
Abstract
Introduction
Approximately one in eight patients undergoing surgical treatment for rotational ankle fractures is diabetic.1,2 Diabetic patients with Charcot neuropathy face significant challenges in managing ankle fractures due to compromised bone quality and increased susceptibility to complications, as highlighted in previous studies. 3 Complications following ankle fracture fixation in diabetic patients range between 26% and 47%, compared to approximately 15% in matched non-diabetic control groups.4–6 A study by Pincus et al demonstrated that diabetes mellitus (DM) is associated with the highest odds of amputation after ankle fracture fixation compared to other risk factors, along with a higher incidence of secondary operations and worse outcomes in terms of activity limitation scores. 6 Due to the increased risk of infection and other serious surgical complications, non-operative management of acute ankle fractures in diabetic patients was historically considered a safer option by some. 7
Ankle arthrodesis has primarily been described as a salvage procedure for Charcot arthropathy or failed fracture fixation. Techniques for ankle arthrodesis include tibiotalocalcaneal (TTC) hindfoot nails, circular external fixators, and tibiotalar arthrodesis with crossed screws or plating. While primary arthrodesis has been reported for the management of severe pilon fractures, there is limited literature on its role in acute diabetic ankle fractures without concomitant Charcot arthropathy.
Ankle arthrodesis or tibiocalcaneal arthrodesis is often considered a preferred surgical option for diabetic patients due to their susceptibility to lower limb vascular and neurologic complications, ulcers, and infections. 7 The use of a tibiotalocalcaneal (TTC) nail offers several advantages, including smaller incisions, reduced soft tissue stripping, and minimal disruption of the fracture site biology. This technique is particularly beneficial for patients with poor bone stock or compromised soft tissue envelopes, as well as those who may struggle to adhere to non-weight-bearing instructions. The primary advantages of TTC nailing include relatively smaller surgical wounds and the ability to allow immediate postoperative weight-bearing. 8
The objective of this study was to assess the functional outcomes of tibiotalocalcaneal nailing in ankle fractures among diabetic patients with Charcot arthropathy.
Patients and Methods
This prospective clinical study included
Inclusion Criteria
Patients of both sexes and all occupations, aged between 40 and 70 years, were included in this study. The study specifically targeted diabetic patients diagnosed with Charcot neuropathy who presented with either recent or neglected ankle fractures. Only cases with an ankle-brachial index (ABI) ranging from 0.65 to 1.2 were eligible for enrollment. Additionally, participants were required to be active and capable of community ambulation.
Exclusion Criteria
Patients with active infections at the time of presentation were excluded from the study. Additionally, those with open ankle fractures or fractures that had previously failed instrumentation were also excluded. These exclusions were implemented to ensure a homogeneous study population and to minimize confounding variables that could affect the outcomes of TTC nailing.
Operative Technique
Patients had prophylactic antibiotics and were positioned supine on the operating table. All surgical procedures were conducted under fluoroscopic guidance. Initial closed reduction and temporary stabilization were achieved using Kirschner (K) wires. A longitudinal incision measuring 2 to 4 cm was made to access the plantar surface of the calcaneus. A guidewire was introduced and advanced to the center of the talus's superior surface, followed by reaming to prepare the tibial canal. After graduated reaming, the TTC retrograde nail was inserted over the guidewire. Proper fracture reduction and accurate nail and ankle positioning were confirmed using fluoroscopy. The optimal ankle position was maintained at neutral dorsiflexion, 5° to 10° of external rotation, and 0 to 5° of hindfoot valgus. The final locking of the nail was performed after verifying the correct alignment and rotation both clinically and radiographically.
