
Abstract
Purpose
With the aging population and rising life expectancy the incidence of trauma-related injuries, particularly proximal femur fractures, is expected to increase. Complications such as fracture-related infections (FRI) significantly impede the healing process and pose substantial risks to patients. Despite advancements in understanding, diagnosing, and treating FRI, challenges persist in achieving optimal outcomes. This review addresses the significance of FRI following proximal femur fractures, emphasizing diagnostic methodologies and therapeutic modalities to enhance clinical care.
Findings
Notably, a consensus definition for FRI has been established, providing clarity for accurate diagnosis. Diagnostic criteria encompass confirmatory and suggestive elements, facilitating precise identification of FRI. Therapeutic strategies for FRI in proximal femur fractures include a spectrum of surgical and antimicrobial approaches. Surgical interventions, ranging from debridement with implant retention over implant removal/exchange to staged conversions to arthroplasty, are tailored based on fracture stability, individual patient factors, and infection characteristics. The intricate decision-making process is elucidated, highlighting the importance of individualized treatment plans and multidisciplinary collaboration. Antimicrobial therapy plays a pivotal role in FRI management, with empirical regiments targeting common pathogens and local delivery systems offering sustained antibiotic release. Microbiological analysis and collaboration with infectious disease specialists should guide antimicrobial treatment and ensure optimal therapy efficacy.
Conclusion
Managing FRI following proximal femur fractures requires a tailored, multidisciplinary approach. Treatment strategies should be guided by diagnostic precision, patient-specific considerations, and collaboration among surgical, infectious disease, and clinical teams. Implementing comprehensive therapeutic approaches is essential for mitigating the impact of FRI and improving patient outcomes.
Introduction
As life expectancy continues to rise, there is a projected increase in the number of trauma patients, particularly among the elderly population. 1 Among these cases, proximal femur fractures are the most common type, with incidence rates of 109 per 100,000 inhabitants in Germany. 2 A study conducted by Gullberg et al 3 , in 1997 already predicted a doubling of femoral fractures worldwide between 1990 and 2025, with an additional doubling by 2050, resulting in up to 21.3 million fractures globally. 3 Other analyses estimated an increase from 1.26 million in 1990 to 4.5 million by 2050. 4 While fractures themselves can be debilitating, the additional development of an infectious complication significantly complicates the healing process and poses a serious risk to the patient’s health.5,6 A recent meta-analysis pooled data from 20 studies, comprising 88,615 patients, reported an incidence rate of fracture-related infection (FRI) of 2.1% (95% CI: 1.54%–2.62%). 7 The most commonly identified causative pathogens are Staphylococcus aureus (31.4%-37.4%) and Staphylococcus epidermidis (16.9%-25.8%). 8 One particular challenge is the formation of biofilms by the infectious agents. A biofilm refers to the aggregation of freely moving (planktonic) bacterial cells on surfaces, where they transform into sessile cells and create an extracellular polysaccharide matrix. The biofilm provides a shield against the immune system’s defenses and hampers the effectiveness of antimicrobial treatments. 9 Consequently, the administration of antibiotics alone is usually insufficient to completely eradicate the infection, necessitating surgical interventions. To achieve favorable results for the affected patients suffering from FRI after proximal femur fracture, surgeons have to take into account several aspects. A multidisciplinary team approach is therefore highly recommended and has been shown to be associated with more favorable outcomes. In addition to the patient’s overall state, local considerations must be taken into consideration when determining if re-osteosynthesis is feasible and appropriate or whether arthroplasty yields a superior outcome. 10 Due to the high vulnerability of these often elderly and multimorbid patients, individual treatment concepts must be pursued which are tailored to the expectations and resources of the patients. Therefore, the present review aims to emphasize the significance of FRI after proximal femur fractures, summarize diagnostic approaches, and highlight therapeutic options to enhance the quality of care in clinical practice.
