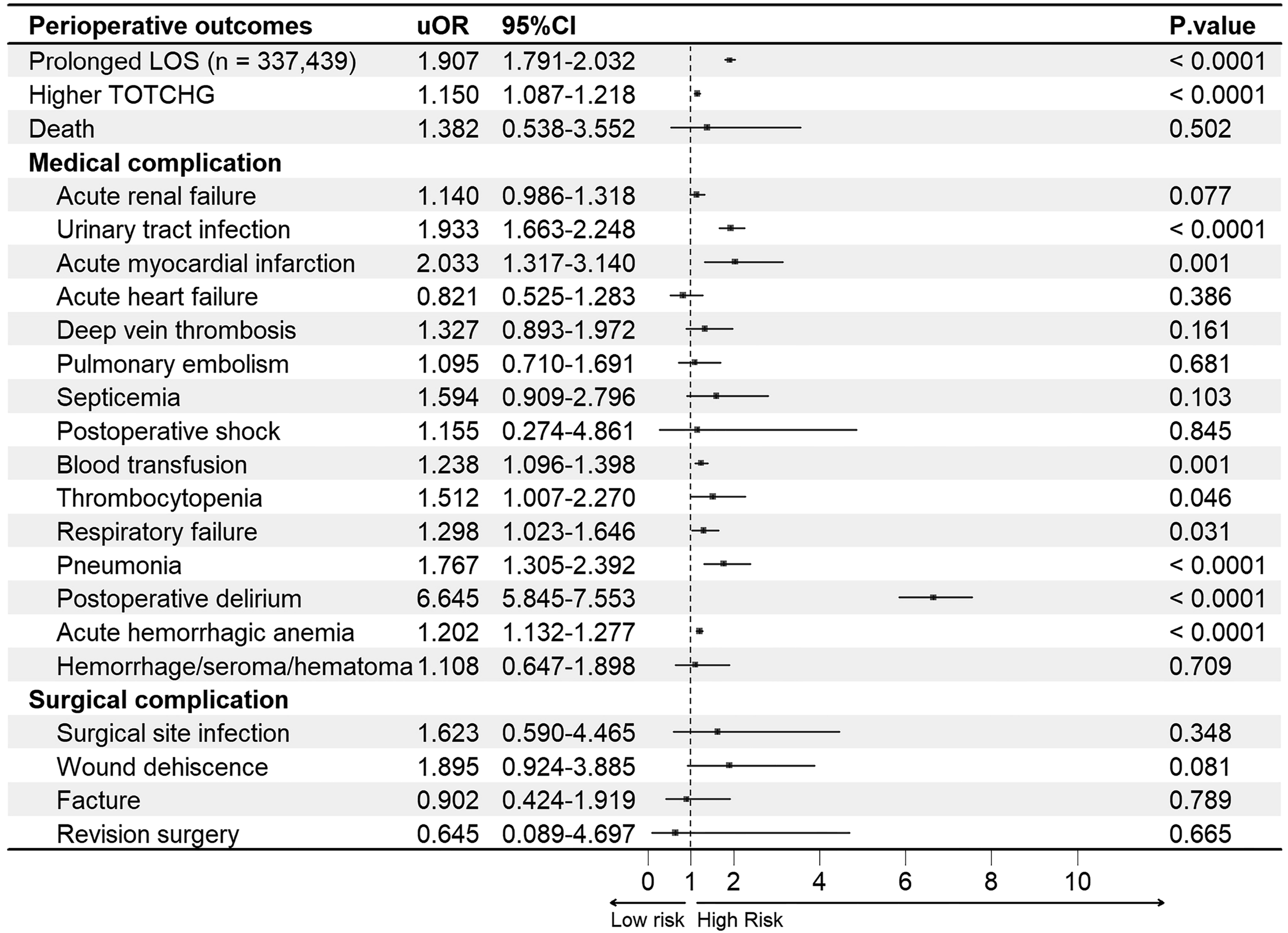
Model 1 logistic regression analysis after PSM revealed dementia statistically significantly increased the risk of urinary tract infection (aOR = 1.959, 95%CI = 1.533-2.504, P < 0.0001), pneumonia (aOR = 1.888, 95%CI = 1.160-3.071, P = 0.010), postoperative delirium (aOR = 5.698, 95%CI = 4.306-7.541, P < 0.0001), and acute hemorrhagic anemia (aOR = 1.218, 95%CI = 1.119-1.326, P < 0.0001) (Figure 4). Model diagnostics showed adequate fit for some outcomes (P > 0.05), but suboptimal fit was observed for pneumonia (P = 0.047), postoperative delirium (P = 0.007), and acute hemorrhagic anemia (P < 0.0001) (Table S2). Adjusted odds ratios of perioperative outcomes for the dementia and the matched non-dementia groups (Model 1). aOR: adjusted odds ratio, 95%CI: 95% confidence interval, LOS: length of stay, TOTCHG: total charge. aOR (squares) with 95%CI (horizontal lines) were estimated by multivariable logistic regression; two-sided P < 0.05 indicates significance
After further adjustment for patient demographics and comorbidities, the associations observed in Model 1 remained consistent. Dementia was a statistically significantly risk factor for urinary tract infection (aOR = 2.001, 95%CI = 1.561-2.564, P < 0.0001), pneumonia (aOR = 2.043, 95%CI = 1.244-3.355, P = 0.005), postoperative delirium (aOR = 5.854, 95%CI = 4.418-7.758, P < 0.0001), and acute hemorrhagic anemia (aOR = 1.229, 95%CI = 1.128-1.340, P < 0.0001) (Figure 5). Model diagnostics indicated improved goodness-of-fit compared with Model 1 (P > 0.05) (Table S2). Adjusted odds ratios of perioperative outcomes for the dementia and the matched non-dementia groups (Model 2). aOR: adjusted odds ratio, 95%CI: 95% confidence interval, LOS: length of stay, TOTCHG: total charge. aOR (squares) with 95%CI (horizontal lines) were estimated by multivariable logistic regression; two-sided P < 0.05 indicates significance
In-Hospital Resource Utilization
In-Hospital Resource Utilization of Total Knee Arthroplasty

aLOS: length of stay.
bTOTCHG: total charge.
cSD: standard deviation.
P values were calculated using the unpaired t-test for continuous variables and the Chi-square test for categorical variables; two-sided P < 0.05 was considered statistically significant.
In the analysis of the unmatched groups, dementia was associated with prolonged LOS and higher TOTCHG (Figure 3). Model 1 showed similar associations (LOS: aOR = 1.890, 95%CI = 1.721-2.076, P < 0.0001; TOTCHG: aOR = 1.115, 95%CI = 1.031-1.206, P = 0.006) (Figure 4). After adjusting for covariates, Model 2 confirmed these findings (LOS: aOR = 1.966, 95%CI = 1.785-2.165, P < 0.0001; TOTCHG: aOR = 1.122, 95%CI = 1.037-1.215, P = 0.004) (Figure 5) and demonstrated good model fit, supporting the robustness of the results.
