
Abstract
Introduction
Lower-limb osteoarthritis (OA) in the elderly can be a risk factor for frailty, which is the preliminary of disability, but it may be reversible with appropriate interventions. We aimed to use the Kihon Check List (KCL) to assess multiple domains of frailty and to identify the characteristics of frailty in patients with hip or knee OA following total joint arthroplasty.
Materials and Methods
This study included 136 ≥ 65-year-old patients (mean age: 73.0 years) who underwent total arthroplasty with end-stage hip and knee OA. We assessed frailty status, instrumental activities of daily living (IADL), and health-related quality of life (HRQoL) according to the KCL, functional ambulatory index (FAI) and EuroQol-5 Dimension (EQ5D), respectively, as well as the extent of pain preoperatively and at postoperative 6 months.
Results
Using KCL, seventy-eight (57.4%) patients were frail preoperatively, but the prevalence significantly decreased to 52 patients (38.2%) at postoperative 6 months. Total arthroplasty intervention provided significant improvements in the total KCL scores, including the physical domain (P < .01), pain (P < .01), FAI scores (P < .01), and EQ5D (P < .01), but not the social domain. Multivariate logistic regression analysis identified age at surgery (OR: .93, 95% CI: .86-.99) and preoperative FAI score (OR: 1.10, 95% CI: 1.03-1.19) as independent predictors of postoperative frailty.
Conclusions
Total arthroplasty procedures on patients with hip and knee OA reduced their KCL score, but social aspects were less improved than physical aspects in the shortterm. Older age and preoperative lower IADL score can be useful for accurately estimating less improvement of frailty in the early postoperative phase. Our results suggest that long term follow-up of OA is needed to provide comprehensive interventions, including in social aspects, especially for patients with lower activity.
Introduction
In the last 50 years, several lifestyle factors have improved human life span, which has led to an increase in age-related diseases 1 and frailty. 2 Frailty, caused by a multisystemic reduction in the reserve capacity, 3 is the preliminary stage of disability. 4 However, it may be reversible with appropriate interventions. 5 Osteoarthritis (OA) is thought to be the most prevalent chronic joint disease and one of the most common sources of pain and disability in the elderly: consequently, OA may lead to frailty and the need for nursing care of an individual. 6 Thus far, no cure for OA has been found; instead when pain relief is no longer sufficient, the final treatment option is total joint arthroplasty of the hip (total hip arthroplasty [THA]) or knee (total knee arthroplasty [TKA]). 7 Surgery and its postoperative rehabilitation are causally linked to the improvement of pain and the recovery of physical function. On the other hand, OA is associated with increased mortality, increased length of stay in hospital, higher chance of readmission, and higher rates of discharge to institutional care after THA and TKA in frail patients than in non-frail patients with OA. 8 Although some studies have stated that THA and TKA improved functional mobility of OA patients, 9 few have discussed frailty after arthroplasty surgery for patients with end-stage hip or knee OA.
The concept of frailty includes physical, psychological, and social components, which influence each other. Among them, social frailty has attracted recent attention. 10 Presently, several frailty scales are used, and a lot of empirical research has been conducted to determine which frailty scale is best suited for clinical applications. 11 From several aspects, frailty is clinically considered to be a predisability, and elderly functioning should be assessed across multiple domains to identify frail individuals. 12 The Kihon Check List (KCL) is a reliable tool for screening frailty status that was developed to identify older people at risk of dependency. 13 The KCL is thought to be a type of deficit model, similar to the frailty index, 14 because its score reflects the number of functional declines in each domain. This categorical structure is helpful for identifying problematic domains for prevention and indicating frailty status. In addition, the total KCL score has been found to significantly correlate with the number of frailty phenotypes defined in the Cardiovascular Health Study frailty index criteria.15,16 The KCL also includes factors related to psychological and social aspects, enabling a more comprehensive frailty evaluation. Few studies have used KCL to evaluate frailty,17,18 and this assessment tool is not yet used as a frailty scale in studies on musculoskeletal diseases. Hence, the predictive power and usefulness of KCL have not been confirmed in patients with OA after arthroplasty.
The study aim was to evaluate the prevalence of frailty in patients who were scheduled to undergo THA and TKA and to use the KCL to identify the characteristics of each frailty domain over the shortterm postoperative period. We also aimed to identify preoperative factors predictive of persistent postoperative frailty.
