
Abstract
Background:
Total Hip Arthroplasty(THA) is a surgical treatment for hip disease. A large amount of evidence has been reported on comparing outcomes of neuraxial(spinal or epidural) anesthesia and general anesthesia. However, it is unclear whether nerve blocks(NB) as main anesthesia technique compared with general anesthesia(GA) for THA could reduce perioperative complications. We conducted a retrospective evaluation of NB and GA, using a propensity score-matched analysis(PSMA).
Methods:
A total of 902 patients older than 60 years old with hip disease undergoing primary THA received combined lumbosacral plexus and T12 paravertebral nerve blocks (n = 143) or GA (n = 759) at our institution from 2012 to 2018.Binary logistic regression was used for comparison of the primary outcomes(the incidence of delirium) and the secondary outcomes(the percentage of postoperative hemoglobin(>10g/dl), transfusion(>2 units), major cardiac events(MACE), postoperative pulmonary complications (PPC) and 30-day mortality) in the matched cohorts.Statistical analysis was performed using SPSS v 23.0.
Results:
Both cohorts were balanced in all included parameters after PSMA. The incidence of delirium was lower (OR 0.233,95% CI 0.064-0.845, p = 0.030) in NB group in matched cohorts. In the unmatched and matched cohorts, the percentage of Hb(>10g/dl) was higher in GA group but the incidence of transfusion(>2 units) was higher in NB group. No difference was found in the incidence of 30-day mortality in the unmatched and matched cohorts. In the unmatched cohorts, the incidence of PPC was higher and LOS was longer in NB cohort, but no difference was observed in the matched cohorts.
Conclusion:
In patients older than 60 years old receiving primary THA, NB could be associated with a lower incidence of delirium.
Keywords
Introduction
Total hip arthroplasty(THA) is an effective and long-term treatment for the hip joint disease. 1,2 Due to increased life expectancy and expectation for life quality in the elderly, the number of THA patients is increasing by the year. It is estimated that the demand for primary THA is predicted to grow by 174% to 572,000 by 2030 in the US, and the number of THA performed in the UK in 2035 is estimated to be 95,877. 3,4 Despite tremendous advances in anesthesia techniques and surgical care, THA is associated with high perioperative mortality and morbidity. 5,6 Disability and 1-year mortality are reported up to 80% and 27% respectively. 7,8
De Visme et al. has proved that lumbosacral plexus blocks are a logical alternative to GA and SA for hip surgery. Besides, it has an advantage in limited sympathectomy and bladder paralysis. 9 Ultrasound-guided nerve blocks with nerve stimulator increase the success rate and reduce risks such as nerve injuries, undesirable spread-hematoma and renal puncture. 10 Combination of lumbosacral plexus and T12 paravertebral nerve blocks compared with lumbosacral plexus alone provide better analgesia, especially for the territory of the greater trochanter. 11
Postoperative delirium is common in orthopedic patients, especially with elderly patients. 12 Recent studies show that delirium is associated with negative outcomes and mortality. 13,14 It may also increase the risk of post-discharge dementia. 15 There is no consensus for the unique anesthesia technique to decrease the incidence of delirium.
In order to address this issue clearly, a propensity score-matched analysis(PSMA) is used, which is an after randomization method and a tool to balance the known confounders in the observational cohorts. 16,17 We performed a PSMA in our retrospective cohort study for the patients receiving THA in our hospital from 2012 to 2018, comparing the 2 different anesthesia techniques NB and GA on perioperative morbidity and mortality.
Materials and Methods
Database and Study Design
After approval from Ethics Committee of Changzhou First People’s Hospital, the third affiliated hospital of Soochow University, we used the hospital electronic database to access the medical records including medical history, laboratory examination, surgical and anesthesia procedures and clinical outcome data. Follow-up was achieved using a telephone questionnaire.
