
Abstract
Background
This study aimed to investigate the effect of omitting a distal locking screw in intramedullary nailing of stable intertrochanteric femur fractures on clinical outcomes.
Methods
Ninety-six patients over 65 years old with stable pertrochanteric fractures (AO/OTA 31-A1 and A2) treated with short/intermediate proximal femoral nails (PFNA-II) were randomly assigned into two groups: Group 1 (distal locked) and Group 2 (distal unlocked). Comparative analyses were conducted on operative time, total fluoroscopy time, blood loss, incision length, complications, and functional outcomes.
Results
The mean operative time was significantly shorter in Group 2 (35.73 ± 7.62 minutes) compared to Group 1 (47.40 ± 9.96 minutes) (P < 0.001). Fluoroscopy time was also shorter in Group 2 (45.92 ± 6.08 seconds) compared to Group 1 (54.02 ± 5.94 seconds) (P < 0.001). Incision length was reduced in Group 2 (9.21 ± 1.41 centimeters) compared to Group 1 (12.96 ± 1.68 centimeters) (P < 0.001). Blood loss was lower in Group 2 (187.50 ± 32.00 milliliters) than in Group 1 (208.65 ± 49.12 milliliters) (P < 0.05). There were no significant differences between the groups in fracture union time, hospital stay, fracture union weeks, or postoperative blood transfusion rates.
Conclusions
Proximal femoral nailing without distal locking offers shorter operative times, reduced fluoroscopy exposure, and lower blood loss and complications, making it a viable option for treating stable intertrochanteric fractures.
Background
The rising incidence of osteoporotic hip fractures, particularly in the geriatric population, has emerged as a major public health concern. These fractures significantly impair quality of life, leading to disability and premature death.1-4 Among osteoporotic fractures, approximately half are trochanteric fractures.5,6 Recent trends favor intramedullary fixation over extramedullary methods for these fractures.7,8 Proximal femoral nails, with their biomechanical advantages and shorter lever arms, facilitate early mobilization and bear most postoperative biomechanical forces, promoting secondary bone healing.9-12
However, distal locking screws, which stabilize the nail against axial and rotational forces, have been associated with complications such as loosening, breaking, secondary femoral shaft fractures, and fascia lata irritation.9,13,14 Additionally, distal screw insertion increases operative time, blood loss, and fluoroscopy exposure.1,2,14 Given that perioperative anemia is linked to postoperative mortality in elderly patients, minimizing surgical time and blood loss by omitting distal screws may help reduce mortality.15-18 Cadaver studies support the use of distal unlocked intramedullary nails.19,20
We hypothesized that distal unlocking does not compromise the stability or healing of proximal femoral nails and allows for quicker surgeries with fewer complications. This study aims to compare the outcomes of distal locking vs unlocking in stable pertrochanteric fractures treated with proximal femoral nails. (Figure 1).
Methods
Study Design and Ethical Considerations
This single-center, randomized controlled trial was conducted at a third Level University hospital in the capital city of Türkiye. The study was approved by the Gülhane Scientific Research Ethics Committee (Protocol No: 2021/263) and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants. This trial was not registered in a clinical trial registry before patient enrollment. Although this is a limitation, ethical approval and patient consent ensure adherence to scientific and ethical standards.
Patient Selection and Inclusion Criteria
Ninety-six patients (67 females, 29 males) with stable pertrochanteric fractures were included in the study. We divided them into 2 groups with 48 patients in each group. Only fractures classified as 31-A1 and 31-A2 according to the Orthopedic Trauma Association (AO/OTA) classification were included. The classification was determined by two independent orthopedic trauma surgeons using standard anteroposterior and lateral hip radiographs and CT scans when necessary.
Exclusion criteria included pathological fractures, open fractures, bilateral fractures, prior hip or femur surgery, severe cognitive impairment that prevented compliance with rehabilitation protocols, and patients with a history of contralateral hip surgery (eg, cannulated screws, cephalomedullary nail, arthroplasty), as this could interfere with femoral shortening measurements.
Randomization Process
Patients were randomly assigned to one of two groups: distal locked (Group 1) or distal unlocked (Group 2) proximal femoral nail fixation. Randomization was performed using a computer-generated block randomization (1:1 ratio) by an independent statistician who was not involved in the surgical procedures.