Definition and Diagnostics
For a considerable period, a clear definition of infections following fractures treated with internal fixation with metallic implants did not exist. Diagnostic criteria were often extrapolated from periprosthetic joint infections (PJI). 11 Plenty of terms describing bone infections are available, such as implant-associated infection, fracture-related infection, posttraumatic osteomyelitis, or infected nonunion. Most of the past studies in the field did not use a valid definition, 12 leading to inconsistency and restricted informative value as differentiated terminology is a prerequisite for accurate diagnosis and consequently optimal therapy. 13
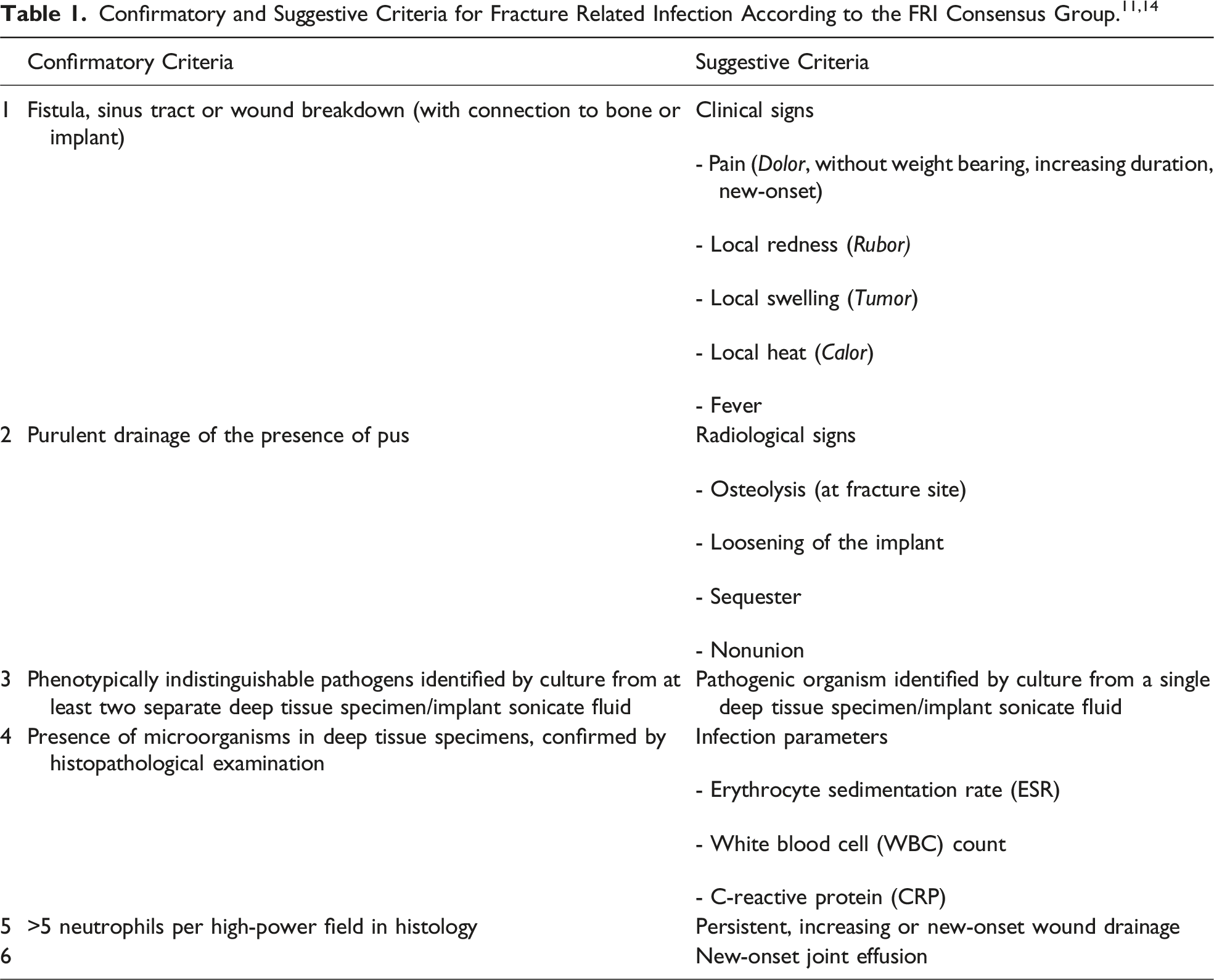
In many cases FRI can be identified clinically. The presence of a fistula, wound breakdown, or purulent drainage following osteosynthesis is considered definitive evidence of FRI, necessitating surgical intervention to treat the infection and identify the responsible pathogen. However, the diagnosis of FRI is multifaceted and can be challenging due to overlapping symptoms with normal fracture healing in the acute state and subtle clinical signs in later stages impeding the differentiation from noninfectious causes.11,14
When a patient exhibits non-specific inflammatory signs such as pain (dolor), redness (rubor), warmth (calor), swelling (tumor), fever, or elevated infection parameters, along with suggestive radiological findings, surgical exploration can be used to confirm the diagnosis, especially when alternative causes for the symptoms are unlikely. Serological markers like C-reactive protein (CRP), leukocyte count (LC), and erythrocyte sedimentation rate (ESR) are not reliable as standalone indicators of FRI in these cases. Ultimately, microbiological analysis, including cultures from deep tissue or implants, and histological examination are essential for confirming the presence of FRI and guiding appropriate treatment.11,14
If the patient’s condition permits, a comprehensive radiological assessment, including conventional radiography and computed tomography (CT), should be performed preoperatively. The imaging can not only help confirm the diagnosis but also provide critical information for surgical planning, such as assessing fracture healing and implant stability. 15
Nuclear imaging techniques, such as positron emission tomography (PET) scans, can complement the diagnostic process by localizing the infection, assessing its extent, and identifying additional infectious foci. 15 In certain cases, especially involving the proximal femur, preoperative diagnostics should also include a puncture of the ipsilateral hip joint to evaluate potential joint infection.