Study Cohort
All 902 patients undergoing primary THA at the Third Affiliated Hospital of Soochow University a 2182-bed tertiary teaching hospital, from 2012 to 2018 were enrolled retrospectively in our research. The inclusion criteria were indications for primary unilateral THA older than 60ys. The exclusion criteria were:(1)receiving bilateral arthroplasty;(2)undergoing general or regional anesthesia within 3 months;(3)revision arthroplasty;(4)multiple injuries;(5)patients younger than 60ys. The included cases were divided into 2 cohorts according to the anesthesia technique (GA versus NB). The primary outcomes were the incidence of delirium. The secondary outcomes were the percentage of postoperative hemoglobin(>10g/dl), transfusion(>2 units), MACE, PPC, and 30-day mortality. Demographic data(including age, gender, principal diagnosis, American Society of Anesthesiology(ASA) physical status classification), preexisting comorbidities (including diabetes, anemia, pulmonary function(PF), myocardial infarction(MI), congestive heart failure (CHF), chronic renal failure(CRF) and the revised cardiac risk index(RCRI)), procedures and postoperative complication were extracted independently by 2 researchers. PF was stratified into 0, 1, 2 and 3 representing none, mild(FEV160-80%), moderate(FEV140-60%) and severe(FEV1 <40%) according to pulmonary function test. Delirium was diagnosed according to the confusion assessment method(CAM). PPC was diagnosis by clinical presentation and chest imaging.
Patients in the NB cohort received the ultrasound-guided combination of lumbosacral plexus and T12 paravertebral nerve block with nerve stimulator using 0.33% ropivacaine. Dexmedetomidine(0.5ug/kg) was intravenously infused 10 minutes before blocks, and 5ug sufentanil was given before lateral positioning. In the lateral decubitus position, ultrasound-guided lumbar plexus block (L3–4 vertebral space level, 0.33% ropivacaine 30 mL) and sacral plexus blocks (0.33% ropivacaine 20 mL) were performed followed by T12 paravertebral block(0.33% ropivacaine 10 ml). The needle position was confirmed by a quadratus femoris twitch for lumbar plexus block and gastrocnemius twitch or foot dorsiflexion for sacral plexus block at a current 0.5 mA by nerve stimulator. In general anesthesia cohort, the induction was conducted with propofol, sufentanil and muscle relaxant followed by intubation or LMA. Anesthesia was maintained with sevoflurane.
Statistical Analyses
Chi-square test, Fisher exact test or Mann-Whitney U test were used to compare the baseline characteristics in the unmatched and matched cohorts. PSMA was used to evaluate the cause-and-effect relationship in our retrospective observational research. All the specific proper covariates were selected according to published papers and clinical expertise to avoid unobserved confounders. Nearest-neighbor matching (1:1)with fixed calliper widths(0.02) without replacement was used to form a matched sample, thus proposed causal exposure baseline variables were balanced between NB and GA cohorts. 18,19 A callipers width of 0.02 was applied in our research, as recent studied indicated. 20,21 A balance between matched cohorts was also tested. All variables that could be associated with clinical outcomes were included. These variables included age, gender, ASA score, RCRI grade and comorbidities (hypertension, diabetes, anemia, CHF, pulmonary function, MI and CRF). The discharge proportionality of different anesthesia type in the matched cohort was also assessed. Multivariate regression was used to evaluate the association between anesthesia techniques and dichotomous clinical outcomes(the incidence of delirium, the percentage of postoperative hemoglobin(>10g/dl), transfusion(>2 units), MACE, PPC and 30-day mortality) in the matched cohort and odds ratio(OR) with a 95% confidence interval was also reported. Statistical significance was defined as 2-tailed P < 0.05. Analyses were performed using SPSS 23.0(Version 23; IBM, Armonk, New York).
Results
From 2012 to 2018, a total of 902 patients older than 60ys were identified without missing variables of interest who had indications for total hip arthroplasty(Figure 1). There were 143(15.9%) patients undergoing ultrasound-guided combined lumbosacral plexus plus T12 paravertebral block with the nerve stimulator and 759 patients undergoing general anesthesia. In the unmatched cohorts, most of the perioperative variables including age, ASA class, preoperative commodities and hemoglobin levels were significantly different between the 2 anesthesia cohorts as was shown in Table 1. Patients who underwent NB were more likely to be older, with higher ASA classification, more preoperative commodities.
