
Abstract
Introduction
Hip fractures in individuals aged 65 and older present a significant burden to patients, families, and health care systems. These fractures lead to increased morbidity, loss of autonomy in Activities of Daily Living (ADLs), prolonged hospitalization, and heightened mortality rates. Despite existing knowledge, there is a need for high-quality studies to understand mid- to long-term outcomes and the impact of postoperative variables on mortality.
Methods
This retrospective matched case-control study analyzed patients who underwent operative management for hip fractures between August 1, 2021, and August 1, 2023, at a single Level II trauma center. Cases were defined as patients who expired between postoperative day 1 and ninety, while controls were patients alive at postoperative day 90. Cases and controls were matched by sex and age at the time of surgery. Patients over age 60, who underwent surgical treatment of a femoral neck or intertrochanteric fracture after receiving a preoperative block and were able to ambulate prior to their injury included. Cases and controls were matched based upon patient demographics including comorbidities. Major matched comorbidities were diabetes mellitus, hypertension, Chronic Obstructive Pulmonary Disease, and Coronary Artery Disease. A logistic regression was used to measure the association between in-hospital mobility and 90-day mortality.
Results
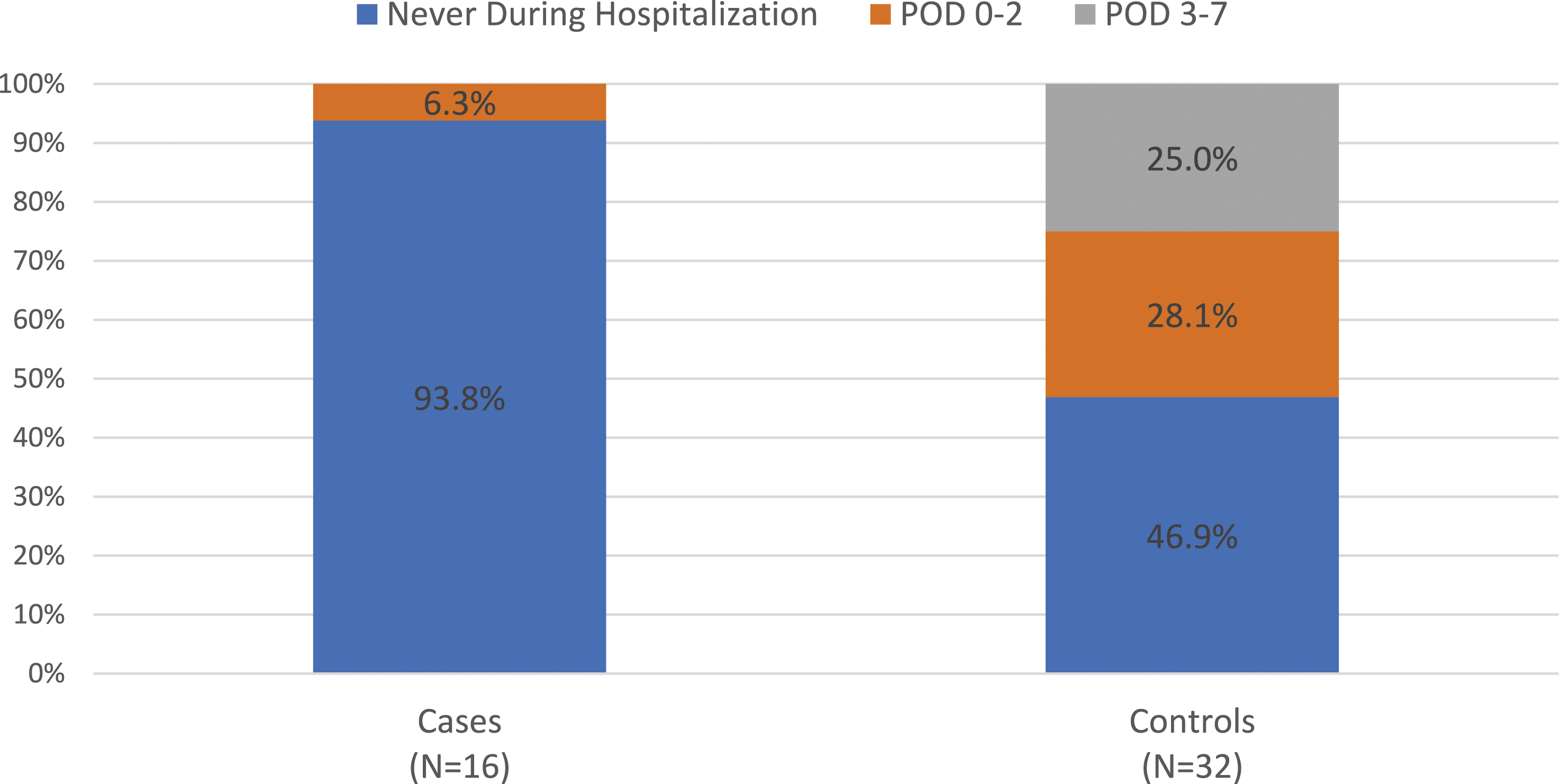
The 90-day mortality rate was 9.5% (16/169). The mean age of participants was 85.7 years, with 62.5% female. No significant differences were found in hospital length of stay or operative time. However, 37.5% of cases were discharged on hospice compared to 3.1% of controls. Only 6.3% of cases ambulated in the hospital compared to 53.1% of controls (P-value <.001). Logistic regression indicated that the odds of death were 17 times higher in patients who did not walk during their hospital stay (OR: 17.0, 95% CI: 2.91-326.0, P-value: 0.01).