Sample Size and Statistical Analysis
Sample Size
Patient Selection
During the study period (October 2022 to June 2024), a total of 150 patients with ankle fractures were treated at our institution. Of these, 84 patients met the inclusion criteria for tibiotalocalcaneal (TTC) nailing. The selection process is illustrated in Figure 1. Patients were included if they had unstable, displaced ankle fractures, loss of deep sensation, and met the predefined inclusion criteria (diabetic patients with Charcot neuropathy, aged 40-70 years, and an ankle-brachial index between 0.65 and 1.2). Patients with open fractures, active infections, or failed instrumentation were excluded. Flowchart Illustrating the Patient Selection Process. A Total of 150 Patients with Ankle Fractures were Assessed, of Which 84 met the Inclusion Criteria for Tibiotalocalcaneal (TTC) Nailing.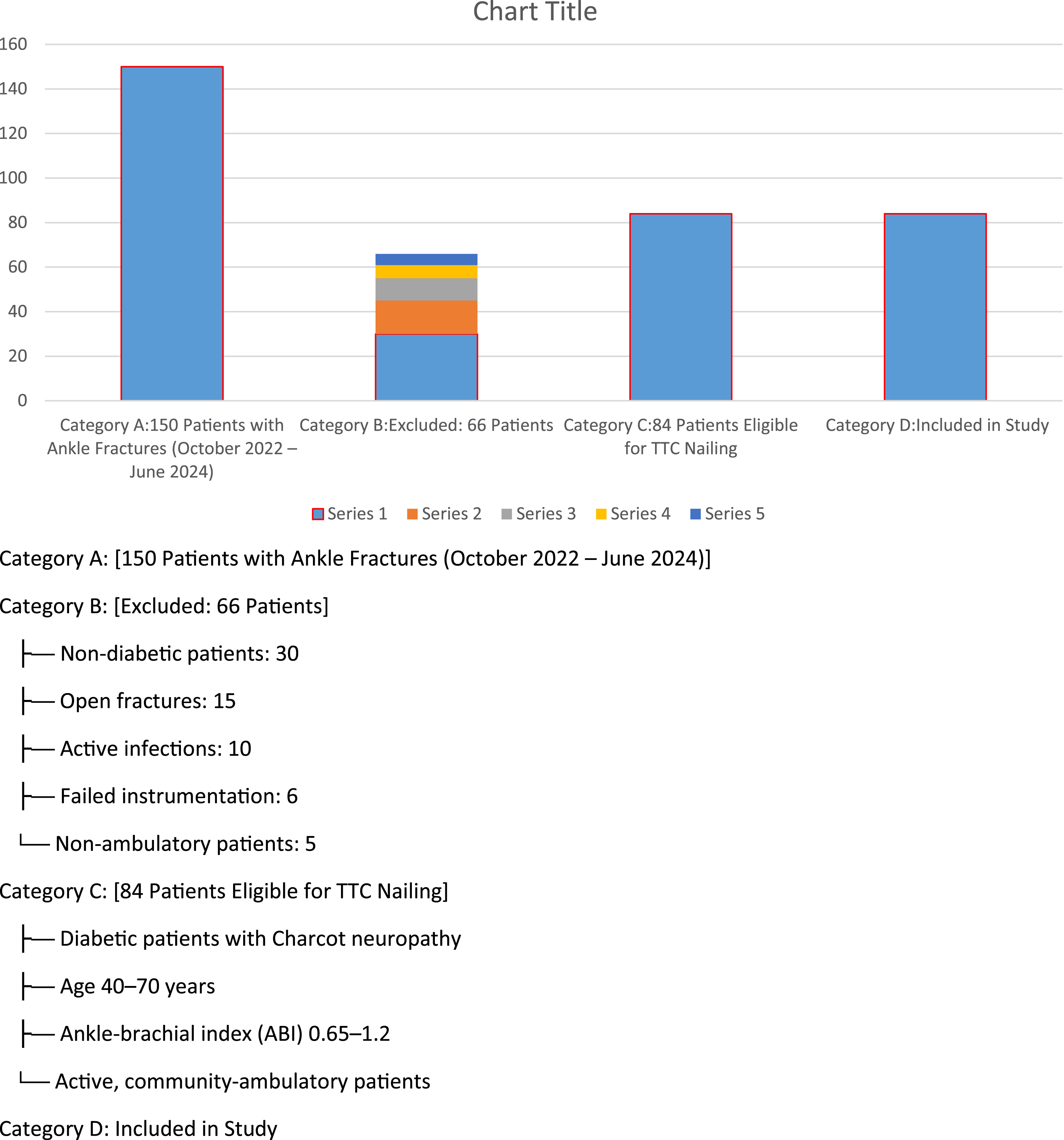
Figure 1 Flowchart illustrating the patient selection process. A total of 150 patients with ankle fractures were assessed, of which 84 met the inclusion criteria for tibiotalocalcaneal (TTC) nailing. The study included 84 patients. The sample size was calculated using a clinical sample size calculator for intervention studies, with an alpha error of 0.05, a study power of 0.80, and a 95% confidence interval (CI). Based on previous literature, the mean FAOS score improved significantly from 24.1 (range: 18-46) preoperatively to 77 (range: 69-86) at the final follow-up.
