
Abstract
Introduction:
Obesity is an oft-cited cause of surgical morbidity and many institutions require extensive supplementary screening for obese patients prior to surgical intervention. However, in the elderly patients, obesity has been described as a protective factor. This article set out to examine the effect of body mass index (BMI) on outcomes and morbidity after hip fracture surgery.
Methods:
The National Surgical Quality Improvement Program database was queried for all patients undergoing 1 of 4 surgical procedures to manage hip fracture between 2008 and 2012. Patient demographics, BMI, and known factors that lead to poor surgical outcomes were included as putative predictors for complications that included infectious, cardiac, pulmonary, renal, and neurovascular events. Using χ2 tests, 30-day postoperative complication rates were compared between 4 patient groups stratified by BMI as low weight (BMI < 20), normal (BMI = 20-30), obese (BMI = 30-40), and morbidly obese (BMI > 40).
Results:
A total of 15 108 patients underwent surgery for hip fracture over the examined 5-year period. Of these, 18% were low weight (BMI < 20), 67% were normal weight (BMI = 20-30), 13% were obese (BMI = 30-40), and 2% were morbidly obese (BMI > 40). The low-weight and morbidly obese patients had both the highest mortality rates and the lowest superficial infection rates. There was a significant increase in blood transfusion rates that decreased linearly with increasing BMI. Deep surgical site infection and renal failure increased linearly with increasing BMI, however, these outcomes were confounded by comorbidities.
Conclusion:
This study demonstrates that patients at either extreme of the BMI spectrum, rather than solely the obese, are at greatest risk of major adverse events following hip fracture surgery. This runs contrary to the notion that obese hip fracture patients automatically require additional preoperative screening and perioperative services, as currently implemented in many institutions.
Keywords
Introduction
The incidence and prevalence of obesity continues to rise, with over one-third of the US population currently afflicted 1 with an annual medical burden that accounts for an estimated 10% of all medical spending. 2 The clinically obese are more likely than the nonobese to exhibit maladies such as diabetes, coronary artery disease, hypertension, and hyperlipidemia. 3 To mitigate costs possibly associated with postoperative complications, health-care institutions throughout the country now screen surgical patients based on their body mass index (BMI) to provide additional perioperative resources for the clinically obese. These services include a mandatory preoperative echocardiogram, 2 anesthesiologists present during both intubation and extubation, and a monitored bed available when admitted postoperatively.
Hip fractures are catastrophic events 4 –6 with relatively high postoperative morbidity and mortality that constitute a significant health-care burden. 4,7 –11 However, the degree to which BMI affects the hospital course and overall outcomes of hip fracture patients is unclear. 4,12 –20 In contrast to other conditions where elevated BMI is considered a deleterious factor, higher BMI has been shown to be protective to bone health, thus mitigating the risk of hip fracture. 11 However, there is little information on the effects of obesity on postoperative outcomes in patients who have sustained these injuries. Although obesity is often correlated with increased postoperative morbidity and mortality rates, some studies have also demonstrated that low BMI in the elderly patients is a marker of declining health, thus associated with worse postoperative outcomes compared to normal-weight or overweight individuals. 21
To clarify the role that BMI plays during the postoperative course of patients undergoing surgical intervention for hip fractures, we examined the American College of Surgeons’ National Surgical Quality Improvement Program (NSQIP) database. By evaluating major and minor adverse events in the postoperative interval, we hope to identify what association, if any, exists between BMI and outcomes for hip fracture surgery. We hypothesized that obese hip fracture patients would be correlative with major adverse complications given the widespread notoriety of elevated BMI in terms of perioperative outcomes.
