
Abstract
Introduction:
There is current debate about which type of total hip prosthesis implants are best for the elderly patient. Implanting uncemented total hip arthroplasty (THA) in elderly people remains contested. The aim of present study was to evaluate the outcome of the uncemented Zweymüller BICON-PLUS THA in those with a minimum of 80 years of age.
Materials and Methods:
A retrospective data collection was performed in a regional teaching hospital in the Netherlands. The primary outcome of interest was the operation-free period. Secondary outcomes included the revision rates of the femoral and acetabular components and postoperative complications of the procedure. After a follow-up of at least 7 years, the surviving patients were reviewed on functionality using validated scores (Hip Disability and Osteoarthritis Outcome Score, Timed Up and Go, and Harris Hip Score) and radiographic analysis.
Results:
Between January 1999 and September 2004, 124 patients (128 THAs), aged 80 years and older, received an uncemented THA with a BICON-PLUS cup and SL-PLUS stem. The overall operation-free period was 6.5 years. One case of loosening of the cup was found among participants, with a survival rate of 99.2% of the BICON-PLUS cup in the analyzed group. In all, 28.8% of this group could be followed for a postoperative period of at least 7 years. The remainder of the patients died prior to the end of the 7-year period. Of these, 16.0% were eligible for clinical review. This group showed good function without evident signs of prosthetic loosening.
Conclusion:
The uncemented Zweymüller THA system, with threaded BICON-PLUS cup and SL-PLUS stem, showed good results, compared to outcome of other THA systems in elderly individuals. Therefore, it is a reliable option in older patients requiring THA.
Introduction
In the past decades, there have been considerable changes in the type of hip prostheses used in clinical practice. During the 1970s, Zweymüller and colleagues developed a threaded acetabular cup, in combination with a cementless femoral stem. This so-called cementless Endler all-polyethylene cup showed unacceptable rates of aseptic loosening. This cup was replaced by a cementless titanium-backed threaded cup, with polyethylene liner, in the mid-80s (CSF-cup). This second generation was designated Alloclassic. In 1992, the third-generation Zweymüller Total Hip Arthroplasty, the Endoplus, was introduced, with minimal modifications of the stem (SL-PLUS) and the cup (biconical, BICON-PLUS).
The Zweymüller Alloclassic cementless stem, with CSF threaded cup, has shown excellent long-term results. 1 –6 Thus far, only 3 survival studies, focusing on the BICON-PLUS threaded cup, have been published. These studies show an intermediate survival rate of 98% to 100%. 7 –9
The primary reason for developing cementless total hip arthroplasty (THA) was the high rates of failure of cemented femoral components in younger and more active patients, as reported in older studies. 10,11 Limited studies of cementless THA are focused on the outcome in elderly individuals. 12,13 Several reports indicate a preference for uncemented fixation in frail patients with significant cardiovascular risk factors. Makela et al described data from the Finnish Arthroplasty Register, with cementless prostheses showing similar long-term survival rates, compared to cemented implants, in patients aged 55 years or older. 14 Based on data by the Finnish Arthroplasty Register, the cemented THA is considered the treatment of choice for severe osteoarthritis in the elderly patients. 15 In general, most reports, evaluating methods of fixation, have focused on hemiarthroplasty. 16,17 Several of these studies state cemented fixation as being the method of choice for hemiarthroplasty in elderly patients.
Increasing survival rate is observed for prostheses with cementless fixation. This could be attributed to new technologies and design changes, such as fixation modifications (materials and coatings) and stem geometry. In general, long-term survival of the cementless femoral stem is superior to the survival of the cementless cup. 18
Despite excellent survival rates of the Zweymüller THA, there are reservations in applying a cementless prosthesis in elderly patients due to insecurities about sufficient grip, bone stock, and bone quality. Still, high-level evidence to support the use of a cemented versus an uncemented prosthesis in the elderly individuals is lacking. The aim of the present study was to evaluate the operation-free period of the Zweymüller BICON-PLUS THA, in patients aged a minimal 80 years. Secondary outcomes included revision surgeries and complications. Also, patients alive, with more than 7 years of follow-up, were reviewed for clinical and radiological data.
