
Abstract
Introduction
Fractures are often caused by falls in older people. Among various causes of falls, polypharmacy is known to be a risk of falls. Furthermore, potentially inappropriate medicines (PIMs), which interact with polypharmacy, include the drugs involved in falls. Here, we primarily aimed to investigate the prescribed drugs in older surgical patients with extremity fractures to determine the frequency of polypharmacy and identify PIMs. The second aim was to clarify the characterization of prescribed drugs of older patients with hip fracture.
Materials and Methods
We retrospectively collected the following clinical data of consecutive patients aged ≥65 years who underwent surgery for extremity fractures at our hospital between April 2019 and March 2021. A total of 19 categories were considered as PIMs. The Poisson regression models were used to examine the association between the number of prescribed drugs and hip fracture prevalence.
Results
A total of 590 patients were reviewed. Our data showed that 55% of older patients with extremity fractures took ≥6 prescription drugs. The frequency of prescription of hypnotics, antithrombotic drugs, diuretics, and non-steroidal anti-inflammatory drugs was comparatively high among the 19 categories of PIMs. Multivariable analysis revealed that polypharmacy was significantly associated with hip fractures. Among PIMs, antithrombotic drugs and diuretics were significantly associated with the prevalence of hip fractures. Finally, we found a significant positive association between the prevalence of hip fracture and the number of drug categories of PIMs among older patients with extremity fractures.
Conclusions
The present study clarified the characterization of the prescribed drugs in older surgical patients with extremity fractures. Special attention should be paid to hip fractures of older patients with polypharmacy or prescribed with many drugs categories of PIMs, particularly antithrombotic drugs and diuretics.
Keywords
Introduction
The incidence of adverse drug events (ADEs) is higher in older patients than in young ones, with >10% of ADEs per year reported in older adults. 1 With an increase in the number of medications, there is a corresponding rise in ADEs, and it was observed that 15% of elderly patients visiting hospitals experience ADEs. 2 The risk of ADE increases with polypharmacy, that is, the simultaneous use of multiple drugs.3-6 Polypharmacy was reported to be associated with 1-year mortality. 7 According to reports of an increase in ADE with ≥5 prescriptions,8,9 several studies have often used 5 drugs as the cutoff for defining polypharmacy. Meanwhile, Kojima et al 10 reported a significantly higher the incidence of ADE with ≥6 drugs in older patients at a Japanese acute care hospital. Although polypharmacy itself is not considered inappropriate, potentially inappropriate medicines (PIMs) for older patients are known to interact with polypharmacy.11,12 Both Beers criteria 13 and screening tool of older people’s prescriptions and screening tool to alert to right treatment criteria (STOPP/START criteria) 14 were globally used in clinical practice to screen for PIMs. The screening tool for older persons’ appropriate prescriptions for Japanese: STOPP-J, 15 which was developed for screening PIMs of Japanese older patients, includes a list of drugs to be described with special caution.
In current aging populations, the incidence of fractures in older adults is globally increasing. 16 The most common types of fractures among extremity fractures of older adults are hip, proximal humeral, and distal radius fractures. 17 Among them, hip fracture particularly causes dysfunction and poor vital prognosis.18,19 Regardless of fracture site, fractures in older adults are often caused by falls. 20 Among various causes of falls, polypharmacy has been also reported to increase the risk of falls.21,22 Past case-control study showed that fall-related fractures and polypharmacy was closely related in older adults. 23 Furthermore, PIMs include drugs involved in falls, such as antipsychotics and hypnotics.13-15 However, the association between extremity fractures in older patients and polypharmacy or PIMs are still completely unclear. Thus, we primarily aimed to investigate the prescribed drugs in older patients with extremity fractures to determine the frequency of polypharmacy and identify PIMs. The second aim was to clarify the characterization of prescribed drugs used by older patients with hip fracture.
Methods
Subjects
We retrospectively collected the clinical data of consecutive patients aged ≥65 years who underwent surgery for extremity fractures at our hospital between April 2019 and March 2021. The participants were divided into 4 groups according to fracture sites, including proximal upper extremity (PU), distal upper extremity (DU), proximal lower extremity (PL), and distal lower extremity (DL). Cases with shoulder fractures were included in the PU group and all upper extremity fracture cases except shoulder fractures were included in the DL group. Cases with hip fracture were included in PL group and all lower extremity fracture cases except hip fracture were included on DL group. Cases with pathological fracture were excluded.