Methods
Case Selection and Stratification
The American College of Surgeons NSQIP (ACS NSQIP) is a prospective, risk-adjusted, multi-institutional program that collects data from numerous health-care institutions about preoperative patient characteristics and 30-day postoperative complications. The NSQIP database was queried for all patients undergoing surgical fixation of hip fractures between 2008 and 2012 using International Classification of Diseases (ICD-9) and Current Procedural Technology (CPT) codes. We identified all patients with femoral neck fractures (ICD-9: 820.00, 820.01, 820.02, 820.03, 820.09) who underwent any of following types of hip fracture surgeries: total hip arthroplasty of femoral neck fracture (CPT 27130); closed reduction percutaneous pinning of femoral neck fracture (CPT 27235); hip hemiarthroplasty of femoral neck fracture (CPT 27236, 27125); open reduction and internal fixation of a peritrochanteric, intertrochanteric, or subtrochanteric fracture (CPT 27244); and intramedullary fixation of a peritrochanteric, intertrochanteric, or subtrochanteric fracture (CPT 27245). These patients were then categorized into 4 groups on the basis of BMI: low weight (BMI < 20), normal weight (BMI = 20-29), obese (BMI = 30-39), and morbidly obese (BMI ≥ 40).
Demographics, Preoperative Status, and Outcomes
Patient demographics such as age, sex, and gender were examined along with comorbidities, American Society of Anesthesiologists (ASA) class, and preoperative laboratory results. Complications were examined as individual outcomes as well as grouped into “major” and “minor” classes.
Minor complications were defined as nonlife threatening and included urinary tract infections, superficial and deep wound infections, wound dehiscence, pneumonia, progressive renal insufficiency, and deep venous thrombosis (DVT) requiring therapy. Major or life-threatening complications included sepsis, septic shock, acute renal failure, pulmonary embolism, unplanned intubation, myocardial infarction, cardiac arrest requiring cardiopulmonary resuscitation (CPR), stroke with neurologic deficits, and ventilator requirement beyond 48 hours. Some adverse events were examined individually and not classified within the minor or major complication classes: mortality, perioperative transfusions, readmission, and reoperation rates.
Statistical Analyses
Continuous variables (eg, age) were described in terms of mean (standard deviation), whereas categorical variables (eg, race) were described in terms of frequency (percentage). Comparison between the BMI groups and continuous variables was done using analysis of variance, whereas comparison between BMI categories and categorical outcomes was done using χ2 tests. Multivariate logistic regression was used to compare rates of both minor and major complication rates across the 4 patient groups after controlling for possible confounders due to differences in background and comorbidities. All analyses were done using SAS 9.4 (SAS Inc, Cary, North Carolina). Significance was defined as P < .05.
Results
A total of 15 108 patients underwent surgery for hip fracture over the 5-year period examined. Of these, 2414 (18%) were low weight (BMI < 20), 10 734 (67%) were normal weight (BMI = 20-30), 1703 (13%) were obese (BMI = 30-40), and 257 (2%) were morbidly obese (BMI > 40). The majority of patients overall in this study were female (70.34%). Female patients (Table 1) showed a greater tendency to be either underweight or morbidly obese (P < .001). Hip fracture patients with higher BMIs tended to be younger than the patients with lower BMI (P < .001). For example, the mean age for morbidly obese patients was 69.8 years, whereas it was 77.0 for the underweight patients. Caucasians also tended to show higher levels of BMI than other racial groups (P < .001).
Patient Demographics and Comorbidities.