Materials and Methods
Study Design
A retrospective cohort study was performed, analyzing patients aged 80 or above, at time of implantation of the Zweymüller BICON-PLUS THA. In addition, in a prospective follow-up, all patients who were alive at the time of study and completed a postoperative period of at least 7 years were evaluated at our outpatient clinic. The patients were recruited and examined as part of the standard local follow-up protocol and after informed consent.
Study Procedures
Retrospective
Between January 1999 and September 2004, a total of 124 patients aged above 80 years received a primary cementless THA. During this time frame, 4 patients received bilateral THA. In total, 128 total hip prostheses were implanted in this group. All 128 THAs operated were included in a database using patient medical records and data from the outpatient clinic including demographics and the American Society of Anaesthesiologists (ASA) physical fitness status. 19 The operation-free period was considered as the end point. Secondary revision and complications were recorded. Three patients were excluded from the study because of missing postoperative data. As a result, 125 THAs were included in our analysis.
Prospective
Of the 125 THAs in 124 patients, 36 were alive and 20 were eligible for collecting clinical and radiological data prospectively as part of the local follow-up protocol (Figure 1). The clinical results were assessed using the validated Hip Disability and Osteoarthritis Outcome Score (HOOS) 0 to 100 and the Harris Hip Score (HHS) 0 to 100. 20 The HOOS is a patient-reported outcome questionnaire and validated for hip symptoms. 21 Additionally, the Timed Up and Go (TUG) test was performed. 22 This test measures duration of getting up from a chair, walking 3 m, returning, and getting back to sit. Patients were asked to rate their satisfaction regarding their THA on a visual analogue (VAS) scale (0-10 excellent to poor). Standardized radiographs were obtained: plain pelvis anterior–posterior and axial views. All radiographs were reviewed and analyzed by an independent researcher. Analysis of the radiographs was focused on the position of the prosthesis, possible migration, and radiolucency, according to the Gruen zones for the stem and the DeLee and Charnley zones for the cup. 23,24
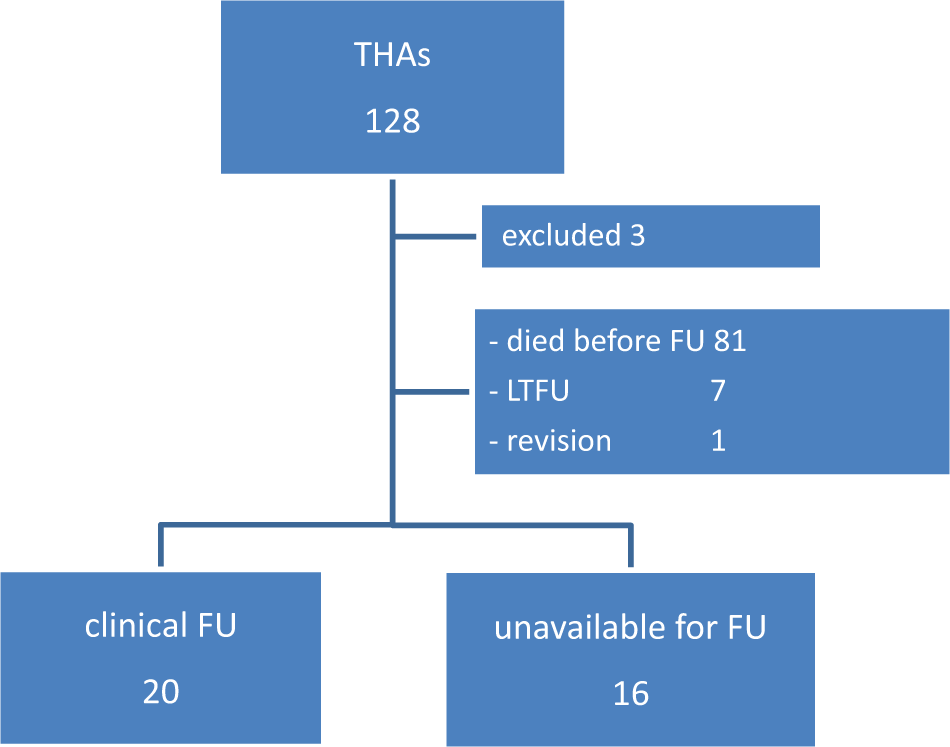
Flowchart of total hip arthroplasty (THA) distribution after 7 years.