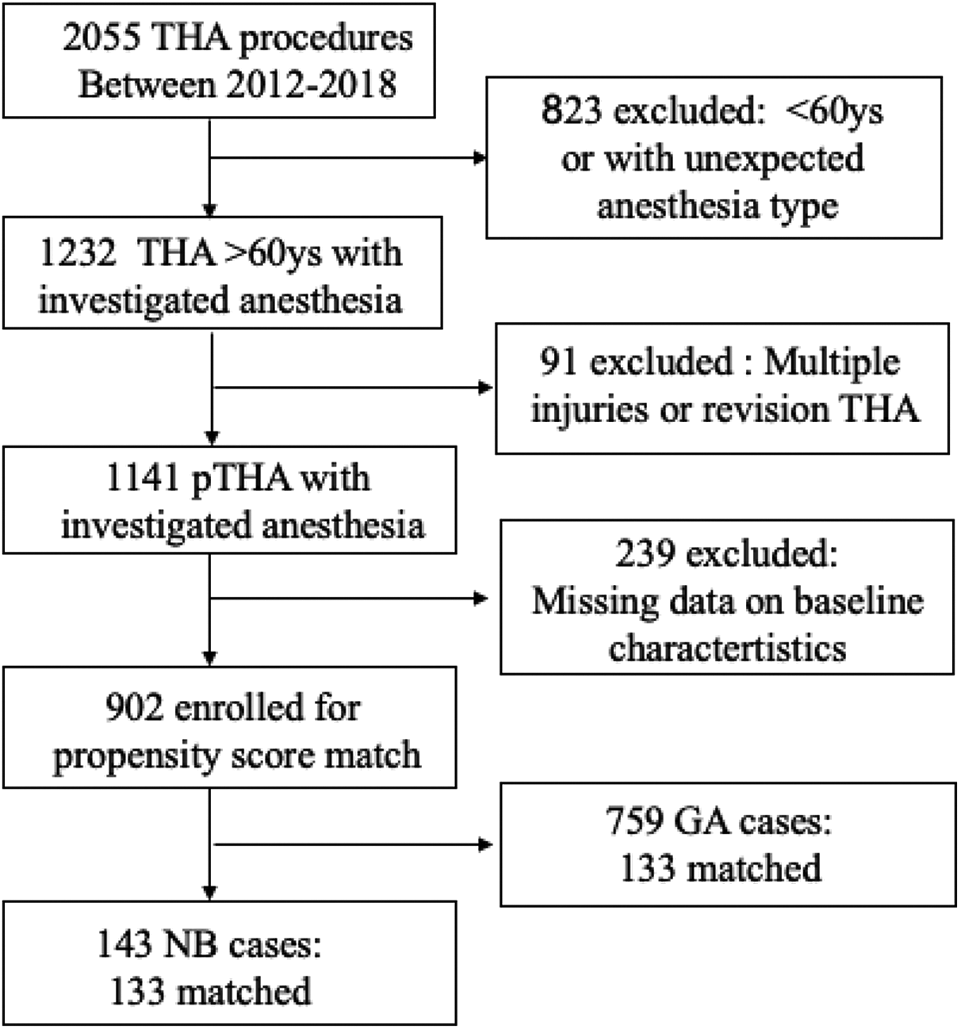
Flowchart of enrollment. THA: Total hip arthroplasty. pTHA: Primary THA. NB: Nerve block. GA: General anesthesia.
Baseline Characteristics of All Patients (n = 902).

MI = myocardial infarction; ASA = American Society of Anesthesiology; PF = pulmonary function; CHF = congestive heart failure; CRF = chronic renal failure; RCRI = revised cardiac risk index; GA = general anesthesia; NB = nerve blocks.