Ethics Approval and Consent to Participate
This research was approved by the institutional ethics committee. Informed consent with the ethics committee was obtained in the form of opt-out on the web-site. All study methods were conducted in accordance with the guidelines set out in the Declaration of Helsinki.
Data Acquisition
The following data were collected and assessed: age, body mass index (BMI), gender, fracture site, preoperative prescribed drugs, and medical history, including hypertension, dyslipidemia, diabetes, stroke, heart disease, and malignancy. Cognitive impairment was diagnosed based on responses to 2 questions extracted from the Kihon Checklist at the time of admission: ‘Do your family or friends point out your memory loss? eg, “You ask the same question over and over again,”’ and ‘Do you find yourself not knowing today’s date?’. 24 Decline in pre-hospital activities of daily living (ADL) was diagnosed based on the response to 1 question extracted from the Kihon Checklist at the time of admission: ‘Do you go out at least once a week?’. 24 The nutritional state and renal function were assessed based on the serum albumin and creatinine (Cre) levels, respectively, as indicated in the blood test data obtained at the time of hospitalization.
Identification of PIMs
Based on a guideline, 15 a total of 19 categories are considered as drugs to be prescribed with special caution: antipsychotics, hypnotics, antidepressants, sulpiride, antiparkinsonian drugs, steroids, antithrombotic drugs, digitalis, diuretics, β-Blockers, α-Blockers, first-generation antihistamines, H2-receptor antagonists, antiemetic drugs, laxatives, antidiabetic drugs, insulin, overactive bladder medications, and non-steroidal anti-inflammatory drugs (NSAIDs). We identified all drugs of these categories as PIMs among the prescription drugs taken by the participants.
Statistical Analyses
The Kruskal–Wallis and Pearson chi-square test were used for comparison of data among 4 groups. Data are shown as mean ± standard deviation. When we examined the association between the number of prescribed drugs and hip fracture prevalence (all participants in the PL group), the Poisson regression models were used to estimate the prevalence ratios (PRs) and 95% confidence intervals (CIs). After checking the univariable association, we adjusted for age, sex, BMI and history of hypertension, dyslipidemia, diabetes, heart disease, stroke, and cancer, as potential confounding factors. Trend test was performed by assigning ordinal scores to the categories of drug number. We also examined which drug category was associated with hip fracture, and whether number of drug category increased the prevalence of hip fracture. Poisson regression was performed using the STATA16 software (Stata Corporation, College Station, TX, USA). P values of <.05 were considered to indicate statistical significance.
Results
Baseline Characteristics (n = 590).

PU: proximal upper extremity fracture; DU, distal upper extremity fracture; PL, proximal lower extremity fracture; DL, distal lower extremity fracture; BMI, body mass index; ADL, activities of daily living.

Distribution of the number of prescription drugs used by older patients with extremity fractures.
Number of Cases Taking the Drug of Categories to be Prescribed With Special Caution.

NSAIDs, non-steroidal anti-inflammatory drugs.
Comparison Among Different Fracture Sites.

PU: proximal upper extremity fracture; DU, distal upper extremity fracture; PL, proximal lower extremity fracture; DL, distal lower extremity fracture; BMI, Body mass index; ADL, activities of daily living.
aKruskal-Wallis or x2 test.
Poisson Regression Model for Association Between Number of Prescribed Drugs and Prevalence of Hip Fracture.
