
Abstract
Aim
Hip fractures in older adults often result in decreased mobility and independence. This study aimed to identify critical balance skills that distinguish different activity levels following fracture, using sub-items of the Berg Balance Scale (BBS).
Methods
This retrospective cross-sectional study analyzed the medical records of 252 older adults (mean age 79.8 ± 8.8 years) with hip fractures. Participants were classified into Independent (n = 90), House-bound (n = 92), and Chair-bound (n = 70) groups based on the Japanese Bedriddenness Rank (BR). Decision tree analysis was performed using BBS sub-items as predictors of activity level.
Results
Key discriminators between activity levels were identified: “360° Turning” and “Sit to Stand” differentiated the Independent from the House-bound groups, while “Reaching Forward While Standing” and “Standing Unsupported” distinguished the House-bound from Chair-bound groups. Model accuracy was 81.9% (AUC 0.894) for Independent vs House-bound and 83.3% (AUC 0.910) for House-bound vs Chair-bound groups.
Discussion
Our results offer a novel, evidence-based approach to tailoring rehabilitation strategies for hip fracture patients. By focusing on these critical balance skills, patient functional outcomes may improve, ultimately enhancing quality of life in older adults following hip fracture.
Keywords
Introduction
Hip fractures represent a significant health concern for older adults, often leading to decreased mobility, loss of independence, and reduced quality of life. Rehabilitation following hip fracture is essential for restoring functional capacity and preventing further complications. A critical component of recovery is the ability to safely expand one’s range of activities, which heavily depends on balance capacity.
The Berg Balance Scale (BBS) 1 has emerged as a gold standard for assessing balance in older adults, especially after hip fracture.2-4 Comprising 14 functional tasks related to daily activities, the BBS provides a comprehensive evaluation of both static and dynamic postural control. While the total BBS score is widely used to predict fall risk5,6 and assess the need for assistive devices, 7 its individual sub-items may offer additional, underutilized insights that could guide more personalized rehabilitation strategies.8,9
In Japan, where population aging is among the most advanced worldwide, the Ministry of Health, Labour and Welfare utilizes the “Criteria for Determining the Level of Independence in Daily Living (Bedriddenness Level)” for older adults with disabilities, hereafter referred to as the Bedriddenness Rank (BR). 10 This unique index has demonstrated high correlation with internationally established measures such as the Barthel Index (BI) and Katz Index (KI). 11 The BR offers valuable insights into patients’ living environments, including their level of independence both indoors and outdoors, as well as their ability to safely participate in community activities. BR classifies patients into nine grades within five broader categories, with higher BR levels (eg, Normal, J1, J2) corresponding approximately to BI scores near full independence (median BI 95-100) and KI scores indicating independence (median KI 5-6). Conversely, lower BR grades (eg, B2–C2) align with severe dependence, reflected by low or zero KI scores. This mapping between BR and internationally recognized ADL scales facilitates the interpretation of BR scores beyond Japan, promoting cross-cultural understanding in geriatric assessments.
Despite widespread use of the BBS, there remains a notable gap in understanding how its sub-items relate to broader activity levels, especially outdoor mobility. Previous research has largely focused on indoor walking ability, often overlooking community reintegration—a crucial aspect for patients recovering from hip fractures.
This study aims to address this knowledge gap by examining the relationship between specific BBS sub-items and BR scores through decision tree analysis. We hypothesize that certain BBS sub-items will emerge as key predictors of functional activity levels, providing novel insights to tailor rehabilitation interventions. The findings are expected to contribute to the development of more individualized and efficient rehabilitation strategies, ultimately improving functional independence and quality of life among older adults following hip fracture.
Methods
Study Design and Participants
This retrospective cross-sectional study analyzed the medical records of older adults (aged >60 years) who were hospitalized and underwent rehabilitation for hip fractures at our institution in Japan between April 2015 and March 2023. Inclusion criteria were hip fractures resulting from falls in adults aged over 60 years. Exclusion criteria included (1) incomplete assessments, (2) refusal to participate during the opt-out period, and (3) classification as Bedriddenness Rank C.
Physical therapy was provided 5 to 6 times per week (20-60 min per session) by licensed therapists, following treatment plans developed in collaboration with orthopedic surgeons and rehabilitation physicians. Rehabilitation focused on gait, balance, and activities of daily living (ADL) and included muscle strengthening, range of motion exercises, balance training, walking practice, and stair climbing. The mean duration of rehabilitation was 34.2 ± 17.4 days, starting on average 2.2 days after injury or surgery and continuing until discharge.