Overall, the diagnosis of FRI involves a combination of clinical assessment, imaging, microbiology, histology, and serological markers, with each method contributing to a comprehensive diagnostic approach.
Therapy
Surgical Treatment
Several factors should be considered for the treatment of an FRI of the proximal femur (Figure 1). The choice of therapy depends primarily on the question of whether the initial fracture is healed or not. If fracture consolidation is not yet achieved, assessment of implant stability and feasibility of re-osteosynthesis in case of unstable fixation is the key. Thereby, the type of implanted fixation device crucially influences the surgical approach. Commonly used implants for osteosynthesis of the proximal femur include intramedullary nails, canulated screw fixation, dynamic/compression hip screws and locking plates.16-18 Treatment algorithm for FRI of the proximal femur.
Therapy of FRI should always combine antimicrobial medication (systemic and local) with surgical treatment. The surgical treatment of FRI comprises two main concepts: debridement, antimicrobial therapy, and implant retention (DAIR) or debridement, antimicrobial therapy, and implant removal/exchange. In case of the proximal femur a staged conversion to arthroplasty is an additional therapy option if fracture reduction or stability cannot be achieved or osteosynthesis seems not reasonable due to extensive bone loss, femoral head necrosis or screw cut-out.
In contrast to periprosthetic joint infection (PJI) the applied devices are temporary implants in cases of FRI. Their purpose is providing sufficient stability until the fracture is consolidated.
Healed Fracture
Once the fracture is healed the fixation device as the focus of infection-carrying biofilm can be removed. 19 Therefore, surgical debridement and antimicrobial therapy (local and systemic) after implant removal can be deemed as effective treatment approach for FRI after fracture healing. 20
Incomplete Fracture Healing
If the current fixation appears stable despite the fracture not being fully healed, a DAIR procedure can be adequate to eliminate or mitigate infection until fracture union is achieved. Subsequently, the internal fixation devices can be removed.
Intramedullary fixation devices implicate a unique challenge in this context. They pose a significant risk factor for treatment failure when attempting to retain implants during infection, particularly when compared to plates. 21 Due to their intramedullary position and the resulting limited access for appropriate surgical debridement, they should generally be exchanged along with intramedullary reaming and irrigation to address the infection. Thereby sufficient reduction and valgization should be aimed for to finally achieve fracture consolidation.22,23 Given that the most commonly used devices for osteosynthesis of the proximal femur (nails and dynamic/compression hip screws) include intramedullary components, the DAIR procedure is rarely feasible in these cases since sufficient debridement cannot be achieved due to the intramedullary implant. In the preparation for a proximal femur nail exchange, it has to be especially assessed if a sufficient refixation of the femoral neck screw is feasible. Otherwise, conversion to arthroplasty would be the treatment of choice.
Insufficient Fracture Fixation
If the current osteosynthesis does not provide sufficient stability presented by implant loosening or secondary fracture dislocation it has to be decided whether a re-osteosynthesis is feasible and reasonable. In this case depending on the severity of the infection a one- or more-stage exchange must be planned. In such cases, a variation or combination of fixation principles can be reasonable (intramedullary/extramedullary, see case 2).
Failed Osteosynthesis
When re-osteosynthesis is no option, for instance due to femoral head necrosis, extended osteomyelitis of the proximal femur or cut-out of a femoral neck screw leading to joint destruction or extensive bone loss, the recommended surgical approach is conversion to total hip arthroplasty. This approach is best performed in a staged manner and includes the temporary implantation of a hip joint spacer made of antibiotic-loaded cement. To address the medullary canal with local antibiotic treatment manually cement-covered intramedullary nails can be used24-26 (see case 3). In the authors’ experience an implant-free interval of 6 weeks with systemic antimicrobial therapy before implantation of an endoprosthesis proved beneficial and can still be regarded as gold standard of therapy. 27 However, depending on the specific pathogen and systemic and local infection parameters the implant-free interval can be reduced. If the pathogen is already identified preoperatively by diagnostic joint aspiration and turns out to be easy-to-treat (low resistance rate) a single-stage conversion to arthroplasty can be considered. However, in some cases multiple revision procedures and exchanges of the cement spacer may be necessary to control the infection before joint replacement. If the greater trochanter has to be resected during debridement, there are modular femoral replacement systems available on the market that allow for a sufficient solution in these cases.