Surgical Procedure
All patients were treated using the Proximal Femoral Nail Antirotation II (PFNA-II) system. The procedures were performed by a single senior orthopedic trauma surgeon and the same surgical team to minimize variability.
PFNA-II nails were available in three different lengths (180 mm, 200 mm, and 240 mm) and distal diameters ranging from 9 to 12 mm, with a constant caput-collum-diaphyseal (CCD) angle of 130°. The decision regarding nail diameter and helical blade length (ranging from 75 mm to 120 mm) was based on patient age, bone quality, medullary width, and fracture morphology, determined intraoperatively. To ensure standardization and minimize bias, all patients received 180 mm long nails.
Surgery was performed under fluoroscopy guidance, with closed reduction achieved before nail insertion. Reduction was considered acceptable if displacement was ≤2 mm in any fluoroscopic view. The helical blade was inserted centrally in both anteroposterior and lateral planes. In Group 1 (locked group), a distal locking screw was applied through the static locking hole using an external guide. In Group 2 (unlocked group), no distal screws were used.
Intraoperative blood loss was calculated based on the weight difference of surgical sponges and the volume of aspirated fluid, excluding fracture hematoma, which had occurred at the time of injury and was not considered part of the intraoperative blood loss. Reaming was not performed in this study to minimize additional operative time, blood loss, and fluoroscopy exposure. (Figure 1). Intraoperative skin incision length, determination of blood loss and application of reduction and fixation under fluoroscopy.
Postoperative Management
Postoperatively, full-length anteroposterior and lateral radiographs were obtained to evaluate the reduction quality and implant position. On the first postoperative day, patients started isometric and isotonic lower extremity exercises under the supervision of a physiotherapist. From the second postoperative day, weight-bearing as tolerated was encouraged with walker assistance. Follow-up visits were scheduled at the first, third, sixth, and twelfth months after surgery. Fracture healing and femoral shortening were assessed using standardized radiographs (Figure 2). Preoperative and postoperative anteroposterior and lateral views of a 77-year-old female patient with an OTA 31 A1-A2 classification fracture in the distal unlocking group.
Outcome Measures
The recorded parameters for comparison included intraoperative variables such as operative time, total fluoroscopy time, blood loss, and incision length. Postoperative parameters included fracture healing, femoral shortening, blood transfusion requirement, and complication rates. Functional outcomes were assessed using the Harris Hip Score, recovery of pre-fracture walking ability, use of walking aids or a wheelchair, and mortality. Femoral shortening was evaluated on standardized anteroposterior pelvic radiographs by measuring the difference in femoral length between the operated and contralateral limb, using the greater trochanter and the lesser trochanter as reference points (Figure 2).
Figure 2 Postoperative anteroposterior pelvic radiograph showing fracture healing assessment. Femoral shortening was measured as the difference in length between the operated and contralateral limb using the greater and lesser trochanters as reference points.
Statistics Analysis
A power analysis was conducted prior to patient enrollment to determine the required sample size. Based on preliminary studies,2,3 a 25% reduction in operative time was hypothesized as the primary outcome. With a power (1-β) of 80% and a significance level (α) of 0.05, the minimum required sample size was calculated as 48 patients per group.
In descriptive statistics, continuous variables were expressed as mean ± standard deviation (SD) and median (Min-Max), while discrete variables were presented as numbers and percentages. The Shapiro-Wilk test was used to assess the normality of continuous data. For between-group comparisons, the Independent samples t test was used for normally distributed continuous variables, while the Mann-Whitney U test was applied for non-normally distributed continuous data. The Chi-square test was utilized for nominal variable comparisons in contingency tables and Fisher exact test were applied to all outcome analyses, where appropriate. Statistical analyses were performed using IBM SPSS version 20 (Chicago, IL, USA), and a P-value of <0.05 was considered statistically significant.
Results
Comparison of Patient Characteristics.

*: Mann-Whitney U test, **: Chi-Square test.
Operational Characteristics Comparison.