Statistics
All analyses were performed using SPSS version 18.0 (SPSS Inc, Chicago, Illinois). Descriptive statistics include number (percentage), mean (standard deviation [SD]), and median. The operation-free period was calculated by the time from initial implantation to the date of first documented revisional surgery. Patients free from reintervention were censored at the date of last follow-up or date of death. Secondary cup or stem revision was defined as removal, exchange, or addition of any component.
The prospective study was analyzed on patient characteristics and the results of the functional tests. These are presented as mean (SD) or median (interquartile range) in case of skewed distribution.
Results
Retrospective
Patients and procedures
A total of 125 THAs, comprising 121 individuals, were included in the analysis: 95 women and 26 men with a mean age of 83.8 years. Seven patients had a physical status category ASA 1, 84 patients ASA 2, 32 patients ASA 3, and 1 patient ASA 4 (fracture). Fifty-one percent of this group were operated on the right side. Osteoarthritis (103) was the most frequent diagnosis as indication for surgical intervention. The rest of the diagnosis consisted of osteonecrosis of the femoral head (4), fracture (17), and pathological fracture (1).
Complications
In 102 (81.6%) procedures, there were no complications. There were 25 complications in 23 implanted THAs (Table 1). Two complications occurred during the operation. In 1 patient, there was a rupture of the gluteal musculature. Another patient experienced cardiac dysrhythmia and died within 1 month after surgery. Of the 125 analyzed cementless THAs, 1 patient required reoperation, due to infection. This patient presented with a wound infection after 20 days and cultivation showed Escherichia coli, sensitive for all antibiotics. The wound was opened and flushed in the operation theater, the infection was subcutaneous, and the fascia was intact, with retention of the THA. Afterward prolonged administration of intravenous cephazolin and later oral ciprofloxacin cured the infection. Eight patients experienced wound leakage and required antibiotics. This resulted in prolongation of the hospital length of stay without surgical intervention. There were no peri- or postoperative femoral fractures.
Complications.

Abbreviation: THA, total hip arthroplasty.
Survival of patients
Retrospective
Of the 121 patients, 81 died within 7 years after the operation. Analysis of the overall survival of the patients showed a median operation-free period of 6.5 years (95% confidence interval [CI] 5.0-8.0) for all patients (range 0-12 years). This was 6.9 years (95% CI 4.9-8.9) for the group aged between 80 and 90 years (n = 116) and 2.4 years (95% CI 1.7-3.1) for patients aged 90 years and older (n = 5). All deceased patients had the THA in situ.
In the analyzed group of 125 THAs, there was 1 cup revision (0.80%) due to aseptic loosening 25 months postoperatively. The overall survival of the BICON-PLUS cup in the analyzed group was 99.2% (124 of 125). There were no femoral stem revisions in this group.
Prospective
From the 125 analyzed THAs, 36 (in 34 patients) could be retrieved and 20 THAs could eventually be clinically reviewed (Figure 1). The remaining 16 THAs were unavailable for follow-up due to unwillingness to participate (n = 5), or poor health conditions made the patients unable to participate in the follow-up (n = 11). The clinically evaluated group of 20 THAs consisted of 2 men and 16 women, with a mean age of 88.9 years and a mean follow-up of 7.9 years (Table 2). Patients had good functions with median scores between 87.5 and 96.2 on the HOOS subscores. The mean score on the HHS was 82.7 and ranged between 61 and 100. The TUG test had a mean of 15 seconds. Of the interviewed patients, 95% considered THA as an improvement and rated it with a 7.9 on a 0 to 10 bad to excellent scale.
Clinical Results of THAs at 7 Years FU (20 THAs).

Abbreviations: THA, total hip arthroplasty; SD, standard deviation; IQ, inter quartile; TUG, Timed Up and Go; HOOS, Hip Disability and Osteoarthritis Outcome Score; HHS, Harris Hip Score; QoL, quality of life; FU, follow-up.
aData are presented as mean (SD) or median (IQ range) in case of skewed distribution.
bn ≥ 5 missing cases.
c5 ≤ n ≥1 missing cases.