Discussion
This study conducted a large-scale analysis of elderly patients with dementia undergoing TKA, focusing on health economic aspects. This study is the first in recent years to examine the outcomes of TKA in elderly patients with dementia from various aspects utilizing the NIS database. In this study, we observed that dementia was independently associated with an increased risk of various perioperative complications and greater utilization of healthcare resources. Our research encompasses a wide range and diverse set of patient information; thus, our findings may still be informative for other similar healthcare settings.
According to our research, between 2010 and 2019, the incidence of dementia ranged from 1.3% to 2.3%, with a slight increase after 2011, likely related to the NIA-AA diagnostic criteria. 21 Additionally, although the transition from ICD-9 to ICD-10 in 2015 introduced additional codes, 22 the annual incidence remained stable, suggesting that diagnostic or coding changes are unlikely to have influenced our findings.
Adjusted multivariate analysis of both models after PSM revealed that dementia significantly increased the risk of urinary tract infection and pneumonia after TKA. Bail K et al compared dementia and non-dementia inpatients and demonstrated that dementia patients had higher rates of urinary tract infections and pneumonia. 23 Wu YM et al found that the rate of pneumonia and urinary tract infection was significantly increased in dementia patients following major surgery. 24 Clinically, urinary incontinence and low bladder function may predispose patients to catheter-related urinary tract infections, 25 while swallowing dysfunction increases the risk of aspiration pneumonia.26,27 Awareness of these vulnerabilities allows clinicians to implement targeted preventive measures, such as minimizing catheter use and duration, and early assessment and management of swallowing difficulties.26,28
Our study identified dementia as a significant risk factor for postoperative delirium, consistent with findings from previous research. For example, Lih Wang et al reported that among patients undergoing TKA, a history of dementia was a risk factor linked with postoperative delirium. 29 Likewise, Kyu Sung Chung et al showed that a history of dementia was identified as a significant independent risk factor and the strongest independent predictor of delirium. 30 Dementia likely increases brain vulnerability, making patients more susceptible to delirium when exposed to surgical stress and other predisposing factors, potentially through systemic inflammation, neuroinflammation, and neuronal damage. 9 Further research is warranted to clarify the underlying mechanisms and to develop effective strategies for preventing postoperative delirium.
