
Abstract
Background
Geriatric hip fracture patients often experience gaps in care including variability in the timing and the choice of an appropriate setting for rehabilitation following hip fracture surgery. Many guidelines recommend standardized processes, including timely access of no later than day 6 to rehabilitation services. A pathway for early identification, referral and access to geriatric rehabilitation post-hip fracture was created to facilitate the implementation. The study aimed to describe the barriers and enablers prior to the implementation of this pathway.
Methods
We conducted a qualitative descriptive study consisting of semi-structured interviews with geriatric hip fracture patients (n = 8), caregivers (n = 1), administrators (n = 12) and clinicians (n = 17) in 2 orthopaedics units and a geriatric rehabilitation service. Responses were analysed using a systematic approach, and overarching themes describing the barriers and enablers were identified.
Results
The clinicians’ and administrators’ top barriers to implementation of the pathway were competing demands (n = 24); lack of bed availability, community resources and funding (n = 19); and the need for extended hours and increased staff (n = 16). The top 3 enablers were clear communication with patients (n = 27), awareness of the benefits of geriatric rehabilitation (n = 24) and the need for education and resources to properly use the pathway (n = 15). Common barriers among patients and caregivers included lack of care coordination, overcoming some of their own specific challenges during their transition, gaps in the information they received before discharge, not knowing what questions to ask and lack of resources. Despite these barriers, patients were generally pleased with their transition from the hospital to geriatric rehabilitation.
Conclusion
We identified and described key barriers and enablers to early identification, referral and access to geriatric rehabilitation post-hip fracture. These influencing factors provide a basis for the development of a standardized pathway aimed at improving access to rehabilitative care for geriatric hip fracture patients.
Contributions to the Literature
This research identified and described implementation barriers and enablers specific to the referral process of post-operative hip fracture patients from acute care to subacute care. The barriers and enablers identified will help to improve referral rates to rehabilitation and help to reduce the acute care length of stay with the goal of helping hospitals meet best practice targets. A better understanding of these barriers and enablers can inform and optimize future implementation strategies so that they are better tailored to the local context and can also inform wider implementation.
Background
Hip fractures often represent sentinel events in the health trajectories of frail and chronically ill individuals, precipitating a steep functional decline and permanent disability. 1 In the United States, the cost of hip fracture care is estimated at more than US$5 billion annually across multiple sectors with most of the cost incurred in the post-acute care setting.2–5 As a result, the economic burden of geriatric patients with hip fractures causes significant and unnecessary strain on the health care system.
Many initiatives have been developed worldwide to improve patient outcomes and reduce cost.6–8 The American Geriatrics Society (AGS) and the International Geriatric Fracture Society (IGFS) have identified the best available evidence for post-acute care settings to improve the outcomes of geriatric hip fracture patients, as well as minimize complications. 9 In addition, many guidelines recommend all patients with hip fracture receive active rehabilitation following their acute care stay with rehabilitation beginning no later than 6 days following surgery.1,10–12
Nonetheless, geriatric hip fracture patients often experience gaps in care including variability in the timing and the choice of the appropriate setting for rehabilitation following hip fracture surgery. Inpatient geriatric rehabilitation is recommended as the gold standard for post-hip fracture care when striving to maximize functional recovery. 13 Geriatric rehabilitation involves a set of multidisciplinary interventions with the aim of restoring functional ability and enhancing residual functional capability in older adults with disabling impairments.14,15 Several studies have highlighted the diversity in post-acute care pathways that exist.16–18 According to Pitzul and colleagues, 16 there are pervasive variations in post-acute care delivery for geriatric hip fracture patients, especially with respect to access to rehabilitation. 16 In their study, the researchers identified over 49 unique post-acute care pathways taken by hip fracture patients to access rehabilitation. Results showed that the flow of hip fracture patients into geriatric rehabilitation is generally inconsistent. Furthermore, they concluded that a treatment model for geriatric hip fractures should emphasize the need to implement standardized plans of care, should work with all members of the health care team and should provide for continual quality improvement. 16
Research shows that timely access to rehabilitation services following hip fracture surgery results in better patient outcomes.19,20 Our institution currently faces substantial variations in referral rates to rehabilitation and also in acute care length of stay. Our current transition from acute to subacute care occurs at an average of 12.7 days which is above the recommendation of no later than 6 days post-surgery.