9
The sample size was determined to evaluate the clinical outcomes of tibiocalcaneal nailing in ankle fractures among diabetic patients with Charcot neuropathy. A total of
Statistical Analysis of Study Data
The data were gathered, examined, coded, and subsequently input into the Statistical Package for Social Science (IBM SPSS), version 23. For quantitative data, parametric results were summarized using means, standard deviations, and ranges, while non-parametric data were represented by medians and interquartile ranges (IQR). Qualitative variables were described using numerical counts and percentages.
The Chi-square test was employed to compare qualitative data between groups, supplemented by Fisher’s exact test when the expected frequency in any cell was below 5. For quantitative data following a parametric distribution, the independent t-test was utilized, whereas the Mann-Whitney test was applied for non-parametric distributions. A 95% confidence interval and a 5% margin of error were established. The p-value was interpreted as significant (S) if the P-value < 0.05 and as highly significant (HS) if the P-value < 0.01.
Results
The study included
Preoperative Data
Preoperative Data in all Studied Patients (n = 84) 48 Patients (57.14%) Reported Preoperative Pain.
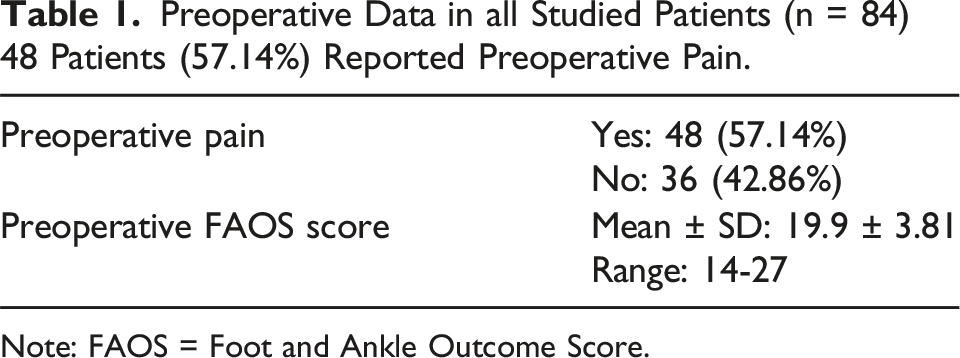
Note: FAOS = Foot and Ankle Outcome Score.
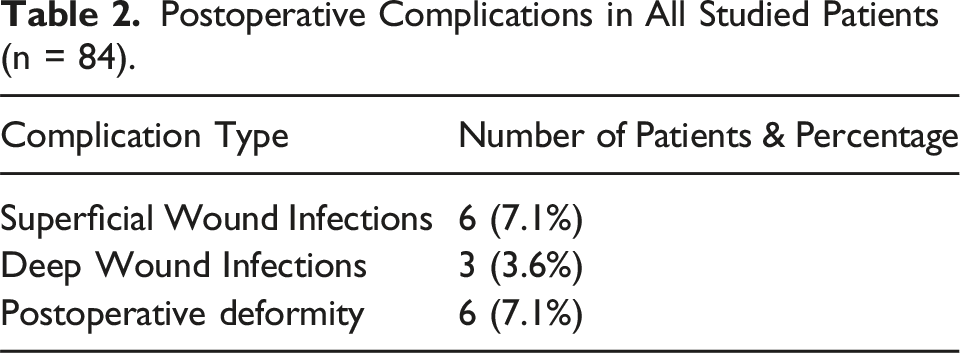
Postoperative Complications
Postoperative Complications in All Studied Patients (n = 84).
