
Abstract
Objectives
To explore the impact of race, language, and socioeconomic status on vitamin D screening and osteoporosis treatment after operative management of proximal femur fractures.
Methods
Design: Retrospective cohort. Setting: Level I, II, and III Trauma Centers within an overarching institutional organization. Patient Selection Criteria: Patients greater than 65 years of age who underwent operative treatment for a proximal femur fracture between January 2020 and June 2023. Outcome Measures and Comparisons: Primary outcomes were rates of vitamin D screening and osteoporosis treatment. Secondary outcomes were rates of geriatric and endocrinology consultation during admission. Primary and secondary outcomes were compared by race, language, and socioeconomic status (Area of Deprivation Index [ADI]). ADI was recorded at the state level (0 to 10) using the ADI mapping tool with higher ADI indicating more socioeconomic disadvantage.
Results
In total, 1149 patients were included (primary English-speaking: 89.2%, White: 90.3%, with intertrochanteric hip fractures: 76.6%). There were no differences in vitamin D screening or osteoporosis treatment observed between racial, language, or socioeconomic groups (P > 0.05)
Conclusions
Black patients or those from higher area of deprivation neighborhoods were less likely to receive endocrine consults. Geriatric and endocrine consults increased the odds of obtaining vitamin D screening and osteoporosis treatment. Despite this finding, race, language, and socioeconomic status did not impact vitamin D screening or osteoporosis treatment after proximal femur fracture. The discrepancies in consultation based on non-clinical factors emphasize the importance of interdepartmental collaboration to optimize standardized osteoporosis treatment after proximal femur fracture and highlight disparities in osteoporosis care.
Level of Evidence
Therapeutic Level III.
Introduction
As the most common metabolic bone disease, osteoporosis poses significant health concerns among elderly patients.1-3 Osteoporosis is characterized by decreased bone mineral density and contributes to proximal femur fractures, leading to severe morbidity, prolonged hospital stays, and high mortality rates.1-3 Effective management consists of antiresorptive, anabolic, and bisphosphonate agents in combination with lifestyle modifications.1,4,5 Despite advances in pharmaceutics and diagnostic modalities, a subset of patients remain disproportionately affected by osteoporosis.6,7 Differences in screening, diagnosis, and treatment have been reported, particularly among racial, linguistic, and socioeconomic groups, however, explanations for such disparities remain heterogenous.8-10 Understanding factors that influence management and outcomes of osteoporotic proximal femur fractures warrants further investigation.
In orthopedics, there is increasing recognition of how socioeconomic factors—such as race and ethnicity, language, residential area, and education—are linked to higher rates of orthopedic trauma and worse surgical outcomes.11-13 Previous literature has identified socioeconomic factors as a barrier to initiation of osteoporosis treatment and an important contributor to the likelihood of receiving timely and appropriate care for hip fracture patients. 14 Socioeconomic status, often assessed through metrics such as the Area Deprivation Index (ADI), result in worse medical outcomes, longer hospitalization, and higher readmission rates.15-17 Furthermore, race has been shown to influence the care of osteoporotic patients, with Black patients disproportionately affected and less likely to receive necessary diagnosis and treatments.8,18,19 Linguistic barriers have also been shown to impair care delivery to patients with osteoporosis. 14 Given the intersection of these factors, it is imperative to explore how race, language, and socioeconomic status influence vitamin D screening and osteoporosis treatment after hip fractures.
Therefore, the primary aim of this study was to examine the impact of sociodemographic factors on vitamin D screening and osteoporosis treatment in a large cohort of geriatric proximal femur fractures. The secondary objective was to compare the impact of sociodemographic variables on the likelihood of geriatric and endocrine consultation.
