
Abstract
Background
Despite advances in surgical care, disparities in functional recovery and mortality following hip fracture directly relate to racial, ethnic, and economic factors. Without a comprehensive method to model patients’ diverse socioeconomic factors, researchers rely on proxies such as race and insurance status. The Distressed Community Index (DCI) score is a validated means of holistically estimating a patient’s socioeconomic status, incorporating variables including community median income, unemployment, housing vacancies, education, business growth, and poverty rates.
Methods
The 2012-2014 100% Medicare Standard Analytical Files was queried, identifying patients surgically treated for isolated hip fractures. Individual socio-economic status was determined by linking residential ZIP codes with the DCI score. The study cohort was divided into 5 distinct tiers based on the DCI score: [0-20] (prosperous), [21-40] (comfortable), [41-60] (mid-tier), [61-80] (at risk), and >80 (distressed). Multi-variate logistic regression analyses were used to assess the impact of increasing DCI score on 90-day complications, readmissions, and mortality.
Results
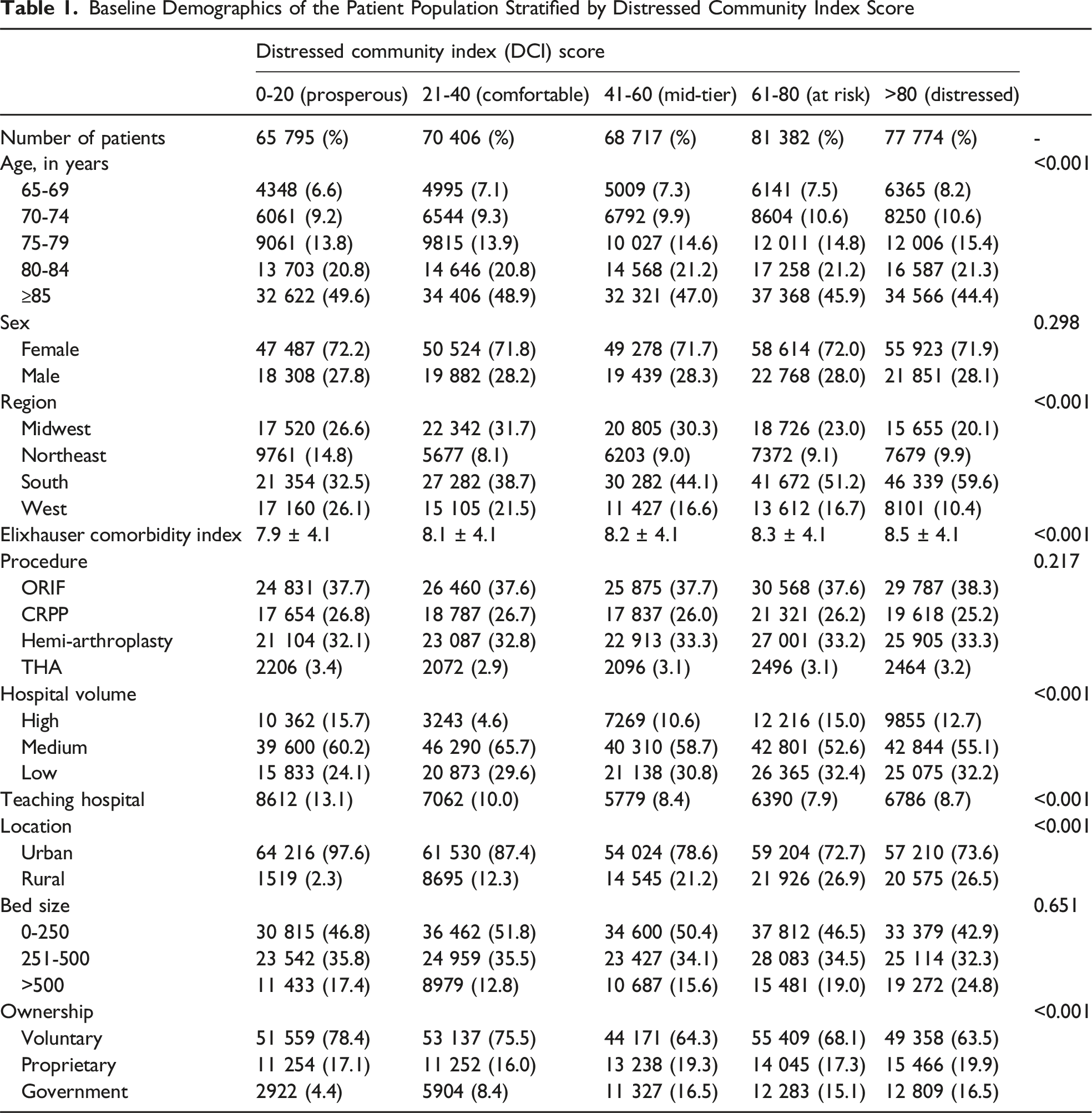
A total of 364 074 patients met inclusion criteria. Patients with lower DCI scores were more likely to receive care at teaching hospitals (13.1%) in urban settings (97.6%) than the Distressed tier (8.7% and 73.6%, respectively). The distressed group was at a significantly higher risk of urinary tract infections (OR 1.12; P < 0.001), pneumonia (OR 1.18; P < 0.001), and pressure ulcers (OR 1.09; P < 0.001). Patients in the distressed group were more likely to have emergency department visits (OR 1.12; P < 0.001) and had higher odds of mortality (OR 1.14; P < 0.001). With elevated DCI score there were lower rates of readmission (OR 0.91-0.95; P < 0.001) but this was not significant in the DCI >80 group.