Management of Poor Outcomes
The nine patients who experienced suboptimal outcomes underscore the significant challenges associated with the management of ankle fractures in diabetic patients with Charcot neuropathy. Surgical site infections, observed in six patients, represent a well-documented complication in this population, attributable to impaired immune response and compromised vascular supply. Early identification and aggressive intervention, including thorough debridement, culture-directed antibiotic therapy, and the application of Negative Pressure Wound Therapy (NPWT), are critical to preventing progression to more severe complications such as osteomyelitis or the need for amputation.Additionally, three cases of advanced postoperative deformities were noted, highlighting the imperative of achieving robust fixation during the index procedure. In patients with poor bone quality, adjunctive measures such as autologous bone grafting or the use of locking plates may be necessary to enhance mechanical stability. Prolonged non-weight-bearing protocols and the utilization of custom orthotic devices are also essential to reduce the risk of recurrent deformity. These findings emphasize the necessity of meticulous preoperative planning, vigilant postoperative monitoring, and a multidisciplinary approach involving orthopedic surgeons, endocrinologists, and wound care specialists to optimize outcomes in this high-risk patient cohort.
Union Rates
Time to Union in all Studied Patients (n = 84). The Average Time to Union was 11.1 ± 1.88 Weeks, With a Range of 8-15 Weeks.

Correlation Analysis
Correlation Between Final FAOS Score and Patient Parameters (n = 84) No Significant Correlations Were Found Between the (FAOS).

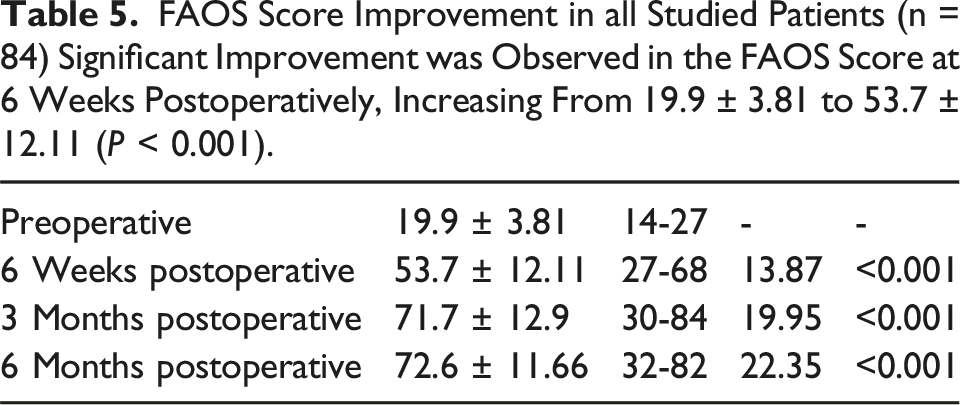
FAOS Score Improvement
FAOS Score Improvement in all Studied Patients (n = 84) Significant Improvement was Observed in the FAOS Score at 6 Weeks Postoperatively, Increasing From 19.9 ± 3.81 to 53.7 ± 12.11 (P < 0.001).
Final Results
Final Results According to FAOS Classification at 6 Months (n = 84) 54 Patients (64.3%) Achieved Excellent Outcomes, While 24 Patients (28.6%).