This study was approved by the institutional ethics committee (Approval No. 24-304, 7070). As this was a retrospective study using anonymized data, written informed consent was waived. Instead, an opt-out notice explaining the study was publicly posted in the hospital to allow patients the opportunity to decline participation. All data were anonymized prior to analysis.
Measurements
The primary outcome was the participant’s level of independence in daily living, assessed using the BR, an official Japanese classification used to evaluate functional independence in both indoor and outdoor settings. BR levels J1 and J2 were classified as the “Independent” group; levels A1 and A2 as “House-bound”; and levels B1 and B2 as “Chair-bound.” This categorization allowed for stratified analysis of independence levels relevant to real-life recovery after hip fracture.
Secondary outcomes included the total score and sub-item scores of the BBS, a validated clinical tool for assessing balance performance, as well as additional functional measures such as BI for ADL function, the Ability for Basic Movement Scale (ABMS) 12 for motor function, and the Functional Ambulation Categories (FAC) 13 for walking ability. All outcome assessments were conducted by licensed physical therapists responsible for rehabilitation sessions from the postoperative period until hospital discharge.
Demographic data extracted included age, sex, days from injury or surgery to evaluation, and discharge destination. Fracture characteristics, including fracture site, laterality (left/right), and surgical procedure, were also recorded. Fracture sites were categorized as medial (neck fractures) or lateral (trochanteric fractures), and surgical methods included arthroplasty, osteosynthesis, conservative treatment, and others.
Degree of Independence for Daily Living: Japanese Bedridden Rank
The level of independence in daily life was evaluated using the Japanese BR, a functional classification system developed by Japan’s Ministry of Health, Labour and Welfare. 10 The BR is widely used in clinical and long-term care settings in Japan due to its practicality and relevance to real-world living situations. Although it is not widely known internationally, its validity and reliability have been supported by strong correlations with established ADL measures such as the BI.
The BR categorizes individuals into four levels—J (independent, able to go outside), A (independent at home but house-bound), B (chair-bound), and C (bed-bound)—each with two sublevels, resulting in eight subcategories. In this study, Rank C was excluded to focus on meaningful distinctions in activity range. Accordingly, BR levels J1 and J2 were classified as “Independent,” A1 and A2 as “House-bound,” and B1 and B2 as “Chair-bound.” This classification enabled investigation of the relationship between balance-related abilities and practical levels of activity and independence in daily life (Table 1).
Functional Balance: BBS
Balance function was assessed using the Berg Balance Scale (BBS), which consists of 14 functional tasks, each scored on a 5-point scale ranging from 0 (unable) to 4 (safe and independent). A licensed physical therapist administered each task with verbal instructions and scored the participant’s performance accordingly. The BBS is known for its high reliability and validity and does not require special equipment, making it a practical tool in older adult rehabilitation.14,15
Statistical Analyses
Missing data were handled by excluding cases with incomplete assessments from the main analysis (complete-case analysis). All subsequent statistical analyses, including the CART analysis, were performed on this complete dataset (n = 252). Sensitivity analysis using multiple imputation was performed beforehand, which showed no significant differences from the main results; therefore, the complete-case analysis results were used as the primary findings.
Participant characteristics were analyzed according to their BR-defined independence level (Independent, House-bound, Chair-bound). Age, BBS total score, BI, ABMS, and time to evaluation were compared using one-way analysis of variance (ANOVA) followed by Tukey’s post hoc test; categorical variables were compared using chi-squared tests. Receiver operating characteristic (ROC) curve analysis was used to evaluate the ability of BBS total scores to discriminate between adjacent independence levels (Independent vs House-bound and House-bound vs Chair-bound). Optimal cutoff scores were determined using Youden’s index. Diagnostic performance was evaluated using sensitivity, specificity, area under the curve (AUC), positive likelihood ratio (LR+), and negative likelihood ratio (LR−).