To address the complexities of the timely referral of hip fracture patients to geriatric rehabilitation, our research’s overall purpose was to develop and implement a theory-based intervention for an earlier discharge of the geriatric hip fracture population transitioning from acute care to subacute care. As such, the purpose of our study was to describe the barriers and enablers to early identification, referral and access to geriatric rehabilitation post-hip fracture.
Methods
Study Design and Setting
In this qualitative descriptive study, we conducted semi-structured interviews between 2018 and 2019, with geriatric hip fracture patients, informal caregivers, administrators and clinicians on 2 orthopaedics units in a large academic health sciences centre and on a geriatric rehabilitation service in an academic health care organization. The research ethics board’s approval was obtained.
Participant Eligibility
We used a purposive sampling technique to recruit clinicians involved at different stages of the referral pathway. This included any physicians (surgeons, geriatricians and internal medicine), nurses, physiotherapists, social workers, transition care coordinators and occupational therapists involved in the management of hip fracture patients either on the orthopaedics units or on the geriatric rehabilitation service. For the patients and informal caregivers, we used a convenience sampling method to recruit hip fracture patients (> 65 or older) and their informal caregivers (> 18 or older). Participants were recruited until saturation was obtained.
Data Collection
Clinicians’ Sample Interview Questions for Each of the 14 TDF Domains.

Sample Interview Questions for Patients and Informal Caregivers.

All participants provided signed informed consent prior to being interviewed. After providing consent, the research assistant conducted the digitally recorded 60-minute semi-structured interviews with the patients, the informal caregivers and the clinicians.
Data Analysis