Materials and Methods
Patients
This was a longitudinal prospective cohort study in patients who intended to undergo primary THA or TKA at a single acute care hospital from April 2019 to March 2021. The inclusion criteria were patients with hip and knee osteoarthritis, ≥ 65 years old and who were scheduled to undergo primary unilateral total arthroplasty and were able to complete some questionnaires. Eligible patients were informed about the study through written and oral communication from the researcher before surgery. Patients who agreed to be approached by the researcher received written information about the study, some questionnaires, and a consent form. In our hospital, operations were performed using the same surgical procedures for each joint, and clinical paths were followed for perioperative management and standardized rehabilitation until discharge to home or a post-acute institute. Full-weight bearing was allowed immediately after surgery. We provided instructions on a self-exercise program for patients discharged to home, including range of motion of the operated joint, muscle resistance training, walking, balance training and basic ADL, and the patients were examined at regular intervals in the outpatient department. The patients discharged to a post-acute hospital were trained in a similar program under the guidance of a physiotherapist. Patients were evaluated for their outcomes preoperatively and at 6 months after THA and TKA. The study exclusion criteria were as follows: patients who have hip or knee OA in opposite side or other joint, revision THA or TKA, inflammatory diseases, such as rheumatoid arthritis or systemic lupus erythematosus, and development of severe postoperative complications or adverse events, including infection, periprosthetic fractures, and dislocation of total hip joint.
Of the 168 eligible patients (115 with THA and 53 with TKA), 12 (4 with THA and 8 with TKA) had an insufficient response to the questionnaires and 13 (7 with THA and 6 with TKA) were lost to follow-up at 6 months. Additionally, we excluded 4 patients with infection (3 with THA and 1 with TKA), 2 patients with periprosthetic fractures (TKA), and 1 patient with dislocation (THA); thus, a total of 136 patients (100 with THA, 36 with TKA) were enrolled in this study.
Outcome Measures
The study reviewed the medical records to obtain patient age, sex, Body Mass Index (BMI), Charlson Comorbidity Index (CCI). 19 By questionnaires, we evaluated frailty, the extent of pain, Instrumental Activities of Daily Living (IADL), and Health-related quality of life (HRQoL) for patients after THA and TKA. Based on previous reports that patients' motor function following THA and TKA significantly improved within postoperative 6 months, we measured clinical outcomes preoperatively and at 6 months postoperatively.20,21
Frailty: KCL
Participants were assessed preoperatively and at postoperative 6 months for frailty using the KCL, which is a good candidate screening tool for identifying frailty in the primary care setting or in outpatient clinics to promote public health.22,23 This assessment tool is a simple self-reporting yes/no survey consisting of 25 questions (Figure 1) focused on the daily routine of older individuals, and it is distinguished from other frailty assessment tools directly addressing the disease.
22
The following terminology was used: questions 6-10 as “physical domain,” questions 4-5 and 16-17 as “social domain,” and questions 1-25 as “total KCL score.” In addition to these, KCL has “IADL,” “nutrition,” “eating,” “memory,” and “mood” domains. Difficulty with any question was counted as a score in the KCL, with a higher score in each domain of the checklist indicating a higher risk of requiring support or care in that domain, so together the survey questions could give a total score between 0 and 25. The patients were divided into two groups: the non-frailty group (KCL scores < 7) and the frailty group (KCL scores ≥ 7) based on a previous report.
23
Kihon Check List.
Pain: Visual Analogue Scale (VAS)
Pain at walking was ranked from 0 to 10 according to the VAS preoperatively and at the 6 months follow-up period.
IADL: Frenchay Activities Index (FAI)
We used the FAI, which has undergone expensive evaluation, to assess IADL. 24 The 15 items of the FAI cover a variety of complex activities, and the FAI consists of a single summary score from 0 points for a sedentary lifestyle to 45 points for a very active lifestyle. The item scoring is based on the frequency with which the activity is performed.
HRQoL: EuroQol-5 Dimension-5 Level (EQ5D-5L) Questionnaire
HRQoL was measured by the EuroQol-5 dimension, which consists of a five-dimensional classification system.25,26 EQ5D-5L has five dimensions: mobility, self-care, daily activities, pain/discomfort, and anxiety/depression. Each dimension has five levels: no difficulty, a little difficulty, moderate difficulty, serious difficulty, and very serious difficulty. The full score of the scale is 1.00 point, and higher scores indicate better health.