Bedriddenness Rank
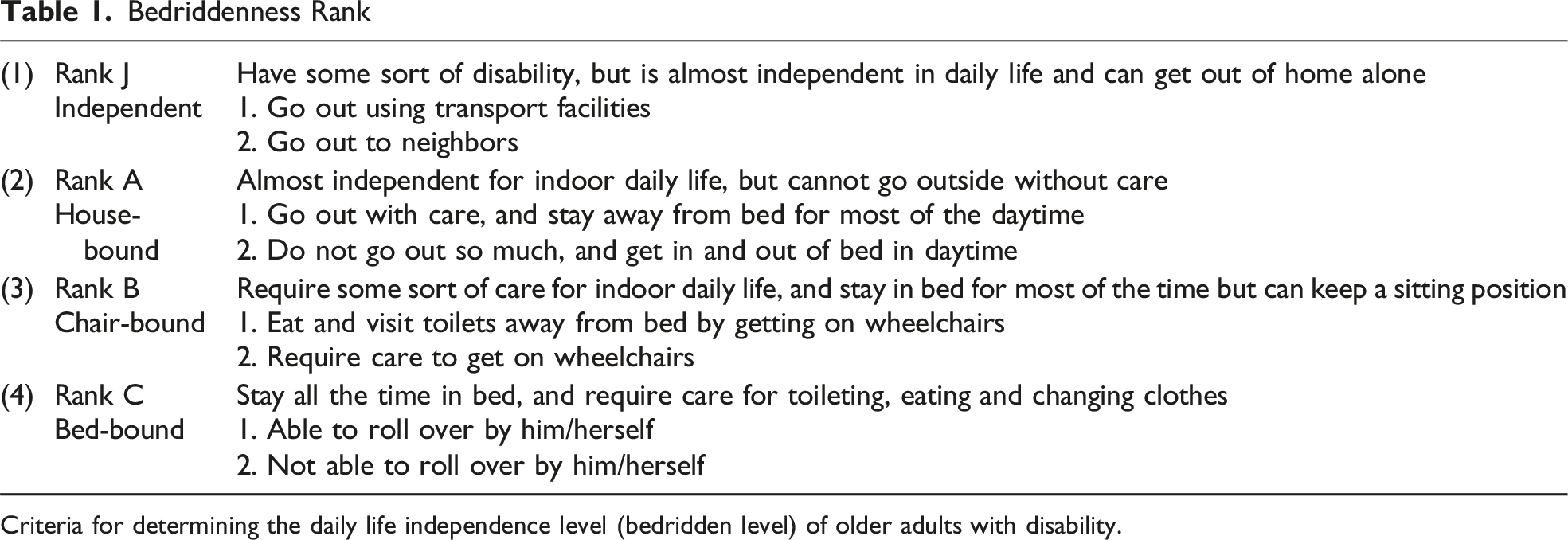
Criteria for determining the daily life independence level (bedridden level) of older adults with disability.
All statistical analyses were performed using JMP Pro software version 16.0 (SAS Institute Inc, Cary, NC, USA), with significance set at P < .05. This study was designed and reported in accordance with the STROBE guidelines.
Results
Participant Characteristics
Basic attributes including BBS, BR, FAC, and other relevant data were extracted from the outcome assessments. Twenty-four cases with missing data were excluded (Figure 1). After excluding 19 participants classified as Rank C, who required the most assistance with ADLs, the study included 252 participants categorized into Independent (n = 90), House-bound (n = 92), and Chair-bound (n = 70) groups. Participant characteristics are summarized in Table 2. The cohort comprised 193 women and 59 men, with a mean age of 79.8 ± 8.8 years. No significant differences were observed in sex distribution or fracture site among the groups; however, participants in the Independent group were significantly younger than those in the House-bound and Chair-bound groups. Data Flow Diagram Characteristics of the 252 Patients With Hip Fractures mean score + SD, [ ]: 95% confidence intervals (CI), η2 = eta squared, V = Cramér’s V, d = Cohen’s d. BBS, berg balance scale; BI, barthel index; ABMS, ability of basic movement scale; FAC, functional ambulation categories. aone-way ANOVA. bχ2 test. cYates χ2 test. dTukey test.

Comparison of BBS Scores According to BR
The mean BBS total scores (± standard deviation) were 49.7 ± 5.4 for the Independent group, 35.6 ± 11.1 for the House-bound group, and 12.0 ± 5.9 for the Chair-bound group, with significant differences between groups (Table 2). The optimal cutoff score for ‘outdoor independence’ was 42 points (sensitivity 86.7%, specificity 76.1%), while that for ‘indoor independence’ was 15 points (sensitivity 95.7%, specificity 68.6%).