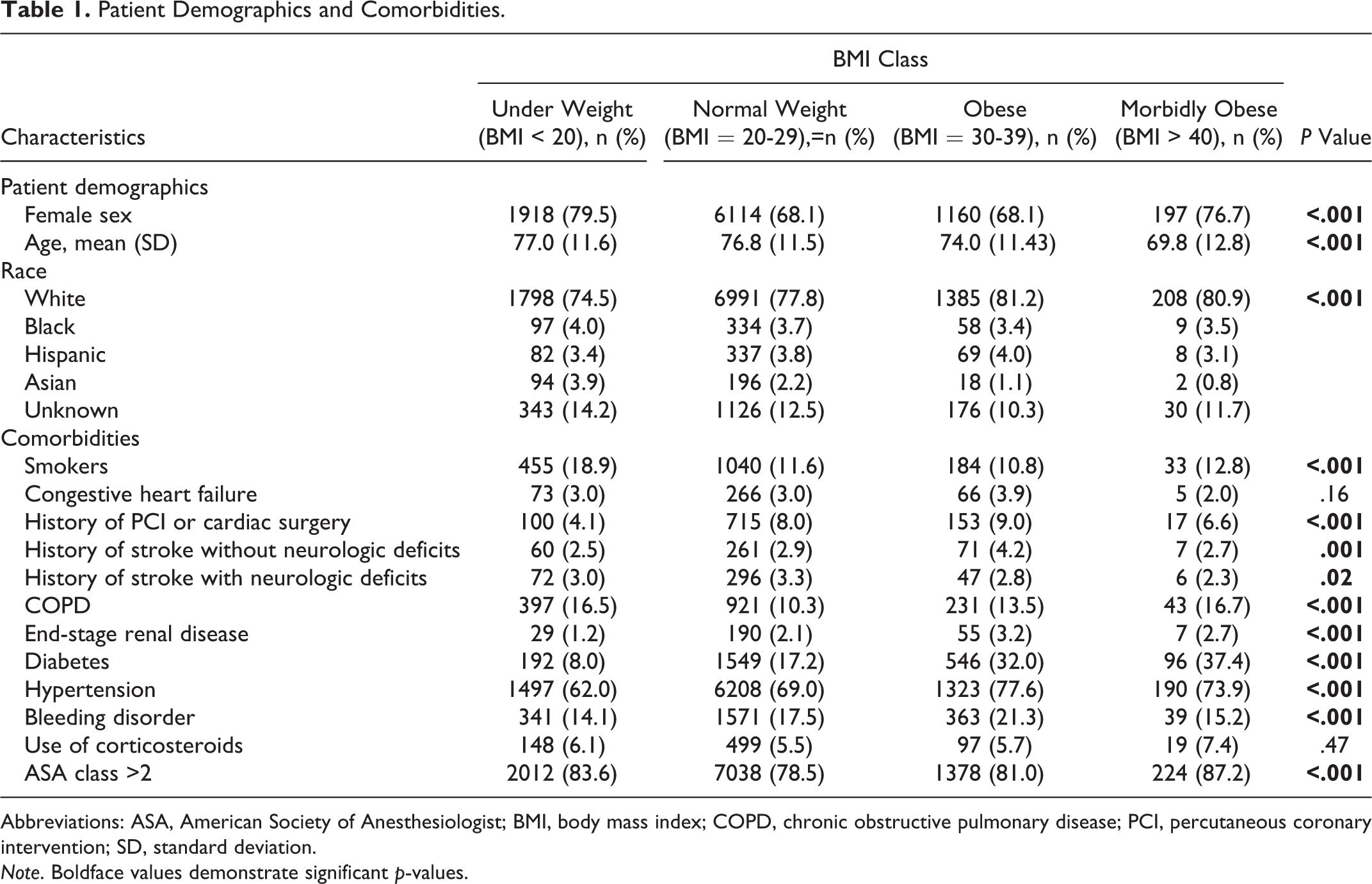
Abbreviations: ASA, American Society of Anesthesiologist; BMI, body mass index; COPD, chronic obstructive pulmonary disease; PCI, percutaneous coronary intervention; SD, standard deviation.
Note. Boldface values demonstrate significant p-values.
In terms of comorbidities, diabetes, hypertension, and end-stage renal disease demonstrated significantly higher rates with increasing BMI levels (all P < .001). The pattern was less clear for other comorbid factors. For example, smoking, ASA class <2, and chronic obstructive pulmonary disease exhibited a U-shaped distribution pattern with respect to BMI, that is, the highest rates were present in the low-weight and morbidly obese patients. Other comorbidities showed an inverted U-pattern with higher rates in the middle BMI levels: history of percutaneous coronary intervention (PCI) or cardiac surgery and bleeding disorders.
Mean operative time (Table 2) increased linearly with increasing BMI, with average surgical time of morbidly obese patients (154.6 ± 54.8 minutes) 40 minutes longer than that found in low-weight patients (113.6 ± 44.1 minutes). No other preoperative characteristics related to preoperative laboratory values or surgery type demonstrated appreciable relationships to BMI.
Preoperative Characteristics and Procedure Type.