Acuteness of Infection
According to the onset of symptoms FRI are historically divided into acute and chronic infections respectively early’ (within 2 weeks after fracture/surgery), ‘delayed’ (3-10 weeks after fracture/surgery) and ‘late’ FRI (over 10 weeks after fracture/surgery). 28 This classification is based on the concept of biofilm formation, where the maturation of the biofilm over time reduces the susceptibility of the bacteria to antibiotics.29,30
Current recommendations include acuteness of infection as one of the main criteria for the choice of treatment and implant retention is no option in case of chronic infections. However, recent studies show that the spectrum of pathogens 31 as well as the effectiveness of different treatment options is not significantly influenced by the factor of time from injury/surgery. 20 Morgenstern et al. investigated the influence of duration of infection especially on the efficiency of the DAIR procedure in a systematic review and meta-analysis. They found high success rates in the case of early and delayed FRI (82%–100%) and still 67% successful treatment of late infections. 32 Thus, in cases with stable fixation of complex, multi-fragmentary fractures in which breakup of osteosynthesis is undesirable and might end up in a situation of impossible refixation, DAIR could be a reasonable therapy option even for delayed or late FRI. Only in case of an infected nonunion which is a special type of chronic FRI 33 where fracture healing without revision is not expectable the DAIR procedure is categorially contraindicated in our opinion, which is in line with the observations made by Morgenstern and coworkers, that DAIR has worse outcome in chronic FRI.
Microbiology and Antibiotic Therapy
The surgical intervention should always include the collection of an adequate number (3-5) of deep tissue samples for microbiological and histological examination. Empiric antimicrobial therapy should be delayed until sample collection is completed to improve the chance of pathogen identification as long as the patient’s condition permits. 19 However, studies in PJI patients showed that standard perioperative antibiotic prophylaxis has not to be dispensed with. 34
More than half of all FRI are caused by Staphylococcus species (Methicillin-sensitive Staphylococcus aureus, Methicillin-resistant Staphylococcus aureus and Staphylococcus epidermidis) followed by Gram-negative bacteria, Streptococcus and Enterococcus species. 31 Several studies could show that microbiology as well as the efficacy of empiric antimicrobial regimes do not significantly differ between early, delayed, or late infections.10,31 Effective empiric antimicrobial combinations include meropenem + vancomycin, gentamicin + vancomycin, co-amoxiclav + glycopeptide, or piperacillin/tazobactam + glycopeptide with equally high sensitivity rates of 100% in early FRI, 93.3%–96.7% in delayed, and 84.2%-92.1% in late-onset FRI. 8 Empiric antibiotic monotherapies should be avoided due to high rates of drug resistance.
Patients in our cohort are generally treated with an empiric combination of amoxicillin/clavulanic acid + vancomycin and local gentamicin + vancomycin. The systemic therapy is further adapted according to the microbiological results and should be applied over a period of at least 12 weeks after implant retention or exchange respectively 6 weeks after implant removal. To prevent multi-drug resistances the systemic use of reserve antibiotics such as meropenem should be restricted to septic patients or high-risk infections with difficult-to-treat pathogens. 10 Close collaboration with infectious disease specialists facilitates guiding and monitoring therapy and decision-making within this complex field. 35
For local antimicrobial therapy different drug delivery systems can be used to achieve a prolonged antibiotic effect. In staged surgical approaches polymethylmethacrylat (PMMA) cement spacers allow for continuous release of antimicrobial agents over a period of multiple weeks. PMMA cement is available preloaded with a range of antibiotics and combinations mainly consisting of gentamicin, clindamycin, and vancomycin and can be supplemented by further heat-stable antibiotic agents depending on the microbial spectrum. 36 For single-stage procedures resorbable materials based on collagen sponges or calcium sulfate pellets are available antibiotic-loaded or can be individually drenched with antimicrobial agents.
Clinical Cases
In the following we outline three cases of our patient cohort with FRI of the proximal femur. The included patients had provided written informed consent for the use of medical data and radiological imaging.