PSMA was used to balance the possible confounders. In our retrospective, observational research, with a caliper width of 0.02,133 cases of general anesthesia patients were matched to 133 cases of regional anesthesia. All the observed variables were balanced between cohorts (Table 2).
Baseline Characteristics in the Cohorts after PSMA.

PSMA = propensity score-matched analysis; MI = myocardial infarction; ASA = American Society of Anesthesiology; PF = pulmonary function; CHF = congestive heart failure; CRF = chronic renal failure; RCRI = revised cardiac risk index; GA = general anesthesia; NB = nerve blocks.
After PSMA, the incidence of delirium was lower (RR 0.233,95% CI 0.064-0.845, p = 0.030) in NB cohort while there was no difference in the unmatched cohorts (RR 0.935,95% CI 0.270-3.234, p = 1.000). In the unmatched and matched cohorts, the percentage of Hb(>10g/dl) was higher in GA cohorts(RR 0.650&0.488,95%CI 0.422 -1.001&0.282-0.845, p = 0.049&0.010) while the incidence of transfusion(>2 units) was higher in NB cohorts(RR 1.605&1.754, 95% CI 1.112-2.317&1.038-2.963, p = 0.010&0.048) in the unmatched and matched cohorts. In the unmatched cohorts, the incidence of PPC was much higher (OR 4.439,95% CI 1.721-11.449, p = 0.004) and LOS was longer(p = 0.037) in NB cohort while no difference was found in the matched cohort. No difference was found in the incidence of 30-day mortality(p = 0.620&1.000) and MACE (p = 0.102&0.735) in the unmatched and matched cohorts (Table 3). Although there was no difference in LOS in the after match cohorts, it showed a general larger percentage of hospital discharge in the NB group(see Figure 2) compared with the GA group. In the multivariable logistic analysis, the incidence of delirium was lower (OR 0.038,95%CI 0.046-0.752, p < 0.05).The incidence of transfusion(>2 units) was higher in NB group while the percentage of Hb(>10g/dl) on the first postoperative day was lower (OR 0.437,95%CI 0.243-0.783, p < 0.05) in NB group compared with GA group. There was no difference in the 30-day mortality(OR 0.591,95%CI 0.049-7.175, p > 0.05), PPC(OR 1.949, 95%CI 0.470-8.070, p > 0.05) and MACE(OR 1.343,95%CI 0.298-6.056, p > 0.05)(see Figure 3).
Unadjusted Outcomes of NB Versus GA Before and After PSMA.
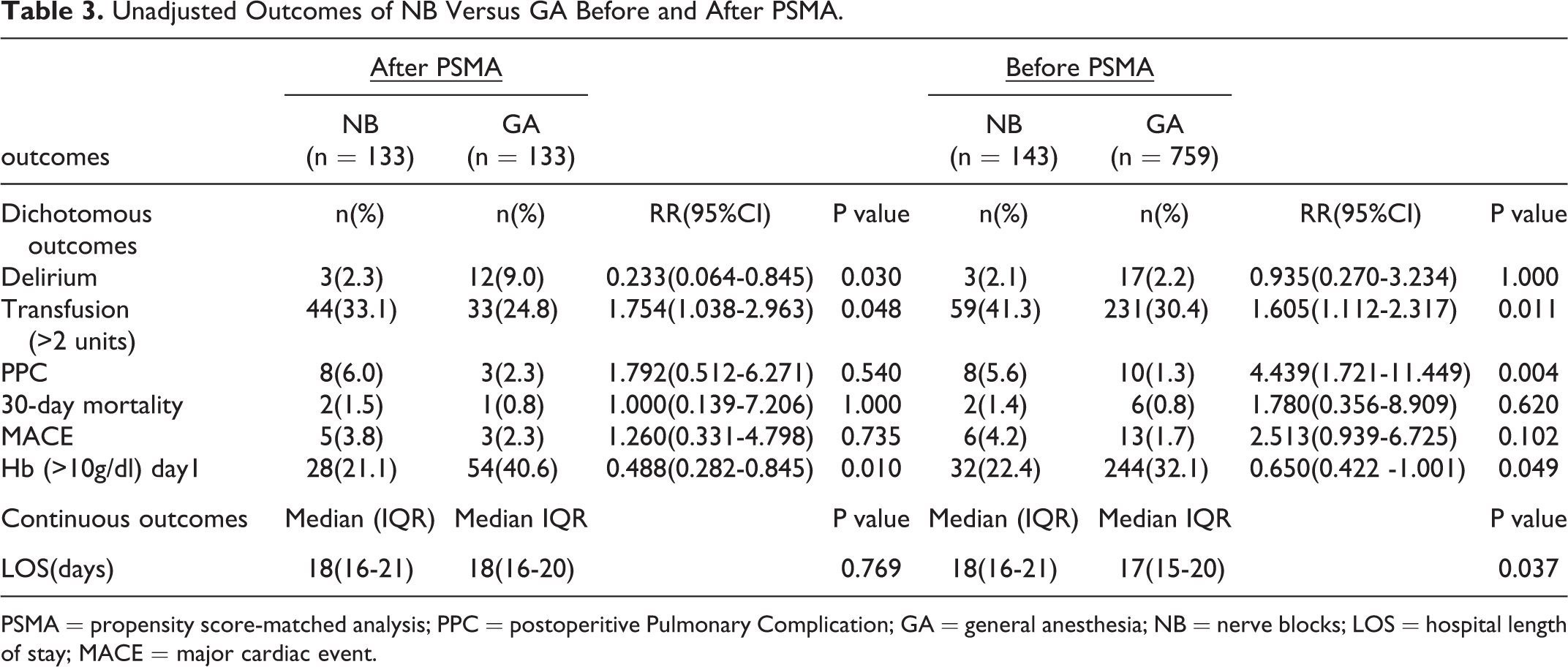
PSMA = propensity score-matched analysis; PPC = postoperitive Pulmonary Complication; GA = general anesthesia; NB = nerve blocks; LOS = hospital length of stay; MACE = major cardiac event.

Percentage of the population discharged from hospital over time. NB: Nerve block; GA: General anesthesia.

Logistic regression analysis result for outcomes comparing NB with GA after propensity score matching. The diamonds indicate the odds ratios and the lines through the diamonds indicate the 95% CI. Postoperitive Pulmonary Complication(PPC);Major Cardiac;Event(MACE);Odds Ratio(OR) nerve blocks(NB);general anesthesia(GA).
Discussion
There are 3 main findings elicited by our retrospective observational cohort study using propensity score-matched analysis. First, the combination of lumbosacral plexus and T12 paravertebral nerve blocks reduces delirium in the patients older than 60ys undergoing primary THA. Second, general anesthesia is associated with a lower percentage of transfusion(>2 units) and a higher percentage of hemoglobin level(>10g/dl) on postoperative day 1. Finally, postoperative pulmonary complication, major cardiac event and 30-day mortality are similar between general anesthesia and nerve blocks.