Selection of Sub-items and Determination by CART Analysis
Figuress 2–1 illustrates differences in BBS sub-item scores between the Independent and House-bound groups. CART analysis identified “360° turning” as the strongest discriminator, with groups divided based on a score of 2 or higher—i.e., whether the task could be performed safely, even if it took more than 4 s. Among participants scoring ≥2 on “360° turning,” the subsequent discriminators were “Sit to stand” (scores of 4 vs 3 or less) in the second layer and “Stand to sit” (scores of 4 vs 3 or less) in the third layer, reflecting whether upper limb support was required. Additional discriminators included “Standing with eyes closed” in the fourth layer and “Placing alternate foot on a stool” in the fifth layer. Decision Tree Analysis Results for Discriminating Activity Level Groups. Figure 2 Presents the Decision Tree Analyses Used to Distinguish Between Activity Levels as Defined by BR. Each Node Shows BBS Sub-Item Used for the Split, the Cutoff Value, and the Sample Size (n) for that node. Figures 2–1 Shows the Decision Tree Used to Differentiate Between the Independent (Outdoor Independent) and House-Bound Groups. The Primary Discriminating Variables Are the Scores for “360° Turning” and “Sit to Stand.” the Model Achieved an Accuracy of 81.9% and an AUC of 0.894 for this Classification. Figures 2–2 Displays the Decision Tree Distinguishing Between the House-Bound and Chair-Bound Groups, With Key Splitting Variables Including BBS Sub-Items Such as “Reaching Forward While Standing.” the Model Achieved an Accuracy of 83.3% and an AUC of 0.910 for this Classification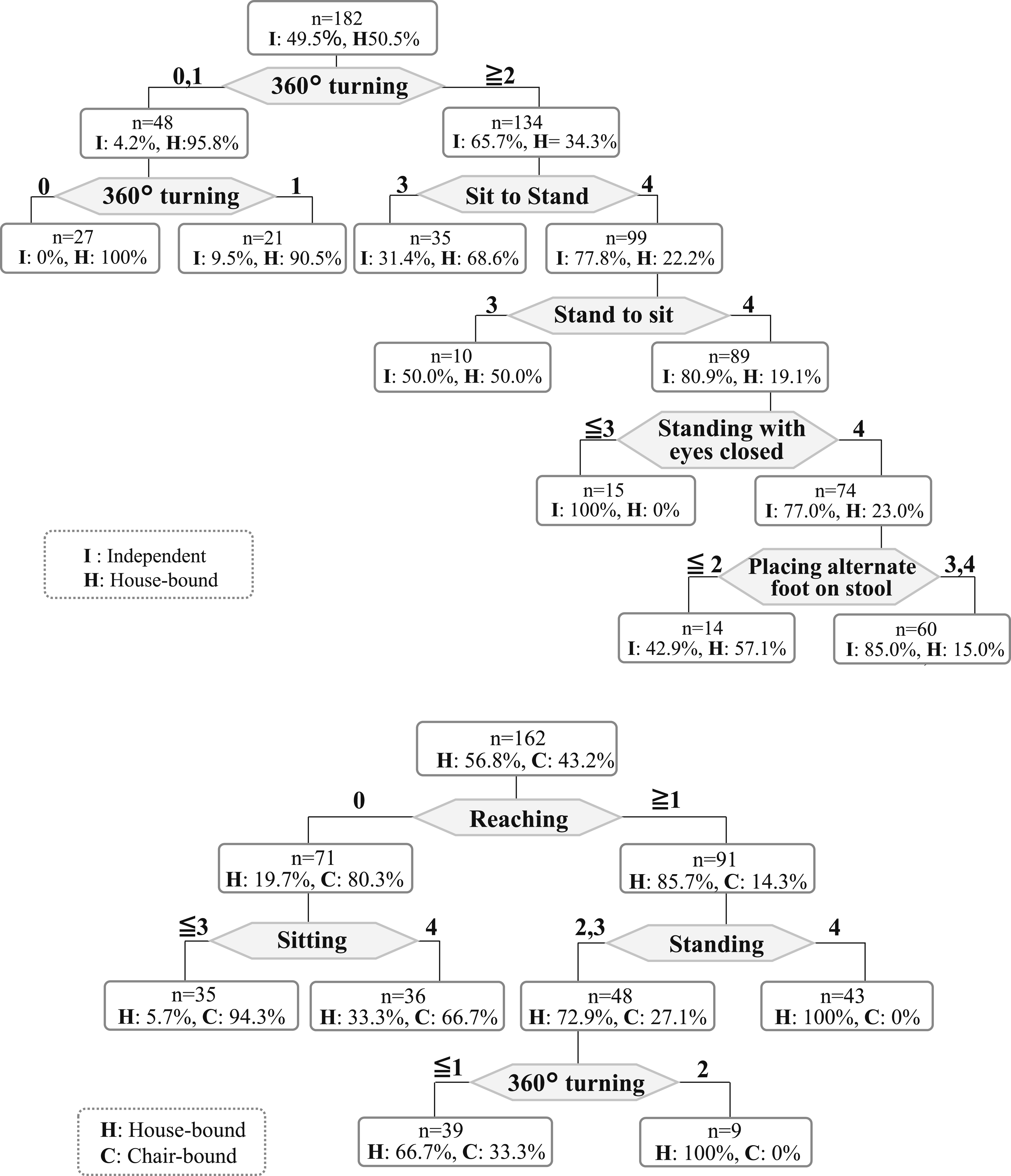
Figuress 2–2 shows differences in BBS sub-items between the House-bound and Chair-bound groups. For these groups, CART analysis selected “Reaching forward while standing” as the primary discriminator, with a cutoff at a score of 1 or higher—indicating whether assistance was needed. For participants scoring ≥1 on “Reaching forward while standing,” subsequent important variables were “Standing unsupported” and “360° turning.”
Effectiveness of the Decision Tree Analysis Model

LR+: Positive likelihood ratio, LR-: Negative likelihood ratio.
AUC, area under the curve of ROC curve; CI, confidence interval.
Discussion
A primary goal of rehabilitation after hip fracture is to restore pre-injury functional abilities. Balance ability is fundamental for expanding the range of activities and preventing falls. This study compared BBS scores with levels of independence in daily living and used decision tree analysis to identify the BBS sub-items most closely associated with activity range. To the best of our knowledge, this is the first study to examine the relationship between specific BBS sub-items and activity levels in patients recovering from hip fracture.
Critical Comparison of BBS Cutoff Values with International Standards