Methods
Patient Selection
After institutional review board approval, adult patients with proximal femur fractures treated between January 2020 and June 2023 were identified from an institutional research patient data registry of Level I, II, and III Trauma Centers within an overarching institutional organization using Current Procedural Terminology codes 27 236, 27 244, 27 245, 27 230, and 27 235. Patients were included if greater than 65 years and underwent an operatively treated proximal femur fracture. Exclusion criteria included missing primary language data, non-operative fracture treatment, pathologic fractures, and surgeries performed at outside facilities. In preparing the manuscript, STROBE Guidelines were adhered to. 20
Data Collection
Demographic variables, injury characteristics, and outcome variables were collected from the electronic medical record. Demographic variables included age, sex, ethnicity, race, ADI, and language. Osteoporosis (diagnosed before the injury), diabetes, and smoking status were also recorded. Additional characteristics included the year of index proximal femur fracture and year of index surgery. All proximal femur fractures were classified as femoral neck, intertrochanteric, or subtrochanteric fractures. Outcome variables included 25-OH vitamin D levels at the time of hospitalization, endocrine consult, geriatric consult, and osteoporosis treatment prescribed during indexed admission.
Patient addresses were used to identify ADI which includes 17 census-based indicators, such as education, employment, housing quality, and income to quantify the level of socioeconomic deprivation, thereby functioning as a proxy for biopsychosocial factors and social determinants of health. 21 ADI was recorded at the state level (0 to 10) using the ADI mapping tool with higher ADI scores indicating increased levels of disadvantage. 21 Quartiles were used to divide ADI into low, middle, and high neighborhood ADI (Supplemental Table 1).
Outcomes
The primary outcomes were the rate of vitamin D screening and osteoporosis treatment. The secondary outcomes were geriatric and endocrinology consultation during admission for the proximal femur fracture.
Statistical Analysis
