
Abstract
Introduction:
Total femoral replacement(TFR) is a well-recognized salvage procedure performed after multiple failed endoprosthetic replacements, which result in severely compromised bone stock and damaged structural integrity. TFR is performed as an alternative to lower limb amputation, restoring femoral integrity and enabling patients to resume ambulation. TFR is expected to be performed more frequently as the worldwide rate of revision arthroplasty increases due to improved patient survival rates and their underlying diseases, exceeding the functional life of endoprosthetic arthroplasty. We present a 74-year-old, overweight woman with an extensive surgical history with respect to her right knee. Her right lower extremity x-rays showed a long-cemented stem knee tumour prosthesis and a Garden 4 subcapital fracture of the ipsilateral hip. Due to multiple surgeries of the knee and femur in the past, a total femoral replacement was required to be performed. The procedure was successful, and the expected outcome was met. A successful procedure performed by a skilled and experienced surgical team, a thorough rehabilitation program, and prompt post-operative management of complications, can overcome the high incidence of infection and dislocation to preserve the limb with improved functionality and reduce pain. TFR is a drastic operative intervention that can preserve the quality of life for most patients.
Keywords
Introduction
Total hip and knee arthroplasties have grown exponentially in popularity over the last 2 decades mainly due to a large aging population. As a result, the most common cause of hip revision surgery is instability and mechanical loosening usually associated with bone loss. Other reasons include fractures, dislocations, infection, and implant recall.
Endoprosthetic revision surgeries have and will continue to have a much higher impact and significance in orthopaedic surgery since the indications for revision have been extended to younger patients. However, the restricted longevity shown to date by all arthroplasty devices will result in patients undergoing at least one revision surgery 1 in today’s longer lifespan. The challenges faced now are not only the increase in the number of procedures being performed, but also the degree of difficulty due to patients’ history of previous surgeries, including revisions with local necrotic tissue and inadequate wound healing. 2,3
The lower extremity’s primary function is to support the body’s weight while also allowing painless ambulation. One of the major goals in the reconstruction of bone defects after multiple revision surgeries is to maintain said function. 1 If it is not possible to fully restore proper function to the lower limb, then the next goal of revision surgery is to restore as much function as possible to increase the patient’s quality of life.
Various surgical techniques for reconstructing and stabilizing massive bone defects have been described in the literature, including the use of tumour endoprostheses. Endoprostheses are metal reconstructions that not only replace the entire resected bone segment, but also the corresponding joint. In several cases, endoprosthetic reconstruction has made limb-salvage surgery possible, leading to a steady reduction in the rate of amputation. 4 Endoprosthetic replacement (EPR) is an option for the management of massive bone loss that can result in contained to massive uncontained defects in the acetabulum and segmental defects in the femur from malignant or benign bone tumours, infection, or mechanical loosening around failed lower limb implants. 1 The use of this procedure has improved significantly, starting with the introduction of custom-made monobloc devices which have evolved to modular devices containing antibacterial coatings. 5 A new era of orthopaedic oncology surgery was marked by the advent of modular endoprostheses in the 1980s. In readily available sets, modular megaprostheses consist of a variety of different components which can be assembled in different configurations to better fix the particular bone defect. This eliminates the fabrication delay (4-6 weeks) of the custom-made models so that surgery can proceed smoothly in a timely manner. More importantly, the surgeon is granted further freedom of choice in order to reconstruct defects that may vary from what the preoperative planning suggested. In addition, they proved to have a lower rate of mechanical failure and are easier to fix since only the failed components need to be removed during revision surgery. 6
Replacing the entire femur, including the knee and hip joint, is considered the most extreme surgical technique using modular megaprostheses. Total femoral replacement (“TFR”) is used alternatively to lower limb amputation as a salvage procedure. This procedure was first described in the mid-20th century and since then it has been used for both oncologic and non-oncologic surgeries. 7 TFR is thought to be performed more frequently as the worldwide rate of revision arthroplasty increases due to the increased survival rates of patients and their underlying diseases, exceeding the endoprosthetic arthroplasty functional life. 3 Reconstructive orthopedic surgeons are therefore often presented with the so-called shattered femur, described as a femur that is not reconstructible with conventional methods. 1 The TFR revision is primarily performed for periprosthetic infection and for aseptic revision-related extreme femoral bone loss. 3
A fascinating benefit of TFR is immediate fixation, which allows for early mobilization with full weightbearing. TFR can reinstate function and help patients walk again at a compromised level. Regardless, this level of function is still better than what has been achieved following hip disarticulation. 2 Although a number of reports on functional ability following TFR for musculoskeletal tumors have been described, 8 -12 there are only a few reports for non-oncologic cases. 2,13 -16
TFR is a beneficial procedure that allows for early weightbearing and mobility. Its benefits may outweigh those of alternate procedures depending on the case. Due to the degree of difficulty, a certain amount of experience and skill is needed. Cautious selection of the surgical candidate and expectations must be taken into great consideration for the success of this technique. 3
Case Presentation
We present a 74-year-old, overweight woman with an extensive history with respect to her right knee. She had a right total knee replacement (“TKR”) 2 years ago, followed by an open reduction and internal fixation (“ORIF”) using a plate and screw construct after she had a fall, resulting in a periprosthetic fracture. The fixation failed and she underwent a revision of the TKR with a distal femoral replacement prosthesis. Her recovery was compromised by a chronic lateral patella dislocation. An extensor mechanism reconstruction and patelloplasty was successfully performed. The patient complained of right knee pain with weightbearing for the following 7 months. Eventually, the pain became unbearable, leading to a second revision to change the femoral component to a long-cemented stem. Her history of recurrent problems with her knee were suspicious for septic loosening of the femoral component due to an indolent prosthetic knee infection. She was treated empirically with Vancomycin while waiting for the culture results that came back negative despite the elevated CRP levels. No further follow up regarding her possible infection was recommended, and antibiotic administration was stopped since no positive culture confirmation was found.