Statistical Analysis
Descriptive data are presented as the mean plus standard deviation or number and percentage. The significance of differences between two groups was statistically analyzed using an unpaired t-test for continuous parametric data and a Chi-square test for categorical variables. Age, sex and preoperative variables with a P value of < .05 in the univariate analysis were used in the logistic regression model. Multiple logistic regression analysis was used to determine clinical outcomes independently associated with frailty status in patients after lower-limb arthroplasty. The results are presented as the odds ratio (OR) with 95% confidence interval (CI). The area under the curve (AUC) of the receiver operating characteristic (ROC) curve was calculated to assess the diagnostic value and accuracy of different parameters as a predictive factor for differentiating between non-frailty and frailty. Statistical analyses were performed using JMP® version 15.0 (SAS Institute Inc, Cary, NC). A P value of < .05 was considered to be indicative of statistically significance.
Results
Preoperative Participant Characteristics
Preoperative characteristics in the non-frail and frail patient groups.
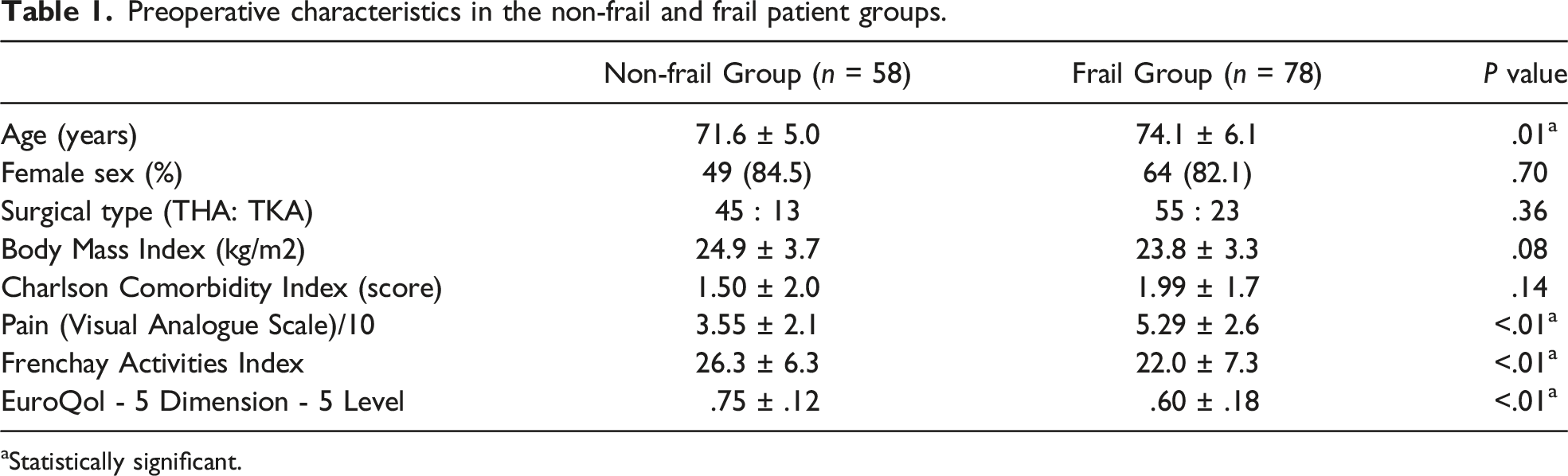
aStatistically significant.
Clinical Outcomes in the Pre- and Postoperative Periods
Outcome measures in pre- and postoperative period.

Pre-op.; Preoperative, Post-op.; Postoperative, KCL; Kihon Check List.
aStatistically significant.

Improvement in the physical and social domains of the Kihon Check List. The KCL Physical domain was significantly improved (P < .01) at 6 months after THA and TKA, but the social domain was not. Pre-op; Preoperative, Post-op; Postoperative, M; Months, SD; Standard deviation.
Clinical Factors Affecting Frailty After THA and TKA
Postoperative characteristics in the non-frail and frail patients’ groups.

aStatistically significant.
Logistic Regression Analysis
Logistic regression analysis for postoperative frailty status.