Baseline characteristics and clinical outcomes were summarized for the group of interest using descriptive statistics with frequencies with percentages for categorical variables and means with standard deviations (SD) for continuous variables. Primary and secondary outcomes were compared by race, language, and socioeconomic status, which was quantified using ADI. In bivariate analysis, differences in outcomes were assessed using Fisher’s exact test or Pearson’s Chi-squared test for categorical variables. Results of the multivariable analysis were reported as odds ratios (OR) with 95% Confidence Intervals (CI). Bivariate statistics were performed on all outcome variables and potential confounding factors (demographic and medical). Variables with a P-value <0.2 in bivariate analysis were included in the multivariable regression models. Throughout all analyses, significance was set at a two-tailed alpha of <0.05. No priori sample size calculation was performed, as all patients meeting the eligibility criteria within the study timeframe were included. All statistical analyses were conducted using Stata17.
Results
Patient Characteristics
Patient Characteristics

Vitamin D Screening and Osteoporosis Treatment
Factors Impacting Osteoporosis and Vitamin D Screening
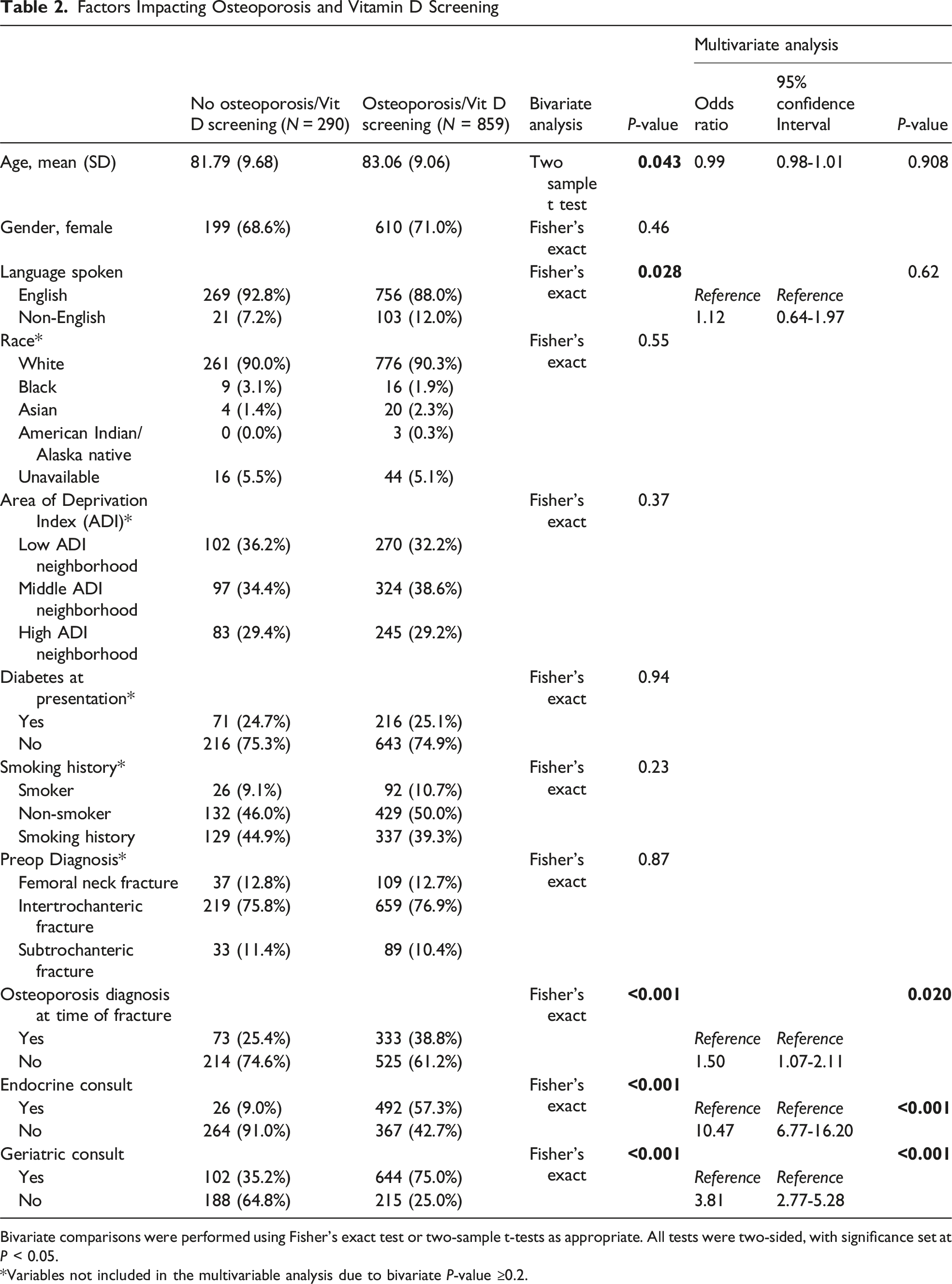
Bivariate comparisons were performed using Fisher’s exact test or two-sample t-tests as appropriate. All tests were two-sided, with significance set at P < 0.05.
*Variables not included in the multivariable analysis due to bivariate P-value ≥0.2.
Factors Impacting Osteoporosis Treatment

Bivariate comparisons were performed using Fisher’s exact test or two-sample t-tests as appropriate. All tests were two-sided, with significance set at P < 0.05.
*Variables not included in the multivariable analysis due to bivariate P-value ≥0.2.
Geriatric Co-Management and Endocrine Consultation
Factors Impacting Endocrine Consultation

Bivariate comparisons were performed using Fisher’s exact test or two-sample t-tests as appropriate. All tests were two-sided, with significance set at P < 0.05.
*Variables not included in the multivariable analysis due to bivariate P-value ≥0.2.
Factors Impacting Geriatrics Consultation

Bivariate comparisons were performed using Fisher’s exact test or two-sample t-tests as appropriate. All tests were two-sided, with significance set at P < 0.05.
*Variables not included in the multivariable analysis due to bivariate P-value ≥0.2.