Conclusions
Patients living in ZIP codes with high DCI score had higher risks of post-operative complications, including death, after hip fracture surgery. Integration of the DCI score into clinical practice may help to mitigate adverse outcomes in this vulnerable patient population.
Introduction
With an estimated incidence of 150 000 hip fractures a year 1 and a 30% 1-year mortality rate, 2 hip fractures remain a significant public health burden in the United States. Post-operative mortality has been associated with clinical comorbidities 3 and increased time-to-surgery. 4 However, despite the advances in surgical and clinical care, disparities in orthopedic surgical outcomes have been observed on racial, 5 ethnic, 6 and economic7,8 bases. Functional recovery and mortality following hip fracture are influenced by social support,9-11 education, 12 income, 13 and employment status.12,14
Social factors that impact care for patients are important but often overlooked. The adoption of value-based care models has placed a greater responsibility on health care systems to maximize the value of care.15,16 This shift towards value-based care has encouraged greater awareness of the socioeconomic factors influencing patient outcomes and cost of care. Interventions, such as the establishment of Critical Access Hospitals, 17 have expanded access to quality orthopedic surgical care in underserved communities.
In order to design novel interventions that address this inequity in hip fracture outcomes, we must better characterize the biopsychosocial risks. Without a comprehensive method to model the diverse socioeconomic variables, researchers have used proxies. However, analyses based on insurance status, 18 education level, 5 income, 19 and race 19 incompletely tell the story. A person’s place on the socioeconomic scale is multi-faceted and includes variables ranging from a person’s place of residence to their community employment rates. Despite a growing interest in identifying disparities in hip fracture care, current evidence is limited by the availability of comprehensive national, community-level socioeconomic data. The Distressed Community Index (DCI) holistically estimates a patient’s socioeconomic status (SES) and models variables including community median income, unemployment, housing vacancies, education, business growth, changes in employment and poverty rates. These scores are normally distributed and range from 0 (prosperous) to 100 (distressed).
The DCI is a well validated tool (21-24) to evaluate the biopsychosocial variables on surgical outcomes however, there have been no studies correlating DCI score to hip fractures. The purpose of this study was to describe the relationship between the Distressed Community Index Score and 90-day outcomes following hip fracture surgery. Although the interaction of sociodemographic factors is complex, identifying and characterizing these risk factors may lead to novel interventions to improve outcomes.
Methods
The 2012-2014 100% Medicare Standard Analytical Files (SAF100) was used to identify patients who underwent treatment for a hip fracture from 2012-2014. Patients were included who were ≥65 years-old and underwent open reduction/internal fixation (ORIF), percutaneous pinning, hemiarthroplasty or total hip arthroplasty (THA) for isolated closed hip fractures. Exclusion criteria were patients under the age of 65 and those who didn’t receive the previously mentioned procedures. Of the excluded patients 42% were <65 years old. Compared to included patients there was slightly higher proportion of males (33% vs 28%), patients from the northeast (42% vs 10%) and lower Elixhauser Comorbidity Index scores (8.0 vs 8.2) within the excluded population. Due to the change in 2015 from ICD9 to ICD-10 coding, the timeframe of 2012-2014 was selected. ICD-9 procedure codes included ORIF (P-7935, P-7855}, hemiarthroplasty (P-8152), total hip arthroplasty (P-8151) and Percutaneous pinning (P-7915).