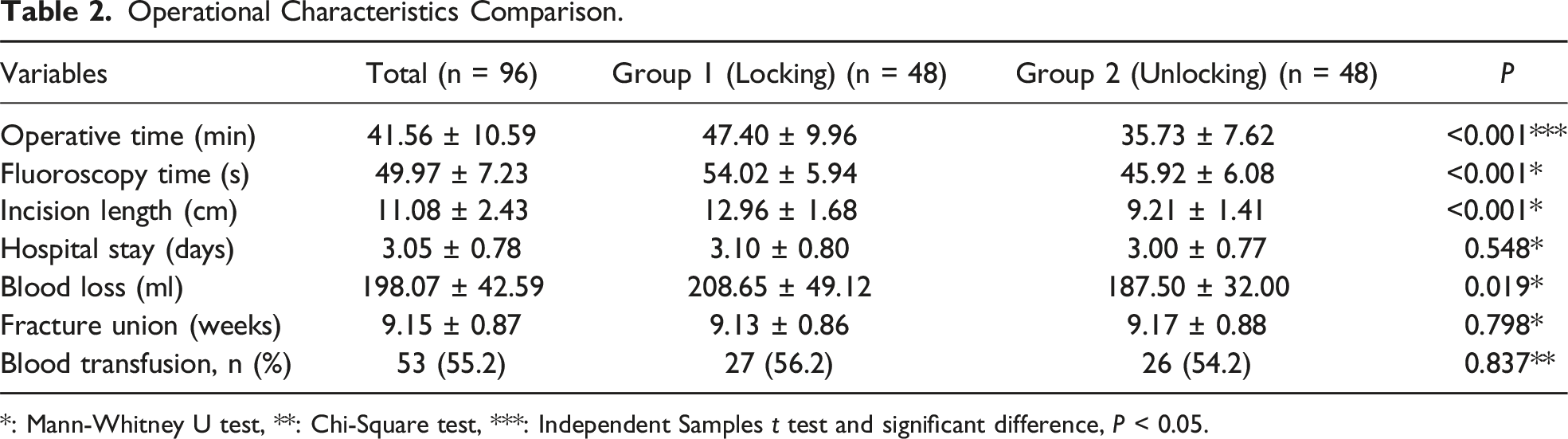
*: Mann-Whitney U test, **: Chi-Square test, ***: Independent Samples t test and significant difference, P < 0.05.
Postoperative Complications.
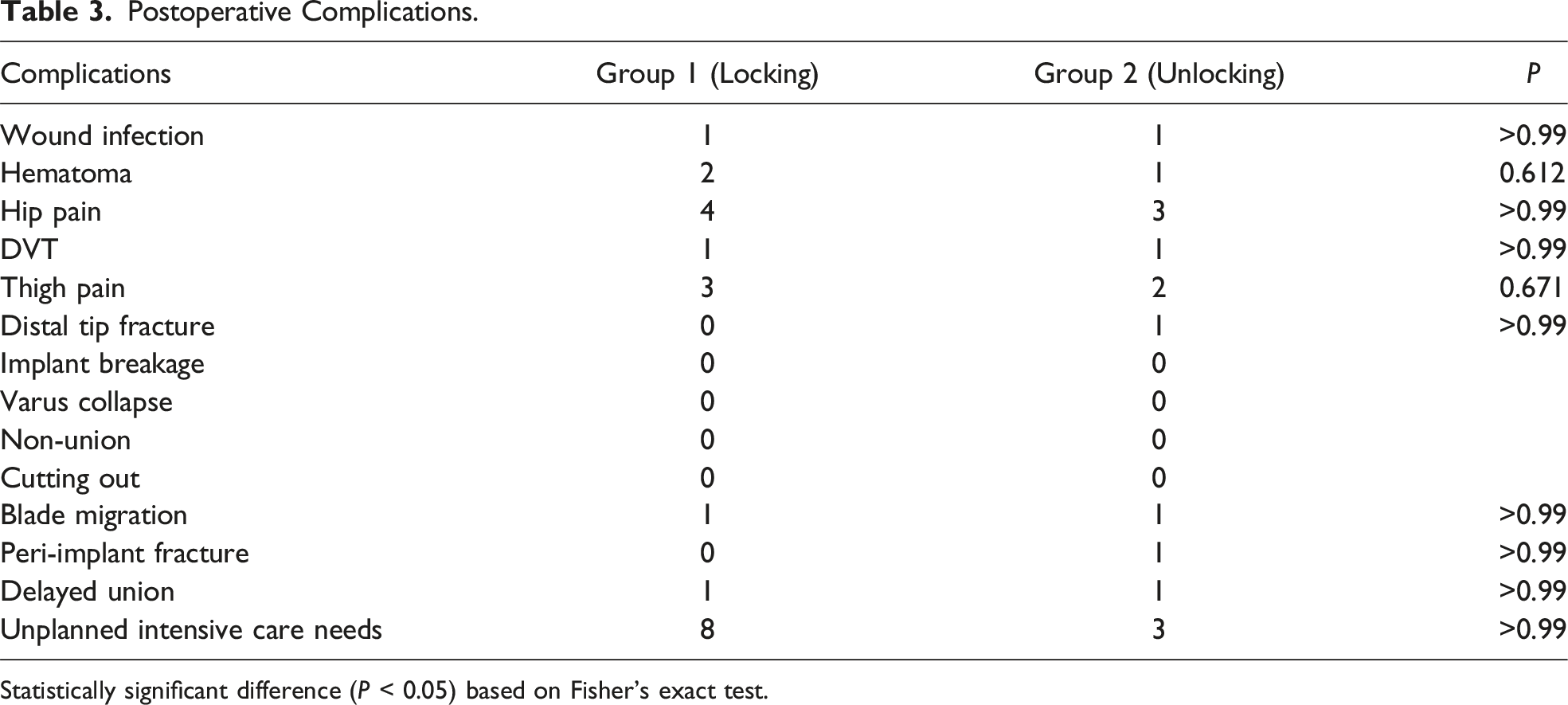
Statistically significant difference (P < 0.05) based on Fisher’s exact test.
Three patients in Group 1 and two patients in Group 2 complained of thigh pain that occurred at night and required the use of nonsteroidal anti-inflammatory drugs. In one patient of Group 2, a peri-implant fracture occurred at the distal part of the nail due to a fall 4 months after the surgery. Open reduction, internal fixation, and plate screws were applied, and complete union was achieved during follow-up. All fractures healed at the end of the follow-up, although both groups had one case of delayed union. In 8 patients in group 1 and 3 patients in group 2, intensive care was not needed in preoperative planning, but intensive care follow-up was required after surgery.
Recovery Outcomes and Clinical Outcomes.

Discussion
Osteoporotic hip fractures, prevalent in the elderly, significantly reduce quality of life and increase mortality. 2 Proximal femoral nails are preferred for their biomechanical benefits, minimally invasive technique, and reliable fixation.1,2,9,21 Adequate fracture reduction in stable intertrochanteric fractures negates the need for distal screws, as supported by comparable union rates and similar complication rates in distal unlocked nailing.
Although our study focuses on stable intertrochanteric fractures, unstable fractures (AO/OTA 31-A3) were excluded due to their inherently higher risk of mechanical failure and increased dependency on distal fixation for rotational and axial stability. Previous studies have shown that distal unlocking in unstable fractures may lead to excessive implant migration and loss of reduction, which was not observed in our cohort of stable fractures. Additional biomechanical studies, such as those by Nherera et al (2018) and Liu et al (2020), have demonstrated that unlocked femoral nails can provide sufficient stability in well-reduced fractures without compromising clinical outcomes.22,23 Biomechanical studies corroborate the clinical findings, suggesting that distal unlocking does not compromise stability in treating stable trochanteric fractures.3,19,24,25 Clinical studies also indicate that omitting distal screws reduces operation time, blood loss, and fluoroscopy exposure without increasing complications.1,2,26 Our study aligns with these findings, demonstrating that unlocked proximal femoral nails offer significant benefits in reducing surgical time, blood loss, and radiation exposure.