Case Example
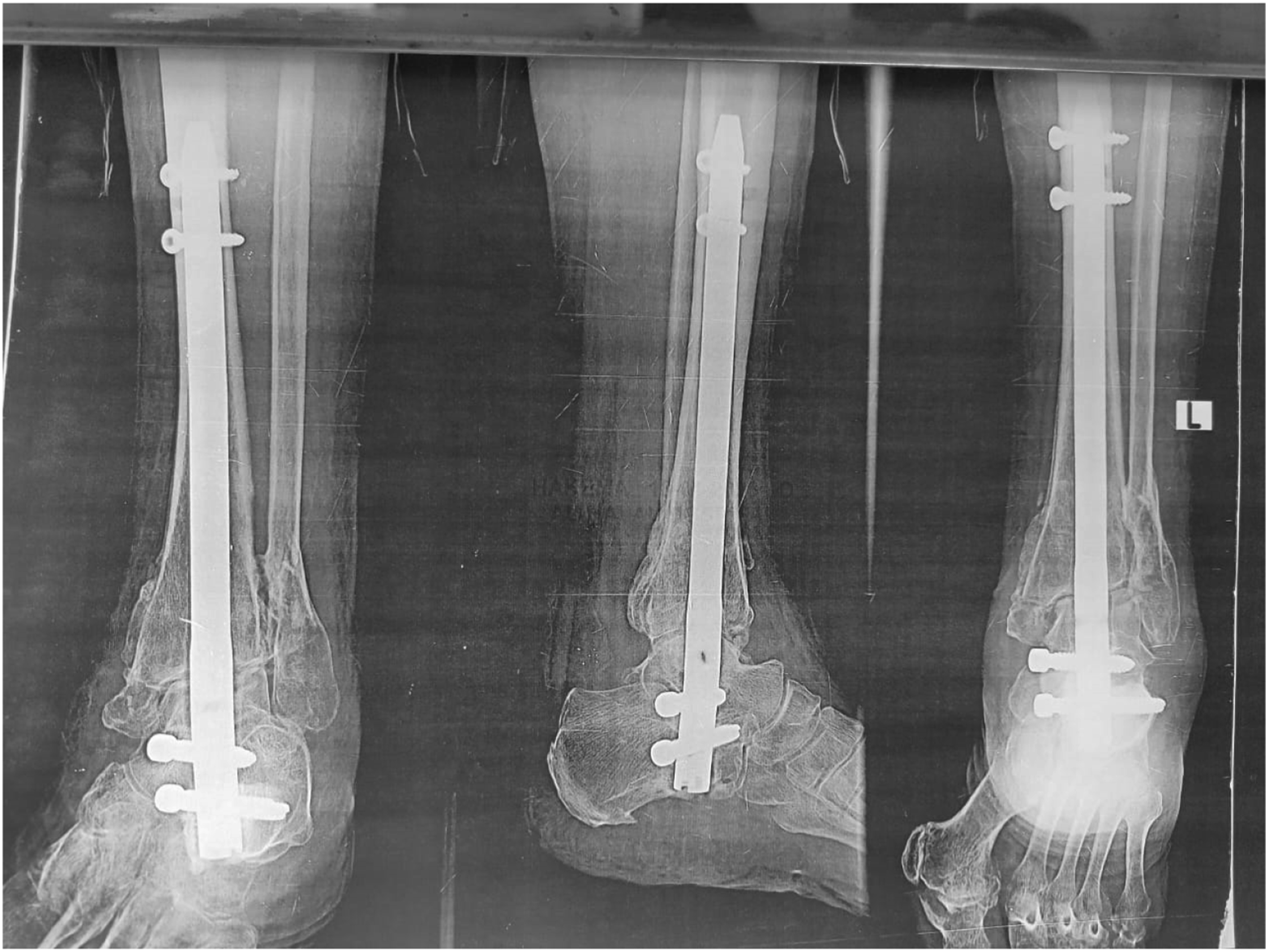
A 50-year-old female was diagnosed with a left Charcot ankle fracture. She has uncontrolled type 2 diabetes,HbA1c was 7.5, which increased the complexity of her condition and the risk of complications. She sustained a bimalleolar fracture one week prior to presentation. She underwent TTC nailing as part of the study, and her postoperative course was closely monitored. At six months postoperatively, her FAOS score improved significantly from a preoperative baseline of 28 (28%) to 68 (79%), reflecting substantial functional recovery. This case highlights the effectiveness of TTC nailing in achieving favorable outcomes, even in high-risk diabetic patients with Charcot neuropathy and ankle fractures. (Figures 2–8). Preoperative Clinical Picture of Left Ankle of the Patient. “Figure 2 Shows the Preoperative Clinical Picture of the Left Ankle, Highlighting the Deformity Before TTC Nailing”. Pre-operative X-rays, AP and Lateral. Pre-operative X-rays in Figure 3 Demonstrate the Extent of the Fracture in both AP and Lateral Views. Postoperative AP and Lateral x Rays After Open TTC Nailing. Figure 4 Confirms the Proper Alignment and Fixation of the Fracture after TTC Nailing. Six weeks Postoperative Lateral, AP and Axial x Rays. Figure 5 Shows Early Bone Healing at 6 Weeks Postoperatively, With Evidence of Callus Formation. Three Months Postoperative lateral, AP and Axial X rays. Indicates Significant Progress in Bone Union and Fusion at 3 Months Postoperatively. Six months Postoperative Lateral, AP and Axial x Rays Showing Good Fusion. “Figure 7 Confirms Successful Bone Union and Fusion at 6 Months, Showcasing the Long-Term Stability Achieved through TTC Nailing. Six months Postoperative Clinical Pictures. Figure 8 Illustrates the Final Outcome at 6 Months, Highlighting Improved Function, Reduced Swelling, and a Well-Healed Surgical Site.