Discussion
This paper aimed to explore the complex interplay between demographic factors, socioeconomic status, and the management of osteoporosis in elderly patients following proximal femur fractures. Our analysis showed that Black patients and those with higher ADI scores were less likely to receive an endocrine consult. Geriatric and endocrine co-management resulted in significantly increased odds of vitamin D screening as well as osteoporosis treatment.
Socioeconomic disadvantage impacts not only orthopedic outcomes but also extends to chronic health conditions like diabetes, obesity, and cancer.23,24 Within orthopedics, there is a growing recognition of how socioeconomic factors—such as ethnicity, language, residential area, and education—correlate with increased orthopedic trauma and poorer surgical outcomes.11-13 Relatedly, Jarman et al. found that Black race was significantly correlated with delays in care, complications, and longer inpatient stays following fall-related hip fractures. 25 Penrod et al. similarly found higher mortality and worse mobility for non-White and disadvantaged patients following hip fractures. 26
The importance of multidisciplinary care for elderly patients with hip fractures has long been stressed in the literature, with studies showing reduced length of time to surgery, shortened hospital stays, and decreased mortality with geriatrics co-management.27,28 A similar study showed that multidisciplinary care reduced emergency department stay and in-hospital complications in geriatric populations. 28
Despite the growing evidence underscoring the influence of socioeconomic disadvantages, there remains a lack of literature regarding the connection between socioeconomic factors and appropriate hip fracture management in the geriatric population. Our retrospective cohort study showed that the integration of multidisciplinary approaches, particularly geriatric and endocrine consultations, significantly improves osteoporosis management following hip fractures. Specifically, geriatric and endocrine co-management showed significantly increased odds of vitamin D screening as well as osteoporosis treatment, both essential for appropriate care of osteoporosis-defining fractures. Our findings align with existing literature, emphasizing that comprehensive care models enhance clinical outcomes for vulnerable populations.
Our results also show that Black patients (P = 0.018) and those with higher levels of disadvantage (P = 0.008) were less likely to receive an endocrine consult. These findings align with a concerning trend noted in prior research regarding racial disparities in healthcare. This discrepancy may stem from systemic biases in the healthcare system, such as implicit bias among healthcare providers, as well as structural barriers that prevent equitable access to care. The underutilization of multidisciplinary consultations for Black patients highlights an urgent need for targeted interventions aimed at improving awareness and training among healthcare providers to ensure equitable treatment pathways. These findings should be interpreted in the context of reported racial differences in osteoporosis and hip fracture rates in the United States, with approximately 10% of White patients and 6% of Black patients affected by osteoporosis. 29 Corresponding annual hip fracture rates are estimated at 140.7 per 100 000 in White women and 57.3 per 100 000 in Black women. 29
Of note, non-English speakers were nearly twice as likely to receive an endocrine consultation (P = 0.002), while patients from high ADI neighborhoods were less likely (P = 0.008). This finding further reflects disparities in healthcare access and referral practices. Physicians may be more proactive in referring non-English speakers to specialists to compensate for language barriers and ensure proper care. However, patients from high ADI neighborhoods may face systemic obstacles, such as limited healthcare access, transportation issues, and financial constraints, reducing their likelihood of receiving specialist care. However, the direct relationship between non-English speakers and ADI cannot be explicitly interpreted in this study.
Our findings also point to the necessity of routine vitamin D screening and osteoporosis treatment in the post-fracture care of elderly patients. The significant association between geriatric co-management and increased screening and treatment underscores the potential benefits of adopting standardized protocols that ensure appropriate patients undergo osteoporosis evaluations and management. Previous studies have shown that implementation of regimented care pathways, involving multiple care teams, improve patient outcomes and reduce readmission rates following geriatric hip fractures.28,30-32 Implementing these protocols not only across hospitals, but across hospital systems, could serve as a critical step in bridging the gap in care and fostering better health outcomes in demographics that are particularly vulnerable to fragility fractures.