Conclusions
This study highlights the critical importance of early postoperative mobilization in reducing 90-day mortality in hip fracture patients. The findings reveal that patients who ambulated during hospital admission had significantly lower mortality rates. These results suggest that early mobilization could serve as a strong protective factor against early postoperative mortality.
Keywords
Introduction
Hip fractures in individuals aged 65 and older pose a considerable burden on patients, their families, and health care systems globally.1-3 The aftermath of these fractures extends beyond the immediate skeletal injury, resulting in increased morbidity, loss of autonomy in Activities of Daily Living (ADLs), institutionalization, and heightened mortality rates.4,5 Furthermore, mortality rates at 1-year post-hip fracture are shown to be significantly higher than expected in the general population. 6
Various factors, including advanced age, male sex, clinical comorbidities, pre-fracture residence, cognitive impairment, and time-to-surgery, have been identified as predictors of postoperative mortality in hip fracture patients.7,8 Despite this knowledge, there is a recognized need for additional high-quality studies to comprehensively understand mid-long-term outcomes and determinants in this patient population. Existing literature primarily focuses on preoperative and surgical variables, leaving a gap in understanding the impact of postoperative variables on mortality. 9
Recent research highlights the acute postoperative phase as a critical period for gauging patients’ recovery trajectories and predicting their future outcomes.10,11 Notably, delayed recovery of ambulation during the hospital stay may be linked to adverse outcomes upon discharge. 12 However, the link between early postoperative mobility and 90-day mortality is an aspect that has not been extensively explored in the literature.
This retrospective matched case-control study aimed to address this gap in knowledge by analyzing the association between early postoperative mobility and 90-day mortality in patients undergoing surgical treatment for hip fractures. By evaluating the significance of postoperative variables in predicting mortality, this study seeks to contribute valuable insights to the existing body of knowledge and enhance the understanding of factors influencing outcomes in hip fracture patients.
Methods
This retrospective matched case-control study analyzed patients who underwent operative management for a hip fracture between 8/1/21 to 8/1/23 at a single Level 2 hospital in Oregon, USA. The study was approved by the Institutional Review Board in August 2023. Study participants were identified using an established research dataset that collected electronic health record data on patients undergoing hip surgery (CPT code 27245, 27236, or 27506) at a single level II trauma center. The dataset was created in December 2023 by the study investigators. Inclusion criteria were patients who suffered a low energy ground level fall that resulted in a femoral neck fractures (FNF) or intertrochanteric (IT) femur fracture and underwent surgical stabilization using a percutaneous pinning or cephalomedullary nail (CMN) placement. Only the index surgery was included for patients with more than 1 qualifying encounter in the study frame. Cases were defined as patients who expired between post-operative day 1 and ninety. Controls were patients who were still alive at post-operative day 90. Study investigators matched each case to 2 controls, without replacement, using patient sex and age at time of surgery. Patient’s younger than 60 and those who were unable to ambulate prior to the injury.
The research dataset contained Structured Query Language derived information related to participant’s demographics, clinical characteristics, and living status at post-operative day 90. Ambulation was a binary variable, defined as unassisted ambulation documented in the electronic medical record during a patient’s hospital stay. When creating the dataset, study investigators manually reviewed patient’s physical therapy notes for the entirety of the patient’s inpatient hospital stay and recorded the first post-operative day that independent ambulation without assistance or use of walking aids was documented in the electronic health record. Regardless of the hospice status, or surgical technique, all patients were started on the same postoperative physical therapy protocol with consultation to a licensed physical therapist with weightbearing as tolerated and goals of ambulation on postoperative day 1. Investigators assumed that patients who did not have any ambulation noted in their medical chart did not walk while admitted to the hospital.