Operative Technique
Open retrograde tibiotalocalcaneal ankle nailing with ankle fusion
Complications
None reported.
6 Month Postoperative Score
The FAOS score improved significantly from 28 preoperatively (28%) to 68 postoperatively (79.1%), representing a 79% improvement.
Discussion
Charcot neuroarthropathy (CN) of the foot and ankle leads to severe deformities due to the loss of neurological function and secondary vascular complications. This condition results in pathologic fractures and collapse of the pedal arch caused by repeated microtrauma. The resulting deformities often lead to ulceration due to pressure on bony prominences, and the associated instability makes conservative treatments, such as bracing, challenging and frequently results in wound complications. 10
Many authors suggest that Charcot arthropathy often develops from repeated minor trauma or isolated major trauma to neuropathic joints. In diabetic patients, the condition may be triggered by joint trauma, exacerbated by the lack of protective sensations, which predisposes them to the disease. 11
In the present study, the average time to union was “Although the complication rate of 20% may appear high, it is important to consider the complexity of managing ankle fractures in diabetic patients with Charcot neuropathy. Compared to alternative treatments, TTC nailing demonstrates a relatively lower complication rate and better functional outcomes.”
In the present study, the FAOS score improved significantly from a preoperative mean of 19.9 ± 3.81 to 53.7 ± 12.11 at 6 weeks postoperatively (P < 0.001). Further improvement was observed at 3 months postoperatively, with a mean score of 71.7 ± 12.9, and at 6 months postoperatively, with a mean score of 72.6 ± 11.66 (P < 0.001). These results align with the findings of Vitiello et al. (2020), 13 who reported a mean overall improvement in the FAOS score of 72.5% (preoperatively: 40 points vs. postoperatively: 69 points, P < 0.001). (Table 5).
TTC arthrodesis, performed with intramedullary nail fixation, has demonstrated favorable outcomes in terms of union rates, functional improvement, and reduced complications. TTC arthrodesis has demonstrated favorable clinical outcomes in both the short and long term in general medical practice. However, there have been limited investigations into the outcomes of diabetic patients, with the majority of studies focusing solely on Charcot arthropathy. 9
The use of retrograde intramedullary ankle nail fixation has gained popularity due to its clear mechanical advantages. This procedure provides stable fixation, eliminating the need for additional external immobilization devices such as casts or braces. Bone union rates range 88-100% among non-diabetic patients treated without external immobilization. 14
A similar pattern has been observed in patients with Charcot arthropathy, where the use of external immobilization is often unnecessary due to the strength of internal fixation. In our study, all 84 patients diagnosed with Charcot arthropathy achieved excellent functional recovery and could bear full weight on the affected limb. Consolidation was observed in all cases, with bone union achieved in 63 (75%) cases and solid fibrous union in 6 (7.1%) cases. The remaining cases (15 patients, 17.9%) experienced delayed union, where their fractures took longer to heal than those who achieved complete bone or solid fibrous union. No additional non-unions were reported beyond the 6 cases already mentioned. 15
Mann et al. 16 studied a different ankle fusion intramedullary (IM) nail design where a calcaneal locking screw was inserted from posterior-to-anterior instead of from lateral-to-medial. They showed that the torsional stiffness of the nail with the posterior-to-anterior screw was superior to that with the coronal plane locking screw.both methods were used in this study with good results. Oesman et al. 17 had also good results using expert tibial nail in hind foot arthrodesis in Charcot neuroarthropathy.