Medicare Standard Analytical Files were utilized for standard 90-day post operative outcomes using ICD-9 codes which included urinary tract infections, pneumonia, pressure ulcers, surgical site infection, deep vein thrombosis, pulmonary embolism, clostridium difficile infection, sepsis, acute kidney injury, emergency department visits, readmission and death. The study based on institutional protocol didn’t meet the need for IRB approval due to data de-identification. This study was reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.
Socio-economic status of individuals was determined by linking the residential ZIP code with the nationally validated Distressed Community Index (DCI) score. Developed by the Economic Innovation Group, the DCI is based on quantitative measurements derived from both the U.S. Census Bureau’s Business Patterns and American Community Survey 5-Year Estimates for the 2014-2018 period. 20 It covers nearly 25 500 zip codes and 99 percent of the U.S. population. Each score is an equally weighted average of 7 component metrics within a given ZIP code: community unemployment, educational attainment, housing vacancies, poverty rate, median income, business growth, and the change in business establishments. The final score is normally distributed, and ranges from 0 (prosperous) to 100 (distressed). The study cohort was divided into 5 distinct tiers, based on the DCI score in concordance with other published analyses: 0 to 20 (prosperous), 21 to 40 (comfortable), 41 to 60 (mid-tier), 61 to 80 (at risk), and >80 (distressed).21,22
Analyses were performed using R Analytics version 4.0.2 with P-values calculated using two-sided ANOVA and Chi Squared analysis for continuous and categorical variables respectively. Unadjusted odds ratios for all the outcomes were determined using univariate logistic regression. Afterwards, adjusted odds ratio were determined using multivariable logistic regression analyses were used to assess the impact of increasing DCI score on 90-day complications, readmissions, and mortality. To adjust for confounding variables, multivariate regressions were controlled for baseline demographics (age, gender, region, co-morbidity burden), type of procedure (ORIF, THA, hemiarthroplasty and percutaneous pinning), and hospital-level characteristics (teaching status, case volume, ownership, location, bed size). P < 0.05 was considered significant and odds ratios (OR) were presented for analysis. Both an overall composite outcome was calculated for each DCI tier which was defined as occurrence of any of the 9 complications as well as a subgroup analysis for each individual outcome. Our hypothesis was that patients with increasing levels of socioeconomic distress would experience a greater burden of post operative complications.
Results