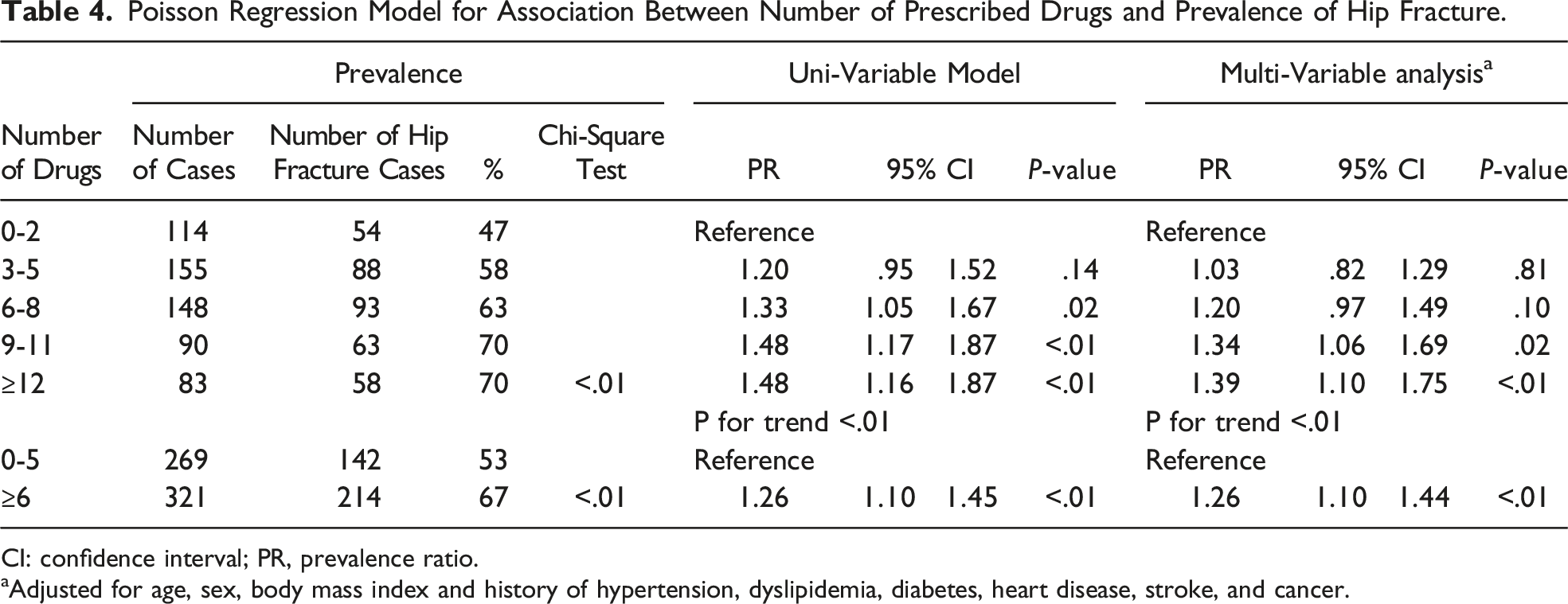
CI: confidence interval; PR, prevalence ratio.
aAdjusted for age, sex, body mass index and history of hypertension, dyslipidemia, diabetes, heart disease, stroke, and cancer.
Poisson Regression Model for Association Between Prescribed Drugs and Prevalence of Hip Fracture.

NSAIDs: non-steroidal anti-inflammatory drugs; CI, confidence interval; PR, prevalence ratio.
aAdjusted for age, sex, body mass index and history of hypertension, dyslipidemia, diabetes, heart disease, stroke, and cancer.
Poisson Regression Model for Association Between Number of Drug Categories and Prevalence of Hip Fracture.

CI: confidence interval; PR, prevalence ratio.
aAdjusted for age, sex, body mass index and history of hypertension, dyslipidemia, diabetes, heart disease, stroke, and cancer.
Discussion
Our data showed that 55% of the older patients with extremity fractures took ≥6 prescription drugs. Furthermore, multivariable analysis revealed that polypharmacy was significantly associated with hip fracture. Among PIMs, antithrombotic drugs and diuretics were significantly associated with the prevalence of hip fracture among extremity fractures. Finally, we found a significant positive association between the prevalence of hip fracture and the number of drug categories of PIMs.