For the clinicians’ interviews, the transcripts were analysed following a 6-step process as follows 24 : (1) 2 reviewers independently coded the transcripts using the TDF as a coding framework; (2) belief statements were developed for each quote, and then, similar statements were merged; (3) themes were generated from the merged belief statements, allowing similarities and differences to be recognized across the clinician groups; (4) themes were grouped into broader categories; (5) each theme was classified as a barrier or an enabler and (6) themes were examined in relation to whether they were shared (i.e. frequency of specific beliefs across interviews, presence of conflicting beliefs and perceived strength of the belief impacting the behaviour). A third researcher helped to resolve any disagreements. In order for a belief statement to be identified as a barrier or enabler, they had to be shared between at least 2 people or 2 provider groups.
For the patients’ and informal caregivers’ interviews, 2 researchers independently coded the transcribed interviews. The individual analyses were then collectively analysed by the team members for similarities between the transcripts using an iterative process until consensus on the coding and thematic analysis was reached. 25 NVivo qualitative data analysis software (QSR International Inc,) was used to support the analysis.
Role of the Funding Source
The funders played no role in the design, conduct or reporting of this study.
Results
Participant Characteristics
Participant Characteristics (n = 38).

aincludes physician assistant.
Clinicians’ Interviews (n = 29)
Barriers to the Implementation of Best Practices for the Management of Hip Fracture Patients Transitioning from Acute Care to Subacute Care (n = 19).
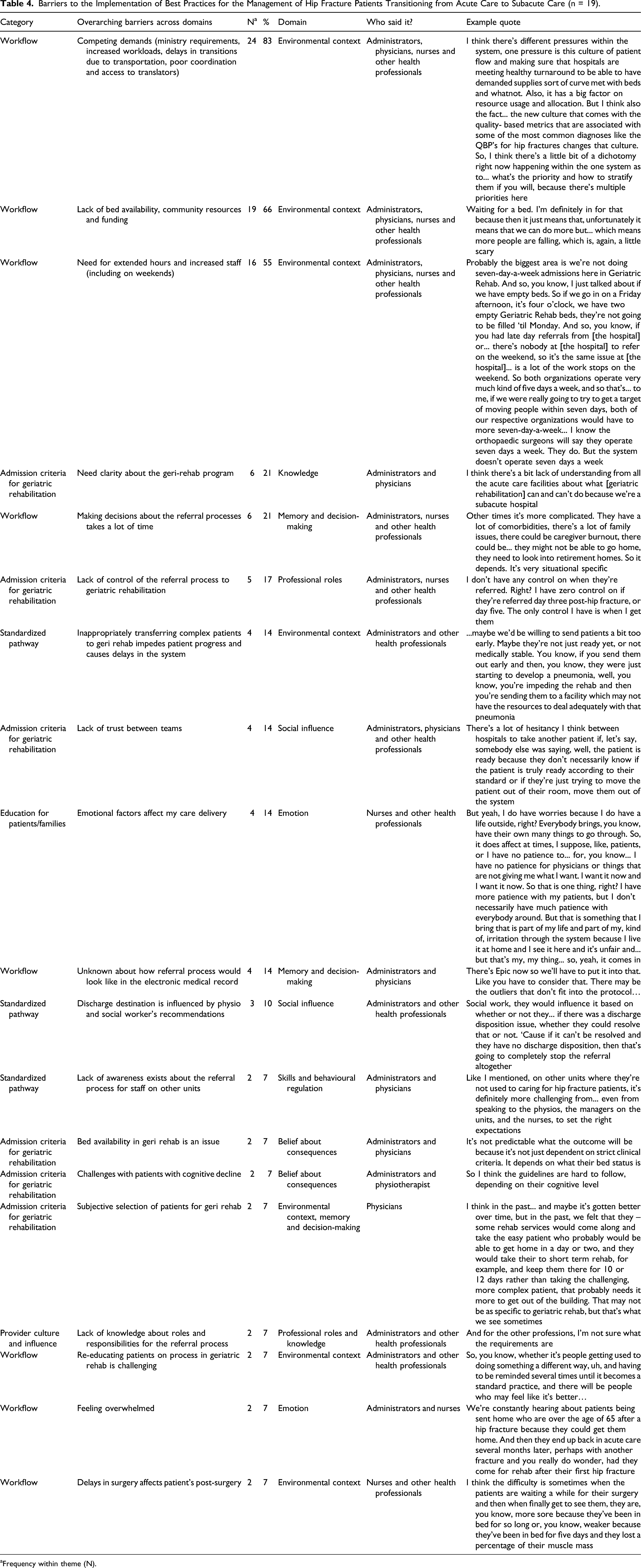
aFrequency within theme (N).
Enablers to the Implementation of Best Practices for the Management of Hip Fracture Patients Transitioning from Acute Care to Subacute Care (n = 17).
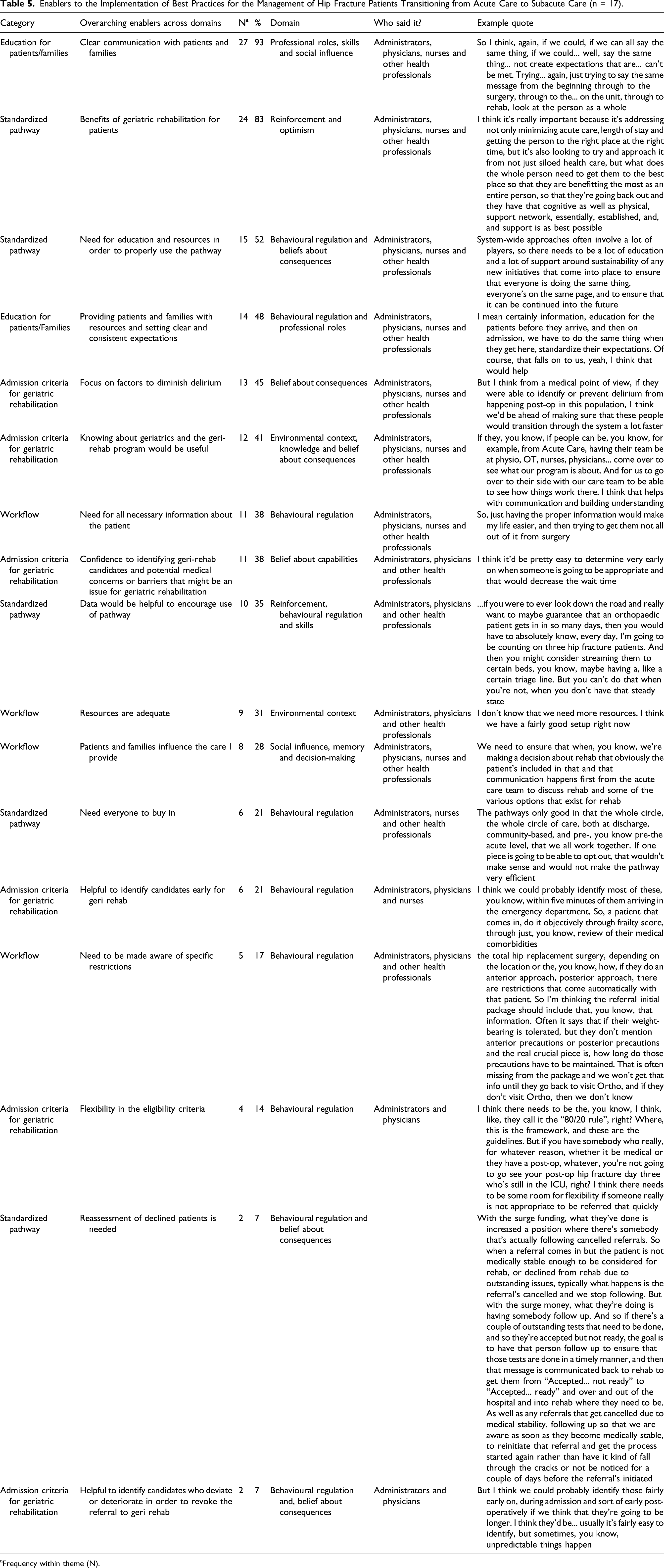
aFrequency within theme (N).