Alfahd et al. 18 reported contrary findings in comparing IM nail to blade plate fixation of ankle fusions in a paired cadaver study. Angular displacements were recorded in multiple planes during cantilever and torsional loading.The stability of the plate and the nail were comparable. Both fixation techniques showed decreased stability in torsion with lower bone mineral density (BMD). No correlation was found between BMD and fixation technique between a blade plate and an IM nail. In this study, relative BMD did not affect implant stability. This implies that patient's BMD is not a major factor in implant selection.
The procedure is beneficial in decreasing the rate of amputation among diabetic Charcot ankle patients. Min-Woong Sohn et al. 19 discussed lower-extremity amputation risk after Charcot arthropathy and foot ulcers. Among 911 patients with incident Charcot arthropathy and 117 patients with incident diabetic foot ulcers after eliminating patients with previous history of lower extremity amputations, crude amputation rates were 14.7% for Charcot patients and 14.5% for foot ulcer patients.Amputation rates decreased dramatically after fusion techniques as showed in this study and in comparison with other studies.
Currently, diabetic patients undergoing tibiocalcaneal arthrodesis experience a significant incidence of postoperative complications, regardless of the type of internal fixation used. Studies with the largest cohorts of diabetic patients have primarily focused on those with Charcot arthropathy, as nail fixation is more commonly utilized in this population. Retrograde intramedullary nail fixation is recommended for ankle arthrodesis in cases of Charcot arthropathy, irrespective of hindfoot involvement. 20
Due to the limited number of cases, the statistical significance of our findings is low. However, a noticeable trend toward mid- to long-term infections was observed, with superficial infections affecting 6 patients (7.1%) and deep infections requiring hardware removal observed in 3 patients (3.6%). The total number of infection cases was 9 (10.7%). Furthermore, superficial infections were managed conservatively with oral antibiotics and local wound care, while deep infections involved deeper tissues and necessitated more aggressive interventions, including intravenous antibiotics and hardware removal once complete bone consolidation was achieved. This trend may be attributed to the well-documented susceptibility of diabetic patients to infections, combined with the bulky nature of the internal fixation device. 12
Conclusion
Our findings indicate that tibiotalocalcaneal arthrodesis using retrograde intramedullary nails is a successful intervention for treating ankle and hindfoot disorders in diabetic patients, yielding favorable clinical outcomes. Significant improvements were observed in functional recovery and pain alleviation, resulting in high levels of patient satisfaction. TTC nailing in ankle fractures among diabetic patients with Charcot neuropathy is a reliable treatment option and an effective method for ankle fusion.
As with all surgical procedures, this intervention is not without complications, which in severe cases may lead to below-knee amputation. Postoperative deep infection was observed in 3 patients (3.6%). This is a serious complication that can occur even after a significant period. Hardware removal may be considered once complete bone consolidation is achieved. 21
Study Limitations
This study has several limitations, including its retrospective nature, the relatively small patient population (n = 84), the lack of advanced imaging to confirm osseous union, and a relatively short follow-up period. 22
Footnotes
Author Note
All authors have read, critically reviewed, and approved the final version of the manuscript. They agree to be accountable for all aspects of the work, ensuring the integrity and accuracy of any part of the study.
Acknowledgments
The authors would like to express their gratitude to all individuals who contributed to this study, including the participants and healthcare professionals involved in data collection and analysis. Special thanks are extended to those who provided technical support and valuable feedback during the preparation of this manuscript.
Statements and Declarations
Ethical Approval
Ethical approval was obtained from the Institutional Review Board (IRB) of [Research Ethical committee Cairo university faculty of medicine] (Approval No. [MD-31-2023]). Written informed consent was obtained from all participants.
Author Contributions
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.