Abbreviations: BMI, body mass index; BUN, blood urea nitrogen; CRPP, closed reduction percutaneous pinning; DHS, dynamic hip screw; IM, intramedullary; INR, international normalized ratio; ORIF, open reduction internal fixation; SGOT, serum glutamic-oxaloacetic transaminase; THA, total hip arthroplasty; WBC, white blood count.
Note. Boldface values demonstrate significant p-values.
As shown in Table 3, univariate analyses revealed that the 30-day postoperative complication rates with significant findings (P < .05) exhibited 4 different correlation patterns with increasing BMI. Mortality rates were distributed in a U-shaped fashion, with the highest rates occurring in low-weight (8.12%) and morbidly obese (6.23%) patients and lower rates in normal-weight (5.15%) and obese (3.40%) patients. Renal insufficiency, both acute and progressive, along with deep wound infections increased linearly with higher BMI. Conversely, superficial wound infections demonstrated a bell-shaped curve wherein the lowest rates occurred in low-weight (0.58%) and morbidly obese (0.78%) patients and the higher rates occurred in normal-weight (0.85%) and obese (1.82%) patients. Finally, blood transfusion rates decreased linearly with increasing BMI.
Thirty-Day Complication Rates According to BMI.

Abbreviation: BMI, body mass index; CPR, cardiopulmonary resuscitation; DVT, deep venous thrombosis.
aNational Surgical Quality Improvement Program (NSQIP) did not collect data on this outcome until 2011.
Note. Boldface values demonstrate significant p-values.
Multivariate analyses controlling for differences in background characteristics, comorbidities, and risk factors were then done to determine whether BMI was actually an independent factor related to these 30-day outcomes (Table 4). The multivariate models yielded only superficial infection rates (P = .01) and blood transfusions (P = .04) as outcomes, which were significantly related to differences in BMI. In addition, there was a possible trend for mortality to be related to differences in BMI (P = .06).
Thirty-Day Outcomes Controlled for Comorbidities and Risk Factors.
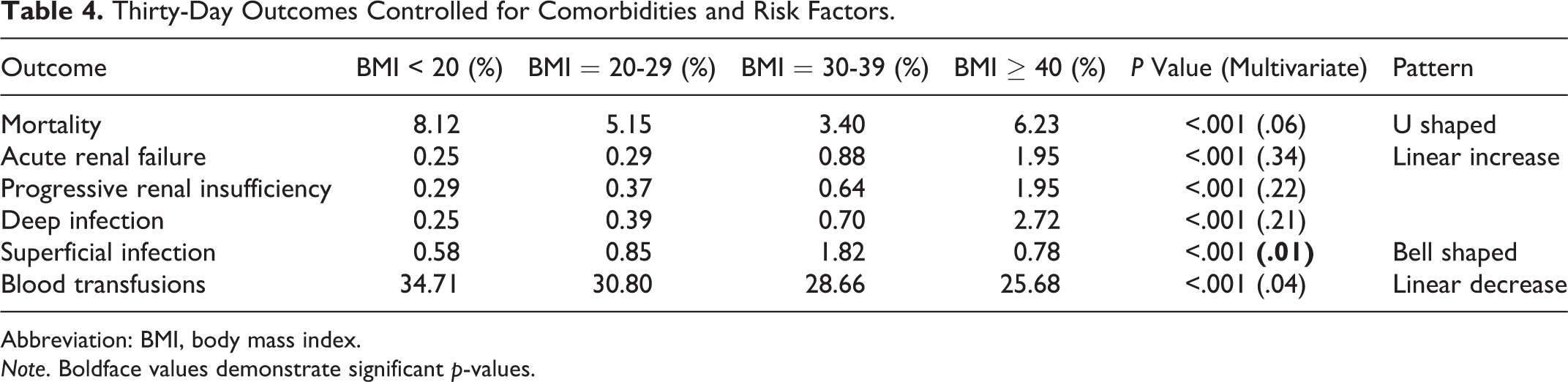
Abbreviation: BMI, body mass index.
Note. Boldface values demonstrate significant p-values.