This study is not without limitations. The retrospective design inherently limits our ability to draw causal inferences, and potential confounding factors such as chronic medical conditions may not have been fully accounted for. This study was also limited to trauma centers within the same academic medical system, with a high representation of non-Hispanic, White patients. The relatively small sample size of Black (n = 25) and Asian (n = 24) patients and homogenous patient population may not adequately represent the important characteristics of race and ethnicity. Additionally, while validated and widely used, ADI is a proxy for neighborhood-level socioeconomic status and is limited by its reliance on Census block-group data, which may fail to capture individual variability. 8 Lastly, while this study focused on vitamin D screening, recent literature has highlighted the role of vitamin K in bone health, which warrants further investigation into its potential role in fragility fracture prevention.33,34 Future studies may include larger patient groups more representative of the general population and aim to explore the underlying causes of the observed disparities in care. Longitudinal studies could provide valuable insights into the long-term impacts of tailored interventions on health outcomes, as well as the mechanisms that drive disparities in care among racial and linguistic groups.
Conclusion
This study aims to explore whether race, language, socioeconomic status, and medical co-management impact the likelihood of vitamin D screening and osteoporosis treatment after proximal femur fracture. Black patients and those with higher disadvantage levels were less likely to receive endocrine consults. Patients who had medical co-management were much more likely to receive osteoporosis workup and treatment after proximal femur fracture. The results of this study emphasize the importance of interdepartmental collaboration and regimented treatment pathways to optimize osteoporosis treatment after hip fracture and underscores the need for advocacy aimed at enhancing care delivery in vulnerable populations.
Supplemental Material
Supplemental Material - Exploring the Impact of Race, Language, Socioeconomics, and Medical Management on Osteoporosis Workup and Treatment After Proximal Femur Fractures
Supplemental Material for Exploring the Impact of Race, Language, Socioeconomics, and Medical Management on Osteoporosis Workup and Treatment After Proximal Femur Fractures by Kelsey Brown, Austin T. Gregg, Mary M. Morcos, Jacob S. Borgida, Jordan O. Gasho, Emma Kerimo, Robert K. Wagner, WuQiang Fan, Thuan V. Ly in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Ethical Considerations
This study was conducted in compliance with ethical guidelines and approved by the Mass General Brigham IRB (Protocol #2023P003580).All procedures adhered to the principles of the Declaration of Helsinki. No ethical concerns were identified in the study’s design or conduct.
Consent for Publication
This study was conducted in accordance with ethical guidelines. The Mass General Brigham Institutional Review Board (IRB) determined that this project met criteria for exemption 45 CFR 46.109(d)(#) and thus informed consent from included patients was not obtained. Patient confidentiality and data protection were strictly maintained. Institutional review board (IRB) approval was secured before study initiation.
Author Contributions
KB: conceptualization, data curation, formal analysis, methodology, writing – original draft and review & editing. ATG: data curation, methodology, project administration, writing – original draft and review & editing. MMM: data curation, methodology, writing – original draft and review & editing. JSB: conceptualization, methodology, data curation, writing – review & editing. JOG: data curation, project administration, writing – original draft and review & editing. EK: data curation, methodology, writing – review & editing. RKW: conceptualization, formal analysis, data curation, writing – review & editing. WF: supervision, project administration, methodology, writing – original draft and review & editing. TVL: conceptualization, supervision, project administration, methodology, writing – original draft and review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Thuan V. Ly reports honoraria from the AO Foundation and consulting fees from DePuy Synthes (Warsaw, Indiana). Robert K Wagner received support from the Marti-Keuning Eckhardt Foundation (Amsterdam, the Netherlands), the Cultuurfonds (Amsterdam, the Netherlands), the VSB Foundation (Utrecht, the Netherlands), and The Prof. Michaël-van Vloten Foundation (the Hague, the Netherlands). All remaining authors declare they have no conflicts of interest. Thuan V. Ly is a faculty member for AO North America Trauma/AO Trauma and a member of the Orthopaedic Trauma Association and the American Academy of Orthopaedic Surgeons. All remaining authors declare they have no non-financial interests.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.