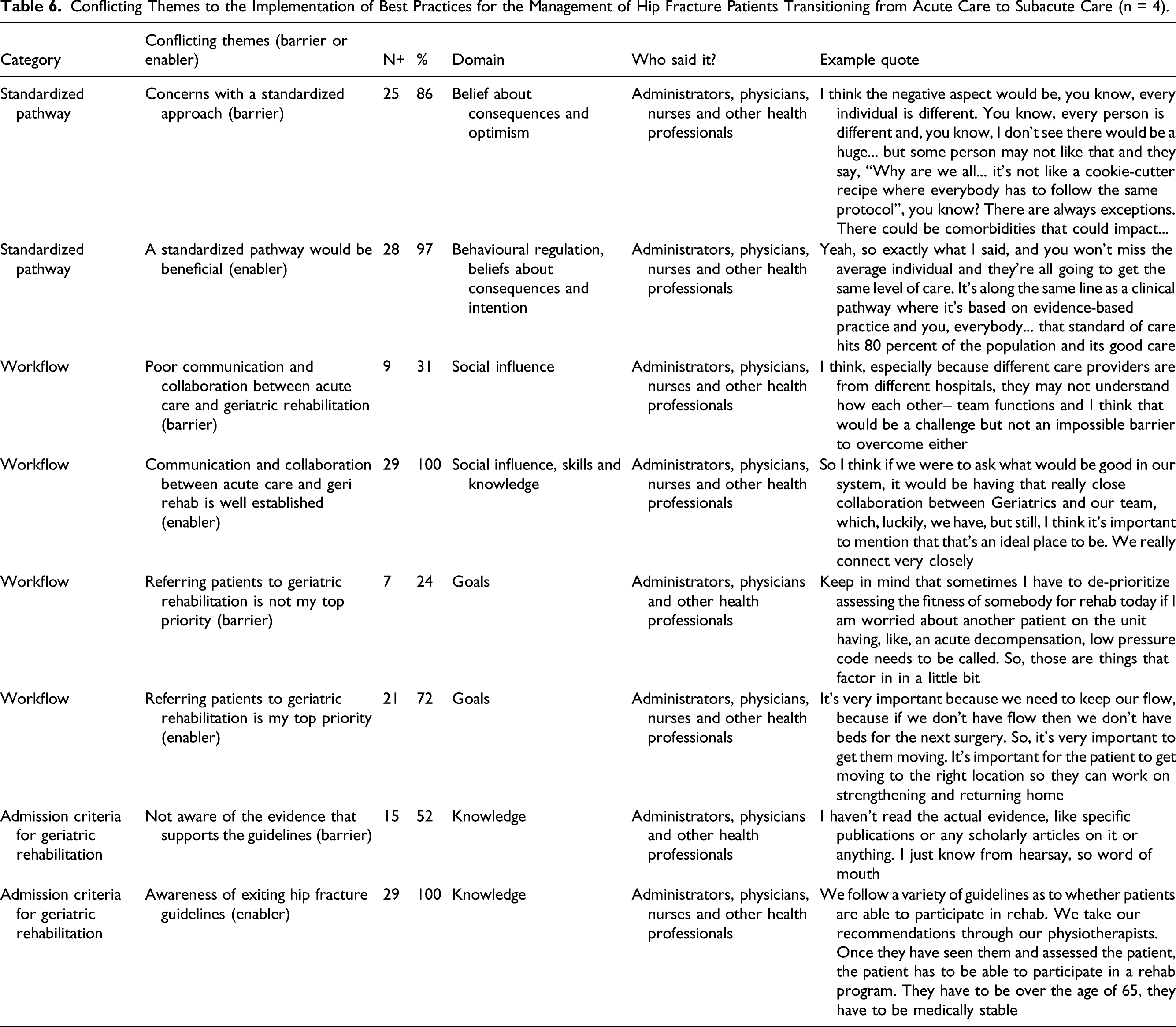
Conflicting Themes to the Implementation of Best Practices for the Management of Hip Fracture Patients Transitioning from Acute Care to Subacute Care (n = 4).