With life expectancy increasing dramatically worldwide, global populations are rapidly aging. 25 Therefore, osteoporosis with aging is a major public health problem. The risk of fragility fractures due to osteoporosis in adults >50 years old is reported to be 40%–50% in women and 13%–22% in men. 26 Among common fragility fracture sites including proximal femur, spine, distal radius, and proximal humerus, the incidence of distal radius fracture does not increase significantly with age while that of vertebral fracture increases gradually from the age of 60, as do that of hip and proximal humeral fracture rapidly from the age of 70. 27 In a large Japanese study, the mortality rate at 1 year after hip fracture injury was reported to be 10.1%. 28 In addition, in patients with hip fracture, complications including respiratory disease, heart disease and cerebrovascular disease were observed in a total of 25.8% after injury. 29 Therefore, taking steps to suppress hip fracture is especially mandatory not only for the benefit of patients with osteoporosis but also for the improvement of medical economy. Previously, a population-based study reported that polypharmacy correlates with an increased risk for hip fracture in older adults. 30 Similarly, a case–control study showed that polypharmacy was significantly associated with an increased risk of hip fracture in patients with osteoporosis. 31 Although the present study only included surgical patients with extremity fractures, it showed a significant association between polypharmacy and hip fracture, consistent with previous results.30,31 Furthermore, our results clearly indicated that the more drug categories of PIMs, the more significantly the increase in hip fracture prevalence among older patients with extremity fractures. Since this is a cross-sectional study, the causal relationships remain unclear but our results indicate that older patients with polypharmacy or using drugs from many categories of PIMs need special attention to hip fracture. Meanwhile, the treatment for osteoporosis is essential for the prevention of fractures in older adults. Since drugs for osteoporosis are not included in PIMs according to the guidelines,13-15 the prescription of drugs for osteoporosis should be individualized to the patient accounting for limitations to adherence posed by polypharmacy.
Among drug categories of PIMs, hypnotics, antithrombotic drugs, diuretics, and NSAIDs were prescribed more frequently in older patients with extremity fractures in this study. Of these 4 drug categories, hypnotics are known to directly increase the risk of falls.13-15 Particularly, benzodiazepines have been reported to cause a variety of ADEs in older adults, including falls,13-15 so care must be taken in prescribing them for older patients, who should be aware of the risk of fractures due to falls. Given that there are other drugs related to fall, which are defined as fall risk-increasing drugs, 32 the relationship between extremity fractures and prescription of fall risk-increasing drugs in older adults needs to be clarified in the future. Kragh, et al 33 reported an increase in the proportion of patients taking FRIDs as well as polypharmacy after hip fracture. In the present study, we also found a significantly frequent prescription of antithrombotic drugs and diuretics in patients with hip fracture among extremity fractures. Although the relationship between the prescription of antithrombotic drugs or diuretics and hip fracture remains unclear, these results indicate that older patients who require antithrombotic drugs or diuretics may be more susceptible to severe fractures such as hip fracture. Therefore, healthcare providers should be wary of hip fracture in older patients prescribed these 2 drug categories.
This study has several limitations. First, our data were collected from a single institution. In the future, the results of this study should be validated at multiple institutions. Second, subjects were limited to patients with surgical extremity fractures. Many older patients with extremity fractures receive conservative therapy. In addition, the proportion of surgical indication varies depending on the fracture site. For example, most cases of hip fracture are indicated for surgical treatment, while cases of wrist fracture are less frequently indicated for surgical treatment compared to cases of hip fracture. Therefore, older surgical fracture patients with conservative therapy should have been included in the prescription drug survey. Third, while we examined the drugs prescribed with special caution according to the guideline, 15 we did not examine whether they were truly inappropriate for the patients. Finally, we did not evaluate whether prescribed drugs are used appropriately or not during hospitalization in this study. Considering that the orthogeriatric management was reported to succeed in preventing and treating perioperative complications in hip fracture patients, 34 geriatric intervention during hospitalization is needed to reduce polypharmacy and PIMs in older surgical patients with extremity fractures. Nevertheless, to the best of our knowledge, this is the first study to review in detail the drugs prescribed for older surgical patients with extremity fractures. We believe that the findings of this study are beneficial for all health care providers dealing with older adults.
In conclusion, the present study clarified the characterization of the prescribed drugs in surgical older patients with extremity fractures. Based on our findings, special attention should be paid to hip fractures in older patients with polypharmacy or taking with many of the drug categories of PIMs, such as antithrombotic drugs and diuretics.
Footnotes
Acknowledgments
We thank Ms. Satoko Okada and Ms. Yukari kuno for technical supports.
Author Contributions
N.F. and S.Y. designed the study. T.M., S.K., and N.F. wrote the initial draft of the manuscript. T.T., R.I., T.M., S.K., M.Y., Y.K., M.M., K.H., and M.I. contributed to the analysis and interpretation of data. T.M. performed the statistical analysis. T.T., R.I., M.Y., Y.K., M.M., K.H., M.I., and S.Y. critically reviewed the manuscript. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
Consent to Participate
We obtained informed consent of participation from all participants in the study. All study methods were conducted in accordance with the guidelines set out in the Declaration of Helsinki.