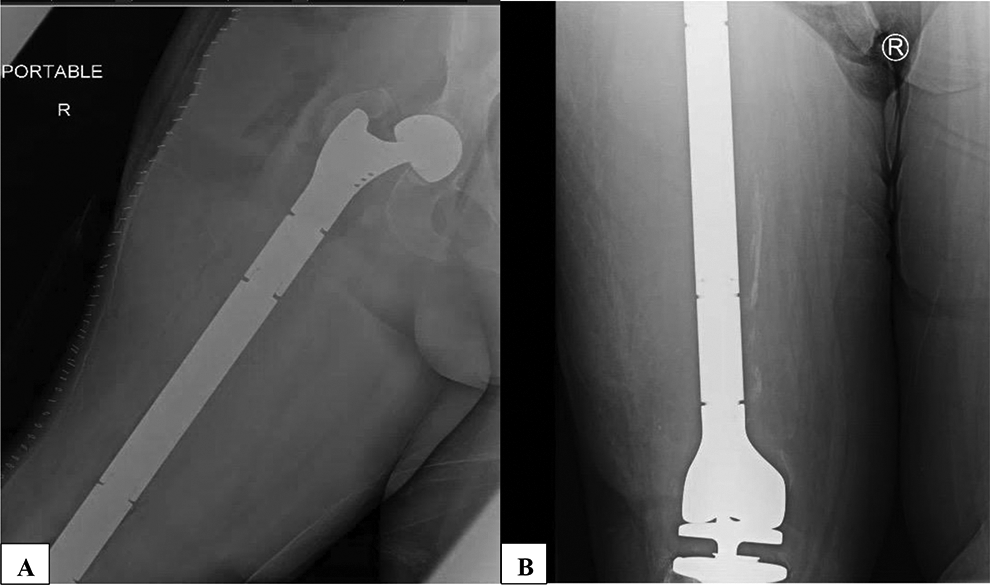
Three months later, she tripped and fell and sustained a Garden 4 subcapital fracture of the ipsilateral hip (Figure 1).

(A) Pre-Operative radiograph showing a Garden 4 subcapital fracture of the hip and a long-cemented diaphyseal stem; (B) status of the knee tumour prosthesis.
Her co-morbidities consist of hypertension controlled with amlodipine with no end-organ damage, renal insufficiency, and obstructive sleep apnea supported by a continuous positive airway pressure (“CPAP”) machine. She takes pregabalin to treat anxiety, olanzapine for bipolar disorder, fluoxetine for depression, and hydromorphone for pain relief.
Upon admission, her physical examination revealed an externally rotated right lower extremity, normal neurovascular status distally, and a well healed midline surgical incision of the knee with bruising around the incision site. Her right lower extremity x-rays showed a long-cemented stem knee tumour prosthesis and a Garden 4 displaced subcapital fracture of the hip.
Given that she was at high risk of developing avascular necrosis of the femoral head, open reduction internal fixation (“ORIF”) would be unlikely to succeed, and a bipolar hip hemiarthroplasty would not have fit due to the long-cemented diaphyseal stem. Therefore, a TFR was performed.
Surgical Procedure Summary
The patient was placed in the lateral decubitus position. A lateral transgluteal approach was used, which was extended to the distal femur. The IT band was split in line with its fibers and extended distally to Gerdy’s tubercle. The femoral head was identified and removed, and the greater trochanter was osteotomized with the abductor mechanism attached for later re-attachment to the prosthesis. The entire femur was skeletonized with careful subperiosteal dissection using electrocautery for the purpose of maintaining full thickness tissue. The distal femur was fully exposed, and the link attached from the femoral stem to the hinged knee component was identified and removed (Figure 2). The entire femur was then removed (Figure 3A).