Barriers
Five categories of barriers were identified: (A) standardized pathway, (B) workflow, (C) admission criteria for geriatric rehabilitation, (D) education for patients/families and (E) provider culture and influence. The top 3 barriers were (1) competing demands (n = 24); (2) a lack of bed availability, community resources and funding (n = 19); and (3) the need for extended hours and increased staff (including on weekends) (n = 16).
Enablers
Four categories of enablers were identified: (A) workflow, (B) admission criteria for geriatric rehabilitation, (C) standardized pathway and (D) education for patients/families. The top 3 enablers were (1) clear communication with patients and families (n = 27), (2) awareness of the benefits of geriatric rehabilitation for patients (n = 24) and (3) the need for education and resources in order to properly use the pathway (n = 15).
Conflicting themes
Some themes (n = 4) were seen as both a barrier or an enabler depending on the interview. Some key informants had concerns with a standardized approach (barrier) (n = 25) and some thought a standardized approach would be beneficial (enabler) (n = 28). Some key informants felt it could be both a barrier and an enabler depending on the situation. All key informants felt that communication and collaboration between acute care and geriatric rehabilitation was well established (enabler) (n = 29), but some felt that poor communication and collaboration between acute care and geriatric rehabilitation was a concern in certain situations (barrier) (n = 9). There were conflicting views with respect to referring patients to geriatric rehabilitation as their top priority (enabler) (n = 21) or not referring patients to geriatric rehabilitation as their top priority (barrier) (n = 7). All key informants were aware of existing hip fracture guidelines (enabler) (n = 29); however, some key informants were not aware of the evidence that supported the guidelines (barrier) (n = 15).
Patients’ and Informal Caregivers’ Interviews (n = 9)
Barriers
Barriers Identified by the Patients and Informal Caregivers (n = 5).

Enablers
Despite these barriers, patients were generally pleased with the transition from orthopaedics to geriatric rehabilitation. A participant said: “One day I woke up, they said that before 11 o’clock somebody’s going to pick you up. So I sat in a chair, somebody fed me, medicated me, dressed me. I had only to wait... they even packed my things. When the stretcher came on, they just put me on the stretcher and my things underneath or some... on top of me... they drove me here. That was perfect.” (Patient #28).
Overall, the participants described the transition as being good and being pleased with the care received.
Discussion
Summary of the Findings
In this study, we used a behavioural theory approach to identify the barriers and enablers likely to influence the implementation of best practices for early identification, referral and access to geriatric rehabilitation post-hip fracture. This comprehensive and systematic approach identified barriers and enablers in the following categories: standardized pathway, workflow, admission criteria for geriatric rehabilitation, education for patients/families and provider culture/influence, all of which that have the potential to inform a future behaviour change intervention.
Barriers identified by clinicians and administrators were related to organizational and system factors such as competing demands for their time to perform other tasks or activities, a lack of bed availability, a lack of community resources, a lack of funding and the need for extended hours and increased staff including on weekends. Enablers were primarily related to patients’ and informal caregivers’ needs, and included items such as clear communication with patients and families, awareness of the benefits of geriatric rehabilitation and the need to receive adequate education and resources to properly use the pathway. Although, patients and informal caregivers were generally pleased with the transition from orthopaedics to geriatric rehabilitation, they too described some organizational level barriers such as a lack of care coordination between the orthopaedics units and the geriatric rehabilitation service, gaps in the information they received prior to discharge and a lack of equipment and staff resources. They also provided their personal experiences with their care transition with common themes including not knowing what questions to ask because of the lack of information provided and having to overcome some medical-related complications and delays during their transition.