In our study, even after eliminating differences in coagulopathy, deficiency anemia, and chronic blood loss anemia among groups through PSM, dementia still showed a statistically significant correlation with acute hemorrhagic anemia. Previous studies have reported that several dementia subtypes, including Alzheimer’s disease, vascular dementia, Parkinson’s disease dementia, and Lewy body dementia, are associated with thrombocytopenia and platelet functional impairment.31-35 Collectively, these alterations may compromise hemostasis and increase susceptibility to perioperative bleeding in the setting of total joint arthroplasty.36-38 Although evidence is limited, dementia-related platelet dysfunction may contribute to acute hemorrhagic anemia, highlighting the need for greater perioperative awareness and further research.
Several of our findings are consistent with studies conducted in other surgical populations. Studies in total hip arthroplasty, hip fracture, and spinal surgeries have shown that dementia increases the risks of postoperative pneumonia, urinary tract infection, and delirium.39-42 Notably, evidence from cardiovascular surgery further supports these results, demonstrating that patients with dementia are at an elevated risk for postoperative pneumonia and delirium. 43 These parallels strengthen the generalizability of our findings and emphasize the need for tailored perioperative strategies across different surgical fields, beyond TKA.
In this study, dementia was independently associated with longer hospital stays and higher healthcare costs. This finding aligns with earlier research showing that patients with dementia often experience prolonged hospitalization following TKA. 44 Additionally, prior studies have demonstrated that postoperative complications prolong hospital stays, increase resource utilization, and elevate costs.45,46 Our results similarly indicate that patients with dementia tend to have more comorbidities and are more prone to complications, which likely contribute to extended hospitalization and greater overall costs.
Limitations
This study has several limitations. First, it did not distinguish between dementia subtypes or perform subgroup analyses to assess their differential impact on perioperative outcomes of TKA. Future studies should incorporate subtype-specific analyses to facilitate more tailored preventive strategies for perioperative complications in patients with various forms of dementia.
Second, the NIS database lacks detailed data on certain assessments of preoperative health conditions and laboratory parameters such as the preoperative functional status and serum albumin, as well as post-discharge health status and long-term outcomes. Therefore, our analysis may have overlooked some potential confounding factors and could not include long-term postoperative outcomes such as chronic pain, long-term survival, or readmission rates. Previous studies have reported higher readmission and mortality rates among patients with dementia after TKA.13,47 To more fully elucidate the impact of dementia on TKA outcomes, particularly over the long term, a more detailed evaluation of patients’ perioperative health status is needed, and prospective longitudinal studies with extended follow-up are warranted.
Third, our results rely on the accuracy and completeness of International Classification of Diseases (ICD) coding. Dementia and TKA may be underdiagnosed or misclassified, as ICD codes may not fully capture all cases or may be subject to coding errors. Such misclassification could potentially lead to underestimation or overestimation of the true association between dementia and perioperative complications.
Conclusion
As dementia becomes more prevalent and the demand for TKA continues to rise, understanding its impact on perioperative outcomes is increasingly critical. Using the NIS database, this study demonstrates that dementia in elderly TKA patients is significantly associated with higher perioperative complications and increased healthcare resource utilization. These findings highlight the need for tailored perioperative care to improve surgical safety in elderly patients with dementia.
Supplemental Material
Supplemental Material - Impact of Dementia on Perioperative Complications in Elderly People Undergoing Total Knee Arthroplasty: A Retrospective National Inpatient Sample Database Study
Supplemenral Material for Impact of Dementia on Perioperative Complications in Elderly People Undergoing Total Knee Arthroplasty: A Retrospective National Inpatient Sample Database Study by Yusong Zhang, Linjia Li, Yuanwei Wu, Jian Wang, Yuxin Zhong, Qinfeng Yang, and Jiwei Luo in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Ethical Considerations
Not applicable. This article does not contain any studies conducted by any of the authors on human participants or animals. Additionally, this observational study was granted exempt status by the institutional review board because of its use of deidentified publicly available data. Therefore, there is no need to grant permission in the ethical approval and consent to participate sections. All methods were carried out following relevant guidelines and regulations.
Consent for Publication
All participants involved in this study have provided informed consent for the publication of the findings, including any personal data, images, or videos that may be included in the manuscript.
Author Contributions
All authors contributed to the thinking and design of the study. Yusong Zhang, Linjia Li, and Yuanwei Wu contributed equally to this work. Material preparation, data collection, and analysis were performed by Yusong Zhang, Linjia Li, and Yuanwei Wu. The first draft of the manuscript was written by Yusong Zhang and Linjia Li, with revisions, guidance, and feedback by Jian Wang, Yuxin Zhong, Qinfeng Yang, and Jiwei Luo. All authors commented on earlier versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.