Cases and controls baseline demographic and clinical characteristics were compared to identify potential confounders. Cases and controls were matched for key comorbidities including diabetes mellitus, hypertension, chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), coronary artery disease (CAD), and congestive heart failure (CHF. The cases and controls were then matched for number of comorbidities present. The normality of continuous variables was explored using histograms and Shapiro-Wilk test. Student T-tests and Mann Whitney U tests were used to compare continuous variables. Chi-square and Fisher’s Exact tests were used to compare the distribution of categorical variables. A logistic regression model was created to measure the association between in-hospital ambulation and 90-day mortality. An alpha level of 0.05 was used for all statistical tests.
Results
After applying initial exclusion criteria, we identified 169 patients with an eligible surgery for our study. 16 (9.5%) of eligible patients died within 90 days post operation and were classified as cases. Cases survived for a median of 15.5 days post operation (range: 0-75). The 16 cases were matched with 2 controls, for a total of 48 study participants included in the final analysis (Figure 1). There were 44 IT fractures and 4 nondisplaced valgus impacted FNF included in the final study. All patients with IT fracture patients were treated with CMN and all FNF patients were treated with percutaneous pinning. Table 1 describes the baseline demographic and clinical characteristics of included participants. The mean age of study participants was 85.7 years old and 62.5% of participants were female. No statistically significant differences in participant’s BMI, hospital length of stay, number of comorbidities, or operative time were found. 37.5% of cases were discharged on hospice compared to only 3.1% of controls. All patients in both cases and control groups were found to have recorded history of hypertension. No patients had CKD. The mean number of comorbidities was not statistically different between cases and controls with an average of 3.09 for cases and 3.19 for controls (P-value: 0.09). 37.5% of study participants ambulated unassisted while admitted to the hospital. Only 6.3% (N = 1) of cases were able to ambulate in the hospital, compared to 53.1% (N = 17) of controls (Figure 2). A univariate logistic regression model that was run to quantify the association between in hospital mobility and 90-day mortality found that the odds of death were 17.0 times higher in patients who did not walk in the hospital compared to patients who could walk during their admission (OR: 17.0, 95% CI: 2.91-326.0 P-value: 0.01). Consort diagram of study participants. Matched Participants Demographic Characteristics. P-value for Length of Stay calculated with t test all other P-values for continuous variables calculated with Mann Whitney U test. P-value for discharge disposition calculated with Fisher’s Exact test. 90-day postoperative mortality in relation to early postoperative mobility.

Discussion
In the pursuit of understanding and mitigating the substantial impact of hip fractures in the elderly population, this retrospective review investigated the association between early postoperative mobility and 90-day mortality. This study found a 90-day postoperative mortality rate of 9.5% which is similar to previously reported early mortality numbers. 13 Our study found that there was no statistically significant difference in BMI between cases and controls which contradicts the previously reported better clinical outcomes in obese or overweight patients.14,15
The results of this study did reveal a statistically significant reduction in 90-day postoperative mortality rates in patients who ambulated during their hospital admission. Previous studies have demonstrated that earlier ambulation does result in lower mortality rates at the 6-month postoperative mark. 16 However, our study shows that this protective affect may occur at an even earlier time frame. Additionally, the results of this study showed that ambulation during hospital admission resulted in a 17-fold reduction in mortality rates at 90 days,17,18 which is a stronger protective factor than what has been previously reported in the literature when examining longer time frames. 16 Previous epidemiological studies have shown similar relationships between discharge status and 90-day mortality rates with those patients discharged to inpatient rehabilitation facility or skilled nursing facilities demonstrating a statistically significant increase in mortality at both 90 and 180 days postop. 19 However, our study did not find a significant relationship between discharge status and short-term mortality. This further emphasizes the importance of early ambulation and 90-day mortality in hip fracture patients.
Our study’s primary limitations include its smaller sample size. Although a statistically significant association between in-hospital mobility and 90-day mortality was found, the 95% confidence interval was very large. Given the small sample size, the regression model was unable to adjust for potential confounders. In addition, the study utilized a retrospective, non-randomized study design. Further, the lack of hemiarthroplasty patients, which is another common treatment modality for femoral neck fractures may have affected the results. Using a matched case-control study design in a strictly defined population attempted to minimize the risk of confounding bias that typically present in non-randomized studies. Moreover, the charting in our retrospective study only allowed us to use ambulation without assistance as a surrogate metric for early ambulation. Whether a difference exists regarding the extent of how much mobility is required to reduce short-term mortality (ie, ambulation without assistance, ambulation with assistance, sitting in the bed, range of motion in bed) poses an important research question.
Conclusion
This study underscores the importance of early ambulation in hip fracture patients to potentially improve early term survival and provides an easily identifiable predictor of postoperative mortality in this vulnerable population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.