Understanding these barriers and enablers will strongly support the future development of an evidence-based intervention to improve early identification, referral and access to geriatric rehabilitation post-hip fracture. The transition from acute to subacute care requires input from multiple team members, and consent from patients and/or families. The variety of responses elicited demonstrated the need for careful planning of any intervention in order to engage all stakeholders and to effect long-lasting change.
Comparison to Previous Research
Despite the ample evidence attesting to the benefits of geriatric rehabilitation programmes for post-hip fracture patients, our study reinforced the fact that a gap in knowledge exists regarding the barriers and enablers to better care transitions between acute and subacute care for geriatric hip fracture patients. This study also highlights the variation in practice for this population. The variation in practice impacts patients’ outcomes as well as overall health care delivery and costs. One systematic review demonstrated that inpatient rehabilitation specifically targeted at geriatric patients improved outcomes related to functional status and decreased mortality rates. 19 Other studies found that geriatric hip fracture programmes were associated with health and social service savings and were more effective than usual care in reducing length of stay,6,20,26 improving function 20 and increasing the rate of return to home after discharge.20,27
In a recent study, 28 the researchers reported that the main barrier to expedite patient discharge was arranging the appropriate placement for patients requiring long-term advanced care with home health nursing or inpatient nursing facilities. In another study, researchers examined the impact of an earlier transfer of hip fracture patients to rehabilitation for ten partnerships between acute care and rehabilitation. 29 Their results showed that only 2 of the partnerships were able to achieve the target reduction in length of stay, indicating that these care transitions are complex events. 29 The barriers to earlier transfer to geriatric rehabilitation are similar to the ones in our study. They include contradictory opinions regarding patients’ eligibility for rehabilitation, inefficient hospital system processes and hospital pressures (i.e. occupancy). The study also supports the need for a high degree of collaboration between acute and subacute care to realize change. 29
Based on the results of our study, we have designed an evidence-based intervention for early identification, referral and access to geriatric rehabilitation post-hip fracture. The pathway will enable all patients if they meet the defined eligibility criteria for geriatric rehabilitation to be accepted and transferred from acute care to subacute care no later than post-op day 6. 1 The implementation of this pathway is guided by our barriers and enablers analysis. Specifically, we selected the evidence-based behaviour change techniques (BCTs) 23 that address these barriers and enablers. These selected BCTs include the development of key flags in the clinical pathway, standardized transfer of information between acute and subacute care, high-risk delirium screening and dashboards to provide immediate feedback to clinicians, patient information materials, multidisciplinary workshops, reminders and sustained engagement. We have combined these BCTs into a deliverable intervention that will be evaluated in a future trial for feasibility and acceptability.
Strengths and Limitations
There are strengths and limitations to our study. We used a theoretical framework to guide our data collection and analysis. This study also included a large variety of clinicians and administrators to get a better insight on the barriers and enablers to the referral to geriatric rehabilitation post-hip fracture. Although we interviewed a total of 38 participants consisting of clinicians, administrators, patients and informal caregivers, it is possible that the participants’ views differ from those who did not participate. However, we did obtain some very important information on what might be the barriers and the enablers to the development and the implementation of the intervention.
Conclusion
This study identified key barriers and enablers to early identification, referral and access to geriatric rehabilitation post-hip fracture. A better understanding of these barriers and enablers can inform and optimize future implementation strategies so that they are better tailored to the local context and can also inform wider implementation. Overall, addressing these barriers pre-implementation may improve the integration of the standardized pathway into practice.
Footnotes
Acknowledgement
We would like to thank all the clinicians, patients and informal caregivers who participated in our study.
Authors’ contributions
All authors (CB, AH, SP, VFM, PEB, SP, JD and JES) contributed to conceptualizing and designing the study. CB drafted the manuscript. All authors (CB, AH, SP, VFM, PEB, SP, JD and JES) critically appraised and edited the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Ottawa Hospital Academic Medical Organization Innovation Fund and the Bruyere Academic Medical Organization Incentive Fund.
Ethics approval
Approval was obtained from the Ottawa Health Science Network Research Ethics Board (#20180469-01H), the Bruyere Continuing Care Research Ethics Board (#M16-18-03) and the University of Ottawa Health Sciences and Sciences Research Ethics Board (#H-08-18-1061).