The cutoff values identified for outdoor and indoor independence were 42 and 15 points, respectively. While previous studies proposed BBS cutoffs of 45-50 points for fall risk screening among community-dwelling older adults,1,6,16 few studies have addressed cutoffs specifically for independence in indoor vs outdoor settings. Our findings provide contextually relevant thresholds that may serve as practical indicators for post-fracture living environments. The lower cutoff values observed in our study likely reflect the heterogeneity of patient environments and the use of assistive devices, which can reduce the physical demands required for independence in certain contexts.
Biomechanical and Functional Rationale for Key BBS Sub-items
During recovery after hip fracture, BBS sub-items such as “360° turning,” “sit to stand,” and “reaching forward while standing” play crucial roles in characterizing patients’ activity range and independence.
The “360° turning” task requires dynamic balance, whole-body coordination, rapid weight shifting, and the ability to change direction, all essential for safe ambulation in outdoor and complex environments. After hip fracture, patients frequently experience reduced support and proprioception in the affected limb; thus, independent performance of this movement indicates a higher level of functional recovery.
The “sit to stand” movement is complex, involving multiple muscle groups and the ability to shift the center of gravity. Patients often face challenges due to pain, weakness, and fear of loading the affected limb. Compensation strategies such as weight shift to the unaffected side or reliance on upper limbs suggest deficits in postural stability. Recent studies link reduced force in the affected limb during this task with slower recovery and greater dependence,17-19 highlighting the need for targeted rehabilitation.
“Reaching forward while standing” reflects anticipatory postural control and stability, directly related to safe daily activity performance and indoor independence.
Patients unable to perform these tasks have limited activity levels, whereas improvement is associated with higher independence.
Clinical Implications
This study identified specific balance tasks—sit-to-stand, 360° turning, and forward reaching while standing—as important factors associated with functional independence in older adults following hip fracture. These findings suggest that targeted training of these critical balance skills may be beneficial for improving activity levels and independence in rehabilitation settings.
Integration into Clinical Decision Support Systems
Our results offer a practical and focused approach to early rehabilitation screening and clinical decision support. By establishing clear cut-off scores for 360° Turning (distinguishing Independent from House-bound) and Reaching Forward While Standing (distinguishing House-bound from Chair-bound), these two critical sub-items can be integrated into a brief, high-yield early assessment tool. Clinicians can quickly administer only these tasks to stratify patients into preliminary activity level groups upon hospital admission or early post-operative stages.