The entire femur skeletonized preserving full thickness tissue.

(A) Postoperative excised femur; (B) Assembled modular TFR; (C) Total femoral prosthesis with re-attached greater trochanter and abductor mechanism seen through an extended lateral approach.
A TFR construct, STRYKER GMRS trial with 15 degrees of anteversion, was prepared on the side table based on previous radiograph measurements and the length was confirmed with side-to-side comparison (Figure 3B). A trial TFR with a bipolar component was used. The distal trial component was connected to the hinged knee component. The hip component was then reduced to the acetabulum. Stability was tested and confirmed (video attached).
Once the final prosthesis was inserted (Figure 3C), the greater trochanter was cerclage wired to the trochanteric femoral component. Stability was then confirmed. The wound was closed by planes in the usual fashion. The wound was then protected with a customizable PREVEENA dressing at minus 125 mm/Hg.
Post-Operative Course
During the first week post-surgery the patient was treated bed to chair. The second week she was up weightbearing as tolerated(“WBAT”) with a walker. PREVEENA dressing was discontinued at 7 days. After the second week the patient was discharged to a rehabilitation hospital. At the latest follow up of 8 weeks, the patient was seen at the fracture clinic. She was walking WBAT with a roller walker. She had minimal discomfort. There was no infection and no dislocations.
In this case, a TFR was indicated. The procedure was successful and the expected results were met (Figure 4).
(A) Post-Operative radiographs of the right hip with a bipolar component, and re-attached greater trochanter; (B) Knee demonstrating excellent alignment, and fixation of the prosthesis.
Discussion
The first TFR was performed in 1952, and a second case was reportedly conducted in 1965 using a custom-made vitallium endoprosthesis, with a successful functional outcome at 6 months. 7 Marcove et al. 17 identified the first reconstructions with complete replacement of the femur after resection of malignant neoplasms. The first modular expandable prostheses were subsequently introduced for skeletally immature sarcoma patients. 18 Nowadays, EPR is a commonly used treatment method. However, it is associated with technical difficulties, including: the reconstruction of the abductor mechanism, soft tissue coverage, and hip joint biomechanics. The popularity of limb salvage procedures has increased markedly due to a better understanding and improved operative techniques, better patient selection, and advances in prosthetic design. Amputation may be reserved in cases of failed reconstruction of complex periprosthetic fractures, or failed internal fixation. 19
There are 4 main components of the implant: (i) a metallic stem that anchors the prosthesis to the remaining femur, (ii) a metallic distal femur replacement that fills the defect caused by distal femur resection, (iii) a prosthetic replacement of the proximal tibial articular surface, and (iv) a rotating hinge knee joint linking the prosthesis of the distal femur and the proximal prosthesis of the tibia. These implants were originally custom-built and took several months to manufacture. These reconstruction systems are now off-the-shelf modular products that allow length adjustment at the time of surgery. 20 Various antibacterial coating technologies have proved to be safe and efficient both in preclinical and clinical trials, with post-surgical implant-related infections reduced by 90 percent in some cases, depending on the form of coating and experimental setup used. 21
Easy post-operative recovery, a stable joint, immediate weight bearing, and quick functional use of the extremity, are the key advantages of an endoprosthetic implant. Related causes of failure of the prosthesis include infection, aseptic loosening, bone resorption and fracture. 20 Finally, reconstruction should achieve a successful functional outcome consistently so that the limb is at least as functional after amputation as an external prosthesis. 22 The improved function given by limb-sparing surgery is supported by data. It was expected that the quality of life of patients undergoing limb rescue operations was superior to that of patients undergoing amputation, but various studies have shown no progress in mild or moderate quality of life changes. While amputation complications are less prevalent than those from limb salvage procedures, the possible decrease in morbidity is offset by the perceived increase in functionality and more suitable cosmetic appearance provided by the procedure of limb rescue. 20 Amputation may eventually be required in patients with complex periprosthetic fracture patterns and those undergoing ineffective internal fixation. 19
Two types of total femoral arthroplasty are available: (i) the intramedullary total femur and (ii) the tumour style total femoral arthroplasty. The intramedullary total femur is composed of a modular hip, femoral component and a constrained knee femoral component with an intercalary segment. This system is indicated whenever a possibility exists for the preservation of the femoral bone stock. Maintaining muscle attachment is its main advantage; however, there are several situations in which no femoral bone stock is remaining and a tumour-type total femoral arthroplasty system is therefore required. 1