OR; Odds ratio, CI; confidence interval.
aStatistically significant.
ROC Analysis
We identified the cutoff scores for age and preoperative FAI score using the ROC curve (Figure 3). Our results revealed that age at surgery differentiated recurrent postoperative frailty at a threshold age of 76 years (AUC: .66, 95% CI: .04−.17, P < .01). Furthermore, the preoperative FAI scores differentiated recurrent postoperative frailty at a threshold score of 25 points (AUC: .69, 95% CI: −.17 to −.06, P < .01). Receiver operating characteristic (ROC) curves for age (A) and preoperative FAI (B) score. Arrows indicate the best cutoff values. (A) Age at surgery. Area under the ROC curve: .66 (95% CI: .04−.17); 77.4% sensitivity and 51.9% specificity for a cutoff of 75 years. (B) Preoperative FAI scores. Area under the ROC curve: .69 (95% CI: .06−.17); 52.4% sensitivity and 78.9% specificity for a cutoff of 26 points. AUC; Area under the curve.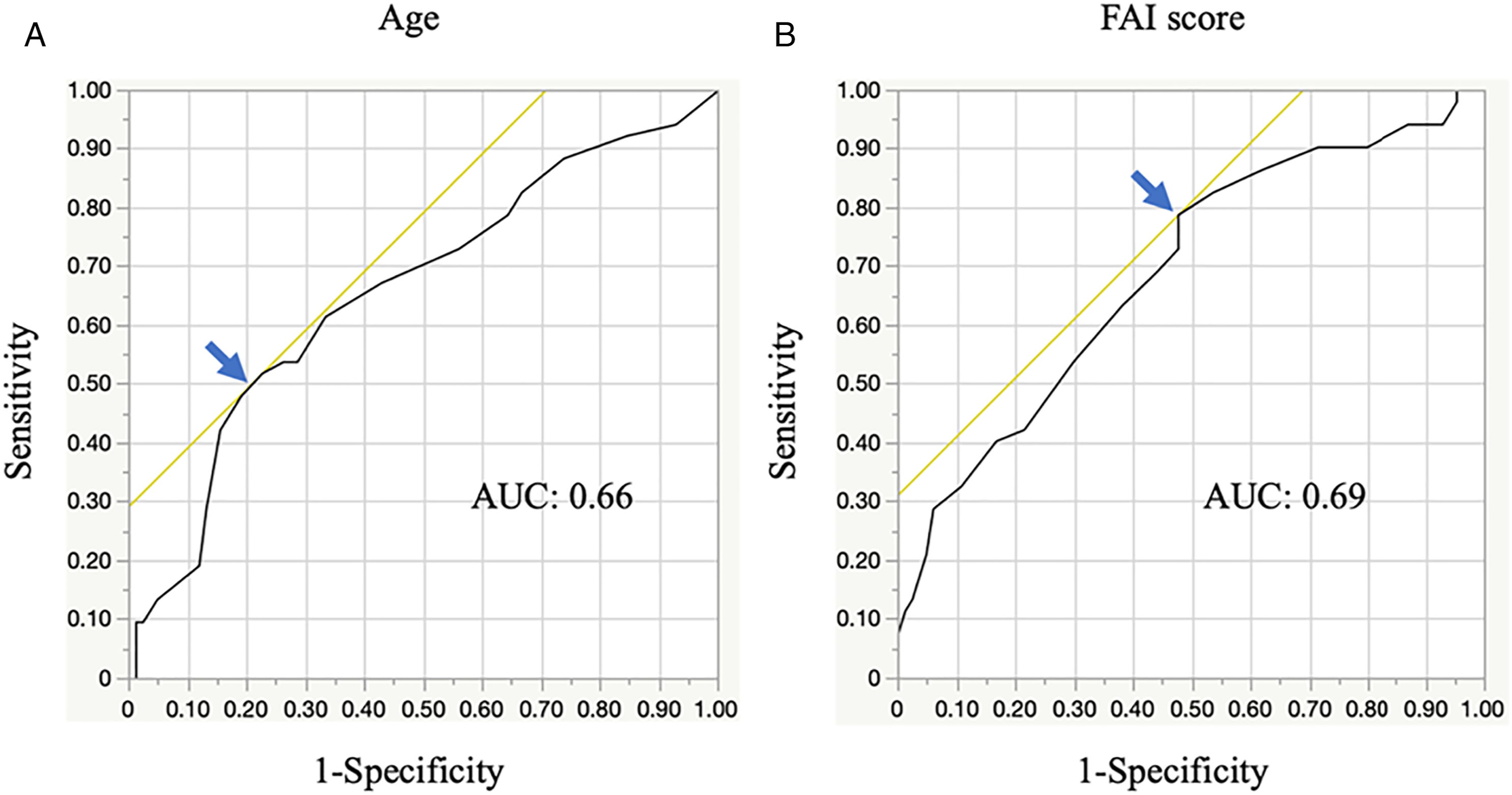
Discussion
The study aim was to identify the prevalence and characteristics of frailty in patients with hip and knee OA requiring surgical treatment and to identify clinical factors associated with frailty using the KCL (cutoff score of 7) following THA and TKA. Our main results showed that the prevalence of frailty in OA patients was decreased by total joint arthroplasty and postoperative rehabilitation, but the persistence of frailty status was observed in 30.1%, and the new appearance was observed in 8.1% at postoperative 6 months. In addition, there was no significant improvement in the social domain of KCL at 6 months after surgery despite improvement in the physical domain. Furthermore, age and the FAI score were independent predictors of frailty at postoperative 6 months. Thus, multidisciplinary interventions, including social aspects, may be necessary over a long period to improve frailty status in low-activity older OA patients.
OA is the most prevalent chronic joint disease in the world and one of the most common causes of pain and disability in the elderly. 27 In addition, OA is strongly associated with the geriatric disease of frailty, which is characterized by reduced homeostatic reserves and resilience and an increased risk of falls and institutionalization. 28 Frailty is a common syndrome in older patients, with an overall prevalence of 7% to 10.7% in people ≥ 65 years old,15,29,30 and there is a significantly higher percentage (range: 24 %–60%) of lower-limb OA in older people. 31 Frailty assessed by the KCL (cutoff score of 7) was observed in 57.4% of patients with hip and knee OA before surgery in our study, which is a relatively high prevalence of frailty. This finding may be explained by the fact that the KCL assessment of frailty is a multidimensional approach that includes not only physical aspects but also psychological and social aspects. In previous research, frail patients with OA had more adverse events in daily activities after THA