Furthermore, the findings can be formalized into algorithmic clinical protocols or Electronic Health Record screening prompts. For example, a patient scoring below the identified threshold on 360° Turning can be automatically flagged by the system as having high risk of being House-bound, triggering a mandatory referral for advanced dynamic balance training. This shift from using the total BBS score to focusing on specific, actionable sub-items facilitates a more efficient and evidence-based allocation of limited rehabilitation resources.
Future Intervention Strategy
However, as this is an observational study, causal relationships between improvements in these tasks and functional outcomes cannot be confirmed. Therefore, future randomized controlled trials are required to clarify whether interventions that specifically focus on these balance tasks can significantly enhance activity range and independence. For example, repeated practice of sit-to-stand movements and interventions aimed at correcting weight-bearing asymmetry may be suitable approaches for enhancing this ability. Likewise, training that emphasizes weight shifting onto the affected limb and balance strengthening may be effective for improving 360-degree turning and forward reach tasks. Intervention studies are needed to investigate whether such targeted training leads to improved balance performance and, ultimately, to expanded activity levels and greater independence in this population.
International Validity of BR
BR is an official Japanese scale developed by the Ministry of Health, Labour and Welfare, widely used in healthcare and long-term care settings in Japan. Although it is not commonly used internationally, BR has demonstrated strong criterion-related validity with internationally recognized ADL measures such as BI and KI. Several studies have reported significant correlations between BR and BI/KI, indicating that BR assessments align well with international ADL standards. BR is also known for high inter-rater reliability and has been validated in multicenter studies across various healthcare settings. Therefore, while BR is a unique Japanese tool, it is both reliable and sufficiently comparable to international ADL measures, supporting the broader applicability of this study’s findings. Even in countries where the BR is not commonly used, translating it into practical activity levels such as “community ambulation capability” and “independent indoor living” allows for the application of the BBS cutoff values and sub-items identified in this study.
Limitations
This study has some limitations. First, since this was a single-center retrospective study, the generalizability of the results is limited.
The assessment of outdoor independence may vary considerably between urban and rural settings due to differences in environment, accessibility, infrastructure, and public transport availability. Therefore, the cutoff values obtained might not apply directly to other hospitals, regions, or healthcare systems.
Additionally, patient factors such as family support, caregiving arrangements, and community resources can differ by area and may affect functional outcomes. We did not fully adjust for potential confounders including age, sex, comorbidities, and cognitive function, which could influence rehabilitation results. Longer follow-up periods and comprehensive assessments of cognitive function and comorbidities would strengthen the evidence and improve generalizability.
The evaluation of independence was based on assessments conducted during hospitalization and may not fully represent patients’ abilities after discharge. Future research with prospective multicenter studies including larger and more diverse populations is needed to validate the findings.
Conclusion
This study identified specific balance skills (BBS sub-items) that characterize differences in activity levels among older adults after hip fracture. While declines in these balance skills were associated with functional outcomes, it remains unclear whether their improvement promotes functional recovery. Further research is needed to assess the effectiveness of interventions targeting these skills. Furthermore, the impact of factors such as comorbidities, cognitive function, and social support on independence was not fully evaluated, and additional investigation is warranted.
Footnotes
Acknowledgments
The authors would like to thank the hospital staff for their valuable assistance and insightful discussions regarding the data in this study.
Ethical Consideration
This study was approved by the Ethics Committee of the University (Approval No. 24-304, 7070) and was conducted in accordance with the Declaration of Helsinki.
Consent to participate
Because the study was retrospective and involved the use of previously collected clinical data, written informed consent was not obtained from individual participants. Instead, an opt-out document providing information about the study was posted in the hospital to offer patients the opportunity to decline participation. All data were anonymized prior to analysis to ensure patient confidentiality.
Author Contributions
H. Yoshida designed the study, the main conceptual ideas, and the outline of the proof, and collected the data; K. Higuchi and Y. Nakayama helped interpret the results and worked on the manuscript; M. Abo supervised the project; and H. Yoshida wrote the manuscript with the assistance of Y. Nakayama and K. Higuchi. All authors discussed the results and commented on the manuscript.
Funding
This work was supported by The Jikei University Research Fund for Graduate Students.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.