A total of 429 106 patients experienced closed isolated hip fractures from 2012-2014, of which 364 074 patients met inclusion criteria. Patients were assigned into one of the 5 tiers of community descriptors, based on the average values for the seven-component metrics of the DCI (Figure 1). Community groups were established by DCI score as 0-20 (prosperous), 21-40 (comfortable), 41-60 (mid-tier), 61-80 (at risk), and >80 (distressed). There were 65 795 (18.1%) patients in the Prosperous tier, the Comfortable tier had 70 406 (19.3%) patients, Mid-tier included 68 717 (18.9%) patients, At-risk included 81 382 (22.4%) with a DCI score of 61-80, and there were 77 774 (21.4%) in the Distressed tier. Distribution of Patient Cohort by DCI Tier. DCI: Distressed Community Index
Baseline Demographics of the Patient Population Stratified by Distressed Community Index Score
Adjusted Composite 90-Day Outcomes by Distressed Community Index Tier

Sub-group Analysis for 90-Day Outcomes by DCI Tier

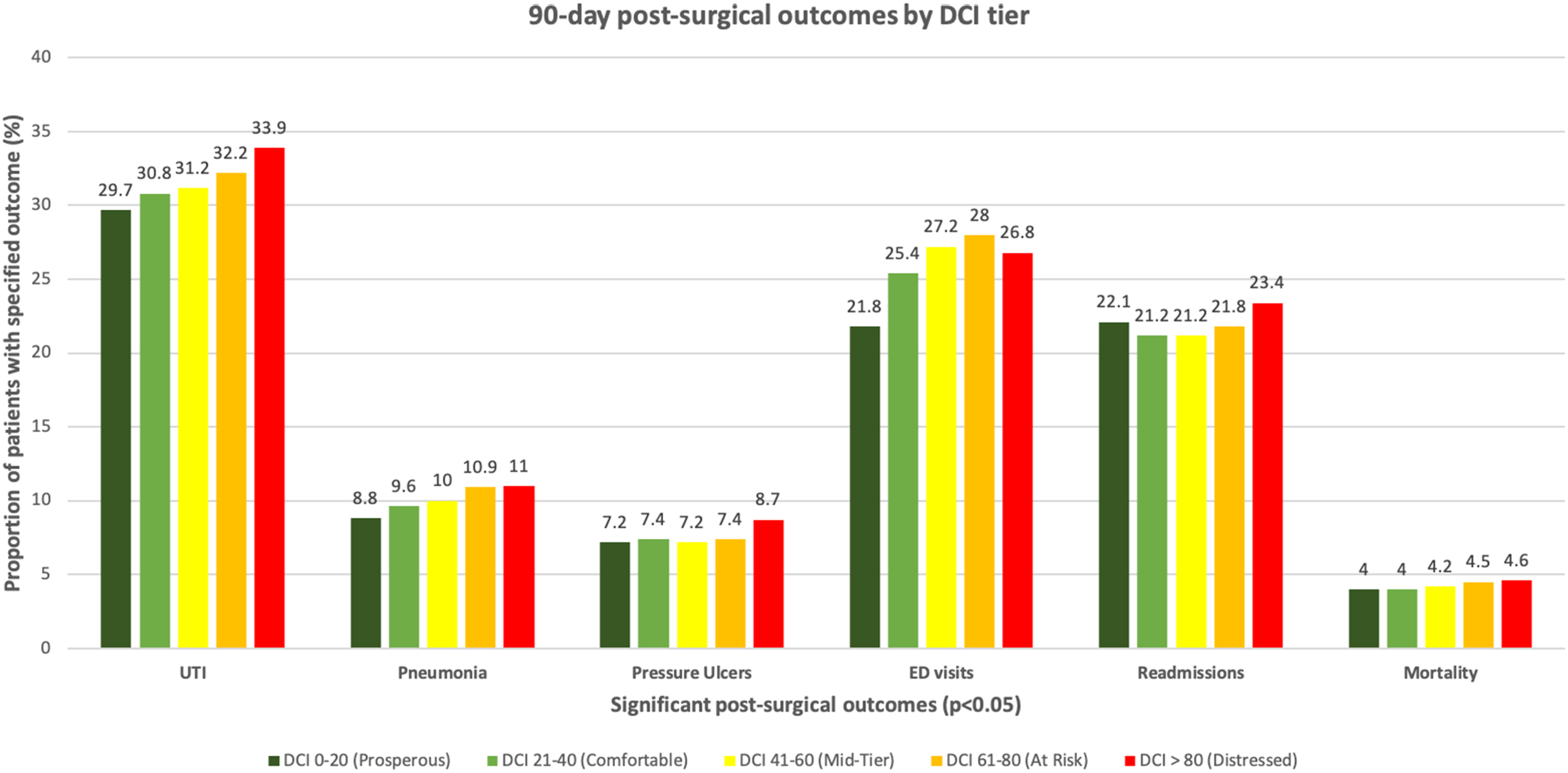
Trends in Statistically Significant (P < 0.05) Post-surgical Outcomes by DCI tier. ED: Emergency Department; DCI: Distressed Community Index; UTI: Urinary Tract Infection
Discussion
Within the first year of injury, hip fracture patients have a mortality rate 3-times their age-matched cohort. 23 Current literature has suggested that outcomes following hip fracture surgery is impacted by SES. 24 However, utilization of individual variables, such as race, as a proxy for SES results in the suppression of unmeasured structural variables. 25 New models, such as the DCI score, better characterize SES by summarizing components of social status and improve prediction of surgical outcomes. This study sought to describe the relationship between the validated DCI model for estimating SES and hip fracture outcomes using a nationally representative Medicare database. The results of this study demonstrate that patients are at a higher risk of experiencing post-surgical outcomes, including mortality, based on their zip-code and community characteristics (Figure 2).
To our knowledge, this is the first analysis of hip fracture post-surgical outcomes with this new model of estimating SES. The strengths of our study include the use of a nationally representative Medicare dataset along with a SES model that maps 99% of zip codes in the nation. This reach supports the generalizability of these results. This study, however, is not without limitations both from our dataset and in our methodology. The first dataset limitation is that this dataset did not included patient-reported outcomes such as patient satisfaction, return-to-work, lost wages, and activities of daily living. This information would offer a deeper understanding on patient complications and outcomes. Additionally, the dataset does not code for nuances such as type of fracture. Some fracture patterns, such as high-velocity traumatic fractures may be more prevalent in certain DCI communities and ultimately influence these outcomes.