Furthermore, the use of distal locked or unlocked fixation may have variable effects depending on patient factors such as bone quality, BMI, and medullary canal width. Our study did not specifically analyze the influence of BMI on postoperative complications. However, previous literature suggests that higher BMI may increase implant stress and the risk of peri-implant fractures in unlocked configurations.27,28 A recent study also reported that complication rates are higher in obese patients with intertrochanteric fractures, emphasizing the need for careful implant selection in this population. 29 Future studies incorporating BMI as a variable may provide further insights into patient selection for distal unlocked fixation.
In elderly patients, prolonged surgery and blood loss are linked to higher mortality.15,18,30,31 Omitting distal screws can mitigate these risks. Our findings show a 25% reduction in operation time and a 21% decrease in blood loss in the unlocking group, enhancing patient outcomes and potentially reducing mortality rates. Additionally, the lower fluoroscopy time in the unlocking group minimizes radiation exposure, benefiting both patients and surgical teams. 32
The significant difference in age between the two groups (locking group being older) may have influenced the overall recovery process. Advanced age is a well-established factor affecting postoperative recovery, mobility outcomes, and complication rates in geriatric fracture patients. Although our study demonstrated no significant differences in functional scores or mortality between the groups, future studies with age-matched cohorts may help further clarify the impact of age on the outcomes of distal locking vs unlocking.
While the distal locking screw is expected to increase the stability of the implant, it should be taken into consideration that it may cause potential problems besides increasing operation time, radiation exposure time, and blood loss.14,33 Hesse et al found that repetitious drilling and over-tightening the distal screw could cause femoral fracture. 14 In their prospective study, Radford et al advocated that distal locking screw weakened the bone and should be avoided whenever possible. 32 On the other hand, Skala-Rosenbaum et al asserted that unlocked nails did not prevent femoral fractures in their retrospective study on peri-implant fractures of 849 nails. 13 In this study, the locked and non-locked groups had similar postoperative complication rates. In the locked group (Group 1), we had 8 patients who needed intensive care after surgery in planning, while in the unlocked group (Group 2), this number was 3. Although not statistically significant, this may be associated with the duration of anesthesia.
One of the concerns with distal screw insertion is the potential for arterial injury due to drilling. While our study did not observe any direct vascular complications, previous reports have documented cases of superficial femoral artery damage from distal interlocking screws. 34 This risk should be considered, especially in elderly patients with atherosclerotic vessels.
The relatively low number of patients is one of the limitations of this study. All surgical procedures were performed by the same experienced surgeon and surgical team in this study, which increases the value of this study by avoiding surgical technical errors. A relatively short follow-up period can be another limitation that might prevent us from encountering some complications. Additionally, we did not include data on BMI, which could influence implant stability and complication rates. Future studies incorporating BMI and its relationship to distal fixation choices may provide further insights.
Another limitation is the lack of multi-center validation. Since this study was conducted in a single high-volume center, the results may not be fully generalizable to hospitals with different surgical expertise, patient demographics, or implant selection preferences. Further multi-center studies are needed to confirm the reproducibility of these findings in diverse clinical settings. There remains a need for prospective studies with long-term follow-up.
Conclusion
Our study highlights that distal unlocked proximal femoral nailing provides comparable clinical outcomes while offering perioperative benefits such as reduced operative time, intraoperative blood loss, and fluoroscopy exposure. This approach may be particularly advantageous in elderly patients, where minimizing surgical burden is a priority.
Additionally, avoiding distal locking may reduce the need for intensive care in high-risk elderly patients, possibly due to shorter anesthesia duration and reduced intraoperative stress. While no significant differences in postoperative complications were observed, factors such as implant migration, peri-implant fractures, and femoral shortening warrant further investigation.
In conclusion, distal unlocked proximal femoral nails appear to be a safe and efficient alternative for well-selected elderly patients with stable intertrochanteric fractures. Future studies should focus on refining patient selection criteria and assessing long-term biomechanical stability to optimize clinical guidelines.
Footnotes
Author Contributions
SS, CY and ÖE contributed to the analysis and interpretation of the data and the writing and revision of the manuscript. CY, HYT, and ÖE contributed to the analysis, interpretation of the data, and writing. SS, and HYT contributed to the data collection, analysis, and methodology. ÖE, SS, and CY contributed to the experimental design, data collection, and data revision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
All data and material are available from the corresponding author as needed.