and TKA; consequently, they had an increased dependence on outside help, and a decrease in IADL and HRQoL.32,33 Reportedlly, total joint arthroplasty for hip and knee OA is highly effective in relieving pain and improving physical function,7,34,35 which is supported by our findings showing significant improvement in pain, IADL, and HRQoL at 6 months after surgery. We also found that frailty in patients was significantly decreased from 57.4 to 38.2% by THA and TKA procedures. On the other hand, persistence of frailty was still relatively common at 6 months postoperatively; thus, we examined which aspects of frailty showed less improvement and which were significantly associated with frailty.
A previous study to clarify the temporal relationship between physical frailty and social frailty found that the association were stronger in the two social domains of social activity and contact with neighbors. 36 In the KCL, social requirements are assessed by questions 4 and 5 and social behaviors by questions 16 and 17, and these were not significantly improved after 6 months postoperatively in our study. Because of the social problems faced by the elderly, social frailty in aging populations is a grave concern, and several studies have shown adverse health effects, such as disability and mortality, attributable to social frailty.36,37 Recent studies have highlighted social frailty as a risk factor for the incidence of physical frailty, disability, and mortality.36,38 In the individual examinations of each aspect of frailty, the physical domain was significantly improved by THA and TKA in the shortterm, but the social domain was not. These results suggest the necessity of follow-up longer than 6 months and additional interventions for social frailty. Social support programs for older people to enhance their quality of life and general well-being have been researched; among participants who completed the program, everyday functioning and health-related quality of life increased, but the greatest improvement was observed in social function. 39 Hence, effective and practical interventions for social frailty have to be investigated and integrated into the nursing care prevention system.
Some researchers have demonstrated a positive relationship between age and frailty. 2 Regarding patients with OA, older age and the presence of frailty are thought to be a risk factor of perioperative complications, longer length of hospital stay, and poor functioning postoperatively.40,41 However, an earlier study demonstrated that the improvement in functional scores was similar for both frail and non-frail patients despite the older median age in the frailty group. The current study found that residual frailty following THA and TKA was significantly associated with older age, 7 but the associations remain controversial. Further studies are needed to assess the effect of age on improving frailty as a prognostic factor in OA patients following THA and TKA.