In all patients, the position of the prosthesis was satisfactory; no migration was seen on the radiographs. Further evaluation showed radiolucency and osteolysis in several patients, mostly in the upper zones of the femur (Figures 2 –4). In 3 patients, the osteolysis was both seen in zone 7 and 14. Osteolysis was seen in 2 patients in zone III of the cup. These were different patients than those with osteolysis in zone V (2 patients). Five patients showed radiolucency in Gruen zone one. In all patients, the position of the prosthesis was satisfactory according to the safe zones by Lewinnek (Figures 5 and 6). 25

Osteolysis.

Radiolucency by DeLee and Charnley (acetabulum) and Gruen (femur), anterior–posterior (AP) view. Reproduced with permission and copyright © of the British Editorial Society of Bone and Joint Surgery. 1

Radiolucency by DeLee and Charnley (acetabulum) and Gruen (femur), lateral view. Reproduced with permission and copyright © of the British Editorial Society of Bone and Joint Surgery. 1

Radiograph, anterior–posterior (AP) view.
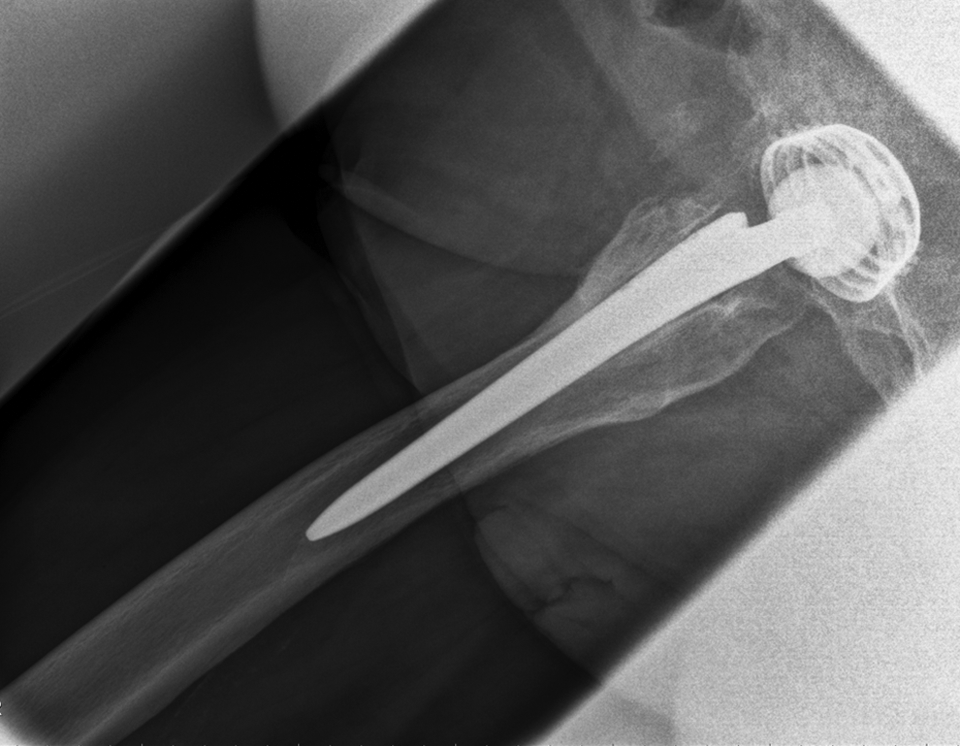
Radiograph, lateral view.
Discussion
Our study demonstrates the outcome of the cementless Zweymüller BICON-PLUS cup and SL-PLUS stem in an elderly population, aged 80 or above, with an operation-free period of 6.5 years with 1 cup revision reported. The group that was clinically evaluated had good functionality, in accordance with other studies. 1,26 After 7 years, the THA showed acceptable functional results, given patients’ age, in 18 patients with 20 THAs. The outcome of the TUG test (15.0) was similar to the measured TUG test outcome (14.2 seconds) from a comparable population (n = 245). 21 The radiographic analysis showed more extensive osteolysis around the cup in only 3 patients and in 2 patients around the stem. However, the clinical consequences of these data may be limited. 1 Previous studies about the Alloclassic stem showed osteolucency was a common sign in the proximal regions, without specific association with loosening. This effect seemed to be the result of the distal gripping of the stem. Our radiographic data must therefore be interpreted with care.