Discussion
The burden of hip fracture care is expected to rise as the growing geriatric population suffers the associated morbidity, mortality, and costs of these injuries. 22,23 Despite being a common orthopedic problem, hip fracture management is plagued by high short-term morbidity and mortality rates which are further complicated by comorbid conditions often seen in the elderly patients. 6,8,9,24 Previous studies also indicate that hip fracture patients incur substantial financial hardship related to the costs of nursing facilities and home care; these significant expenses affect both patients and the communities responsible for their care. 4,6,25 It is therefore extremely important for physicians and surgeons to be able to identify and stratify patient populations who are at risk of complicated postoperative outcomes in order to mitigate the strain that hip fractures impose on the health-care system.
Like the elderly populace, the obese population has also increased substantially in recent years. The heightened need for medical intervention in the obese has precipitated serious public health problems associated with elevated health-care costs and higher rates of disability, 14,26 –28 which is why health-care institutions have reflexively implemented additional perioperative resources to mitigate complications in this patient population. However, in terms of bone health, obesity has historically been considered a protective factor that potentially counteracts osteoporosis in the elderly patients. 29 –31 Interestingly, recent work suggests a U-shaped relationship between bone health and BMI. Bone mineral density increases linearly with BMI and is thus protective for fractures. However, beyond a certain point, the excess weight and adipose tissue have a detrimental effect on bone. 32 –35 Therefore, patients at both extremes of BMI, both low weight and morbidly obese, are at greatest risk of sustaining fragility fractures. Additionally, the consequences of malnutrition place the elderly patients who are either low weight or obese at greatest risk of suffering from sarcopenia, further exacerbating their fracture risk. 36,37 While the complex interplay between obesity and bone health has been studied extensively for fragility fractures, there is little available information on the role BMI plays in postoperative outcomes.
When examining BMI as an independent variable, we observed a marked trend (P = .06) for hip fracture patients in which the low-weight and morbidly obese cohorts have the highest mortality rates. This U-shaped pattern with respect to mortality is strikingly similar to the previously described relationship between BMI and fracture risk, in that it was highest in low-weight and morbidly obese patients. Therefore, the elderly patients at both ends of the BMI spectrum are most vulnerable to adverse events with respect to hip fractures. Conversely, both extremes of BMI (ie, low weight and morbidly obese) had the lowest rates of superficial infection. In terms of perioperative and postoperative blood transfusions, low-weight patients actually had the highest need, with a linear decrease with respect to increasing BMI. Lastly, all of the complication rates that apparently increased linearly with increasing BMI in the univariate analyses (deep wound infection, acute, and progressive renal insufficiency) were confounded by comorbidities and thus cannot be independently attributed to BMI.
This study suggests that patients at either extreme of the BMI spectrum are at greatest risk of major adverse events following hip fracture surgery. The implications of this study are far reaching, as it contradicts the dogma that obese surgical patients are automatically at higher risk of morbidity and mortality than their nonobese counterparts. Further, not only did low-weight patients technically have the highest mortality rates, there was also a significant increase in blood transfusions within this cohort. In addition to the added risks of hematogenous infections, blood transfusions are also associated with prolonged lengths of stay, increased inpatient costs, and higher mortality rates after orthopedic procedures. 23
There are several limitations to our study, many of which are inherent to large, administrative databases. Although these data are clinically validated and collected prospectively, analysis was limited to the 30-day postoperative interval; any adverse events that occurred beyond this time point were not captured. Furthermore, this data set cannot be used to examine factors such as surgeon experience, availability of ancillary resources, or the capabilities of specific hospitals. It is possible that variations in treatment quality between providers may have skewed the observed postoperative complications.
The assumption that elevated BMI, in and of itself, is a risk factor for postoperative complications is beginning to manifest as hospital policy, indiscriminately subjecting preoperative obese patients to additional screening and services. 38 This study demonstrates that a low preoperative BMI can be just as, if not more, devastating to hip fracture outcomes as an elevated BMI. This suggests that, rather than reflexive alteration of care strategies for the obese, surgeons should tailor management, individualize care, and allocate these services to those hip fracture patients most in need. Future work should examine the impact of BMI in other fragility fractures among the elderly patients to determine whether or not obesity plays a role in postoperative outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.