In patients following lower-limb arthroplasty, the main objective is to ensure that the patient achieves postoperative functional improvement sufficient to perform ADL independently. 42 Basic ADL activities are insufficient to determine independent living in the community 43 and often show a ceiling effect when applied to community residents. 44 Consequently, we chose the IADL to assess the level of participation in more complex activities. The FAI, which assesses a broad range of activities associated with everyday life, was originally developed to evaluate IADL and focuses on issues related to self-care and mobility. In our study, although the FAI score was significantly improved at 6 months after THA and TKA, frail patients have significantly lower FAI scores pre- and postoperatively. In addition, residual frailty postoperatively was associated with lower preoperative FAI scores, suggesting that the baseline FAI score is a better measurement for indicating the expected improvement of frailty. These results can be explained by the fact that this instrument measures activities that reflect a higher level of independence and social participation. Therefore, advanced intervention for frailty focused on social aspect may promote community-based independence of frail patients following THA and TKA.
A population-based prospective cohort study demonstrated that the risk of developing frailty was higher in community-dwelling older adults with OA-related pain than in those without OA-related pain. 45 Additionally, patients with OA pain were also more likely to become frail with the disease progression. 46 Pain is the primary concern of people living with OA and the main reason patients seek medical assistance. Ardoino et al. discussed the importance of managing chronic pain that might become a target for intervention to avoid worsening of frailty in older patients. 47 It was thought to be attributed to the reduction of pain, which is one of goals of THA and TKA surgery, 7 and our study also showed that pain intensity was reduced more in older patients with hip and knee OA for 6 months. Consequently, preoperative pain intensity was not an independent predictor of frailty at 6 months postoperatively. These results suggest that older participants are likely to have confounding variables related to frailty status, such as other musculoskeletal disorders, lower-limb muscle strength, and physical balance. 48
This study had several limitations. First, the KCL is used as an effective tool for considering the need for long-term care support for patients due to aging. However, it is not a frailty-specific indicator. Although frailty and osteoarthritis have different disease concepts, they have many common factors that predispose to the progression of both disease processes. Therefore, we cannot report that actual frailty can be accurately assessed only by the KCL scale for patients with osteoarthritis. Thus, comprehensive assessments using some evaluation scales may be necessary for the diagnosis and management of frailty in patients with lower-limb osteoarthritis in future studies. Second, we did not evaluate physical functions, such as walking speed, so we could not compare it with other frailty scales. The validity of the KCL as a frailty scale for assessing patients with OA requires validation. Third, preoperative selection bias, which could have been introduced by patients with OA who chose not to undergo surgery but may have been frail, was not addressed. Fourth, this study included only older people who completed the KCL preoperatively and at the final follow-up. In addition, this was a single-center study with a small sample size, so our results might not apply to a broader. Fifth, we only evaluated patients after surgery for < 1 year, so it was quite possible that social frailty could have improved over the long term. Finally, because of the difference in sample sizes, it was not possible to assess any adverse effects during the postoperative course of THA and TKA. Thus, further multi-institutional studies with longer follow-up and evaluation for other factors related to frailty should be conducted to confirm our results or provide more context.
Conclusion
We examined the prevalence of frailty by KCL, the improvement in frailty in patients with OA following THA and TKA intervention, identified the characteristics of each frailty domain over the shortterm postoperative period, and identified the preoperative factors predictive of persistent postoperative frailty. Our 6 months postoperative results demonstrated that physical frailty and the frequency of frailty were decreased after total arthroplasty procedures, but social frailty did not improve. Moreover, the remaining frailty after surgery was independently associated with preoperative older age and lower IADL. Thus, longer follow-up after surgery and comprehensive interventions, including addressing social aspects, appear to be essential for improving social functioning, especially in low-activity patients with OA.
Footnotes
Acknowledgments
The authors are grateful to the members of the rehabilitation staff at Kyushu University Hospital for their assistance with data collection. This study did not receive any grant founding. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sections.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki and was approved by our hospital ethics review board (approval number: 2019-016).