The first decision in the planning of the operation is whether or not an intramedullary total femur is required or whether or not there would be a need for a tumor-type total femoral arthroplasty device. Anteroposterior and lateral radiographs of the whole extremity, as well as a long alignment film of both extremities should be obtained. In the form of a scanogram with a metallic marker, the alignment radiograph can compensate for magnification and assist in measuring the length of the intact contralateral femur and extremity. The basic principles of acetabular revision should be adopted for the acetabular reconstruction, but constrained components can be suggested in the presence of a compromised soft-tissue envelope. A modular tibial component with stem wedges and augments is extremely helpful and often needed with regard to tibial reconstruction. Standard procedures for reconstruction of the tibia should be accompanied by allograft requirements for the acetabulum or tibia. When considering an intramedullary total femur construct, strut allografts and cerclage cables may be needed on the femoral side. If a tumour-style total femoral arthroplasty is to be performed, subperiosteal dissection of the entire femur will be conducted, the tibial component will be removed and the tibia will be prepared to accept a long-stemmed tibial revision component. The tibial component will be suitable for a rotating hinge articulation. In an attempt to assess soft-tissue stability and leg-length equality, trial reduction will be performed. After the trial reduction, the tibial component is placed either in a hybrid fashion with proximal cementation and distal press-fit fixation or in a fully cemented technique. The entire femur is introduced through the knee wound. It is then fixed to the knee tibial base plate with the appropriate bushings, axle, and yoke and then reduced in the acetabulum with the appropriate head/neck unit. 1
A number of reports on functional ability following TFR for musculoskeletal tumors have been recorded using the Musculoskeletal Tumor Society (MSTS) scoring system with a mean of 71.15%. 8 -12 According to Kalra et al, the survival of the prosthesis without revision surgery was 100% at 5 years and 80% at 10 years. 9 Similar success has been shown by Puri et al who reported an implant survival of 88% at 5 years with only one TFP needing removal because of infection. 11 Concerning the non-oncological cases, Toepfer et al reported in his study that patients treated by TFR with modular total femur prosthesis had a mean MSTS score of 10 ± 4 out of 30. 2 Moreover, Amanatullah et al conducted a retrospective review showing that following non-oncologic TFR, patients had strong pain relief and improved function. Harris Hip score (HHS) rose to 65.3 ± 16.9 from an average of 30.2 ± 13.1. 13 A retrospective study of 100 non-oncological TFRs with a minimum of 5 years of follow-up from Endo-Klinik has recorded similar improvements in patient-reported hip and knee outcomes. Eneking scores increased from 1.25 pre-operatively to 3.29 post-operatively for the hip and from 2.09 pre-operatively to 3.29 post-operatively for the knee. 16 In a retrospective study of 59 non-oncologic TFRs, 98% regained ambulation at 4.8 years of follow-up, but 57% needed at least one cane for ambulation. 14 In another retrospective review on 14 patients who have undergone TFR, an improvement in overall function has been made in all patients, as determined by the MSTS scores. The mean MSTS score was 23% before surgery and this rose after surgery to 59%, with 4 patients reaching a 75% improvement in their function. 15 Although these changes reflect modest increases in overall function, complete or near complete pain relief was experienced by 80% of the patients with a 70% implant survival rate at an average of more than 5 years of follow-up. The major complications of non-oncological TFR were infections followed by dislocations, with a recurrent infection rate of 25% and a recurrent dislocation rate of 20%. 13 Despite the high complication rate found in our complex patient population, non-oncologic TFR remains an effective treatment in the setting of massive femoral bone loss in the multi-revised THA or TKA, providing patients with better quality of life, functional improvement and pain relief.
Conclusion
Patients with end-stage prosthetic disease have a severely compromised femoral and acetabular bone stock where significant fixation is not a feasible choice for either THA or TKA. A successful procedure performed by a skilled and experienced surgical team, a thorough rehabilitation program, and prompt post-operative management of complications, can overcome the high incidence of infection and dislocation to preserve the limb with improved functionality and reduced pain. Taking into account the limited options available to this patient population, TFR is a drastic operative intervention that can preserve the quality of life for most patients. Our case of a 74-year old woman, who underwent a right TFR as a salvage procedure, is an addition to all non-oncological successful reports mentioned before. The main purpose upon conducting such a procedure was to provide the patient with pain relief, early weightbearing, and a better quality of life, while preserving the limb function and mobility.
Footnotes
Author Contributions
Conceptualization, Jose Guerra, Patrick Chaghouri; writing and editing, Jose Guerra, Patrick Chaghouri, Jose Andres Guerra, Sophia Lorina Peters; review, Jose Andres Guerra, Sophia Lorina Peters; supervision, Jose Guerra; All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.