Generally, there are only limited studies focusing on cementless implants in elderly patients. We found a survival rate of the BICON-PLUS cup, in the analyzed group, of 99.2%. A 10-year survival rate exceeding 90% is commonly regarded as a good long-term outcome (National Institute of Clinical Excellence). 27 The long-term survival of the Zweymüller Alloclassic cementless stem and cup are well studied, showing high survival rates in accordance with our study. 2 –4,28,29 Makela et al reported data of the Finnish Arthroplasty Register. 15 They showed survival rates of 88% to 92% of different cementless cups, in patients aged 55 years and older, after 15 years of follow-up (the PCA Pegged excluded). In this series, the cementless Zweymüller cup was not included. Another study, with data from the Finnish Arthroplasty Register, focused on patients aged 80 years and older with implanted THA. This study demonstrated a survival of 97% after 5 years, with revision of the THA, for any reason, of a total of 6989 THA’s implanted (Zweymüller not included). 13 The reversed hybrid THA’s showed the best outcome. Vervest reported 96% cumulative survival of the cementless Alloclassic Zweymüller cup, after a minimal follow-up of 10 years. However, this group consisted of younger patients (average age 61.1 years). 29 We are aware that the long-term survival of the prosthesis is not the biggest concern when implanting a THA in the elderly patient.
Many surgeons are cautious in applying a cementless acetabular cup in the elderly population due to doubts concerning the bone quality with subsequent fixation of the cup. Level 1 evidence does not exist to guide decision-making for total hip component selection in the elderly patient. A titanium biconical threaded cup is quick, reliable, and easy to implant and does not require cementation. 7 –9 In cementless total hip prostheses, the uncemented cup appears to be the component associated with increased risk of revision, compared to the stem. 18,27 It is stated that the common cause, for this problem, is increased polyethylene (PE) wear resulting in loosening. 15
A randomized clinical trial from 2012, comparing cemented and uncemented hemiarthroplasty, with use of the Alloclassic stem, reported 6 intraoperative femoral fractures in the uncemented group and even more postoperative fractures. 16 These findings are in contrast to our study, showing no operation-related fractures in patients with potentially poor bone quality. It may be the result of a slightly different design of the Zweymuller SL-PLUS stem compared to the Alloclassic stem.
A recent review showed that there is a higher risk of intraoperative fractures when using an uncemented THA in an elderly patient. 30 The use of a cemented stem is also not without risk. Recently, a high risk of fracture had been reported with the cemented, polished, and tapered stem. 31 The stem may act as a wedge during a fall, splitting the femur.
The rate of wear depends on a multitude of causes, such as the age and physical activity of the patient as well as the mechanical and physical–chemical features of the material. 32,33 In our opinion, these factors are less applicable to a less active elderly population.
Our study has certain limitations. First, the retrospective design could lead to incorrect interpretation of actual results. The mentioned survival of 99.2% may not accurately represent the failure rate, some patients may have had a failed prosthesis but were not fit for surgery or died. This point should also be taking into account for the 16 of 36 patients who were not evaluated in the prospective part of this study. Therefore, these rates need to be interpreted with care, although these effects are inevitable with the natural course of a group of elderly patients. We included different pathologies as reason for a THA which may have biased the outcome.
In conclusion, excellent survival and clinical results were seen in a population, aged 80 or older, undergoing total hip replacement with the cementless Zweymüller BICON-PLUS cup and the SL-PLUS stem.
Footnotes
Author’s Contribution
Each author has participated in the design of the study, has contributed to the collection of the data, has participated in the writing of the manuscript, and assumes full responsibility for the content of the manuscript. All was according to the ICMJE Authorship guidelines.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All patients gave their informed consent prior to being included in the study. All procedures performed in studies involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or with comparable ethical standards.