Methodological limitations that we must consider include the inherent difficulty that comes with attempting to identify variables to model for SES. One can argue that the 7 selected variables that are modeled in the DCI are not extensive enough to capture a patient’s SES; however, the DCI model has been validated in previous general surgical outcome studies.26-28 Additionally, our patient cohort was selected from Medicare Standard Analytical Files from 2012-2014 however our DCI scores were calculated from Census Bureau Data from 2014 to 2018 which limits the consistency of the socioeconomic application. Key factors, such as a patient’s transportation distance or distance from a trauma center may influence delays in presentation and thus sequelae from post-operative complications. 29 Each zip-code community may have differences in the availability of ancillary services, such as rehab facilities, which could not be captured with our dataset. The DCI score although useful to determine a population based distress level cannot be uniformly applied to each member within that population which is a limit to generalizability.
Our findings suggest that patients with a high DCI score may face barriers in access to care, illustrated by the fact that they were more likely to visit the emergency room and more likely to die after hip fracture surgery. For the Comfortable, Mid-Tier and At Risk populations the readmission odds were significantly lower while the distressed group showed no difference from the prosperous group. We suspect the patients with the greatest level of distress have the highest rates of mortality and thus may not be captured as a readmission if their out of hospital mortality rate is higher within the population. Additionally, patients in the distressed group (DCI>80) had lower odds of DVT (OR 0.84; P = 0.003) and PE (OR 0.89; P < 0.001). This may be explained by barriers to diagnosis such as limited utilization of advanced imaging, challenges with transportation to centers with trained ultrasound technologists. Further examination of these findings would be critical for future study.
Our study also demonstrated significantly higher risk of pressure ulcers in the distressed group compared with the prosperous group with an OR of 1.09. There is literature to support a greater risk of pressure ulcer development with lower patient education levels and lower household income in the orthopedic and acute care populations and we demonstrated a similar relationship based on DCI.30,31 Although discharge location and mobility status of post-surgical patients based on DCI score was not directly addressed in this study, we believe future analytic and quality improvement studies could uncover and address this potential disparity.
Personalizing interventions by DCI tier has the potential to mitigate the risks of adverse outcomes in vulnerable patient populations. In fact, integrating DCI status with the American College of Surgeons National Surgery Quality Improvement Program (ACS NSQIP), a risk-adjusted outcome model, improved the prediction of outcomes and hospital costs. 32 For example, a study evaluating mobility patterns among patients of differing DCI could result in a targeted intervention to reduce pressure ulcers. These critical questions are rooted in the diversity and background of patients within each community, serving as open invitations for the healthcare system to contribute to change. After the identification of modifiable risk factors for patients experiencing higher levels of distress, orthopaedic surgeons and support staff can assemble quality improvement projects to address a specific topic of interest.
Conclusions
Among the 364 071 patients in this nationally representative dataset, patients living in zip codes corresponding with high DCI score were at higher risk of post-operative complications, including death, after hip fracture surgery. The DCI score incorporates 7 holistic components of community distress in an effort to more accurately estimate a patient’s SES. Collecting and integrating DCI score into clinical practice is a comprehensive method to highlight the risks of adverse outcomes in vulnerable patient populations.
Footnotes
Acknowledgements
The authors wish to acknowledge Jessica Wiseman, senior research coordinator at the Ohio State Wexner Medical Center for her contributions to the manuscript. Additionally we would like to thank Muhammad Talal Ibrahim a research fellow at The Ohio State Medical Center for his statistical work in the revision process.
Ethical Considerations
Due to the retrospective nature of the study including deidentified Medicare data, ethical approval was not required per institutional protocol at the Ohio State University Wexner Medical Center.
Author Contributions
Methodology, Formal Analysis, Investigation, Writing Original Draft Preparation was completed, by Mitchell Gray, Janice Bonsu, Azeem Malik, Carmen Quatmen. Methodology was completed by Thuan Ly, Laura Phieffer, Ryan Harrison and Safdar Khan. Writing Review and Editing was completed by all authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by National Institute on Aging under the Grants for Early Medical/Surgical Specialists' Transition to Aging Research GEMSSTAR (Grants for Early Medical and Surgical Supecialists' Transition to Aging Research) Grant (R03AG060177); The National Institute on Aging under the Paul B. Beeson Emerging Leaders Career Development award in Aging (K76AG068435); and the Orthopedic Research and Education Foundation Career Development Award.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.