It has long been controversial whether different anesthesia techniques affect outcomes of THA. There are a large number of studies focused on anesthesia techniques and perioperative complications including RCTs, systematic reviews and multicenter retrospective reviews. A systemic review compared neuraxial anesthesia and general anesthesia pooling 29 studies enrolling 10488 patients undergoing total hip and knee arthroplasty concluded that neuraxial anesthesia was associated with a lower length of hospital stay(LOS) than GA. However, the risks of other morbidity were similar between cohort. 22 The latest study comparing complications following total hip and knee replacement from the National Joint Registry for England, Wales, Northern Ireland and the Isle showed that regional anesthesia was associated with reduced LOS, readmissions, and complications when compared with GA. Thus they recommended the reference-standard for total hip and knee replacement. 23 Another latest systematic review and meta-analysis which analyzed 94 studies and created consensus recommendations spinal vs. general anesthesia for hip and knee arthroplasty concluded that based on current evidence, the consensus group recommended neuraxial over general anesthesia for hip/ knee arthroplasty. 24
However, works of literature comparing NB(combined lumbosacral plexus +/- T12 paravertebral block +/- sedation without intubation or supraglottic device) and general anesthesia are rare. One study compared continuous spinal anesthesia and ultrasound-guided combined psoas compartment-sciatic nerve block for hip replacement surgery in elderly high-risk patients in a prospective randomized study and found that nerve block anesthesia was associated with fewer hemodynamic changes. 25 A randomized study compared postoperative delirium and postoperative cognitive dysfunction(POCD) in general anesthesia with lumbosacral plexus block group and general anesthesia group. It suggested that lumbosacral plexus block led to a lower incidence of postoperative delirium, POCD and earlier discharge readiness time in combination with intraoperative light sedation (high bispectral index). It showed no difference in complications within 30 days of surgery. This RCT included patients aged over 65 years old undergoing total hip arthroplasty investigated the influence of nerve blocks combined with general anesthesia. All patients in the 3 groups received intubation. 26 Our study as a retrospective evaluation, lumbosacral plexus plus T12 paravertebral nerve blocks without intubation were evaluated. The first RCT by Junfeng Zhang et al. investigating the effect of combined lumbar and sacral plexus block with sedation versus general anesthesia on long-term prognosis indicated that ultrasound-guided combined lumbar and sacral plexus block with sedation could be safely used in hip fracture surgery in elderly patients and can reduce the incidence of perioperative complications and improve long-term prognosis. 27 There are 2 different main points between our study and their trial. First, we jointly used T12 paravertebral block, thus providing better analgesia and reducing the sedation anesthetics for THA. Second, PSMA was used in our retrospective research to strengthen the results, and it is an after-randomization method.
The hip joint is associated with complex nerve innervation. THA is commonly performed under neuraxial or general anesthesia. Ultrasound guide plus nerve stimulator makes thorough nerve blocks possible for THA. 28,29 Compared to general anesthesia and neuraxial anesthesia, nerve blocks tampered less of physiology. Moreover, the complications related to extubation, emergence in PACU and catheter are avoided. Lumbosacral nerve block limited sympathectomy and bladder paralysis. The catheter can cause delirium in PACU, which is often observed in clinical settings. Furthermore, less sympathectomy stabilizes perioperative hemodynamics. Moreover, nerve blocks are related to better perioperative analgesia and less opioid. 30 Although it is a retrospective study, our research concentrated on the effect of nerve blocks without general anesthesia and provided robust evidence with PSMA.
Our study had several limitations. Firstly, it was retrospective research using propensity score-matched analysis to balance the baseline characteristics of the 2 anesthesia groups. It is more convincing evidence with RCT, but it is difficult to randomize the high-risk THA patients, and it is a challenging anesthesia technique requiring sophisticated anesthetists. Secondly, the number of NB cases is limited, and it has not the power to compare some of the parameters like 30-day mortality. Thus a well-designed RCT is required in future with a larger sample size.Thirdly, technical challenges associated with the placement of these blocks should not be discounted and they were great to our team in early stage. But all the members in our team have the technical experience over 3 years and are skillful with the techniques. Fourthly, the time to place multiple blocks is longer than GA and SA. 9
Footnotes
Authors Note
All authors reviewed the final version of the manuscript and approved it.
Authors’ Contributions
Data collection: LM, YY, YLY, BXX. Statistic Analysis: CC, ZLW, CDM. Drafting of manuscript: CC, SJ
Availability of Data and Material
Data and material can be acquired from the electronic database of our hospital.
Consent for Publication
We got consent for publication from patients and hospital.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
We got approval from the Ethics Committee of Changzhou First People’s Hospital, the third affiliated hospital of Soochow University and acquired the consent of reviewing the medical records of the patients
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Changzhou Health Commission[QN201925].