Case 1: Chronic Fracture-Related-Infection After Subtrochanteric Femur Fracture with Two-Staged Therapy
An 85-year-old patient presented to the emergency department following a fall on the right hip. Since the X-rays showed a right subtrochanteric femur fracture surgical intervention was deemed necessary, using a long gamma nail and cerclages (Figure 2, A1, A2). Three months after surgery, the radiological follow-up revealed a cutting-out of the femoral neck screw (Figure 2, B1, B2), accompanied by an enlarged, erythematous right hip, and severe pain. Diagnostic hip puncture identified Enterococcus faecalis infection. A two-staged approach was performed for surgical revision. The first procedure involved implant removal, resection of the right proximal femur, and implantation of an antibiotic-loaded cement spacer (40g Palacos® (Heraeus medical, Wehrheim, Germany) + 2g vancomycin + 2g meropenem) (Figure 2, C1, C2). Ampicillin and ceftriaxone were administered intravenously for a total period of two weeks post-surgery, followed by four weeks of oral antibiotic therapy with amoxicillin and linezolid. Subsequently, the proximal femur was replaced using a MUTARS
Chronic fracture-related infection after subtrochanteric right femur fracture (A1/2). Postoperative X-rays after initial fixation with gamma nail and cerclages (B1/2). Cutting-out of the femoral neck screw after six months required resection of the femoral neck and spacer implantation (C). Postoperative X-rays (D1/2) and radiological three months follow-up (E1/2) after insertion of a megaprosthesis revealed no signs of material failure or secondary fracture.
Case 2: Acute Fracture-Related Infection After Gustilo-Anderson Type I Open Subtrochanteric Fracture of the Left Femur
A 55-year-old patient with a Gustilo-Anderson type I open subtrochanteric left femur fracture underwent treatment through intramedullary nail osteosynthesis. Subsequently, a DAIR (debridement, antibiotics, implant retention) procedure was performed due to an acute infection (Figure 3, A1, A2). Despite these interventions, the patient reported persistent weakness and instability. Eleven months after primary surgery, computed tomography revealed nonunion prompting a one-stage exchange strategy. The procedure involved implant removal, debridement and implantation of allograft (Cancellous Cubes, RTI Surgical, Florida, USA), PerOssal® (Osartis, Muenster, Germany) and CERAMENT® V (Bonesupport, Lund, Sweden) followed by stabilization with a perilock plate osteosynthesis (Smith&Nephew, Hertfordshire, UK) (Figure 3, B1, B2). Empirical antibiotic therapy with ampicillin/sulbactam and vancomycin was administered, adjusted to flucloxacillin and rifampicin based on the sonication results confirming Staphylococcus hominis. Systemic antibiotic medication was applied for a total period of 12 weeks. Four months post-surgery, the patient reported pain in the left thigh during stair-climbing, and X-rays indicated implant failure necessitating revision surgery (Figure 3; C1, C2). The second revision involved implant removal, debridement, and the implantation of a gamma nail (Stryker, Kalamazoo, USA) and an augmentation plate (Locking Compression Plate (LCP), Synthes, Zuchwil, Switzerland). The bone defect was reconstructed using corticocancellous bone of the iliac crest (Figure 3, D1, D2). Follow-up after six months revealed increasing fracture consolidation and non-irritating wound conditions (Figure 3; E1, E2). By the 12-month follow-up, an infection-free consolidation was achieved. Acute fracture-related infection after intramedullary nail osteosynthesis of the left femur. (A1/2) X-rays showing nonunion after former Gustilo-Anderson type I open subtrochanteric left femur fracture treated with intramedullary nailing. (B1/2) Postoperative X-rays after conversion to perilock plate. (C1/2) Implant failure. (D1/2) Postoperative X-rays after second revision combining intramedullary nailing and extramedullary plate fixation. (E1/2) fracture consolidation after 12 months.
Case 3: Necrotizing Fasciitis of the Left Thigh and Concomitant Fracture-Related Infection After Intramedullary Nail Osteosynthesis of an Intertrochanteric Proximal Femur Fracture
A 60-year-old female patient presented to the emergency department following a left hip fall incident. X-rays revealed an intertrochanteric fracture of the left femur. Surgical intervention involved closed reduction and internal fixation (CRIF) using a gamma nail osteosynthesis technique (Figure 4, A). Subsequently, the patient developed significant swelling in the left thigh within a week, and clinical and radiological examination confirmed the presence of a seroma. Evacuation was indicated. During surgery, necrotizing fasciitis was identified (Figure 4, B), prompting removal of the intramedullary nail, thorough debridement, saline irrigation, and treatment of bone and soft tissue with an antiseptic solution Granudacyn® (Mölnlycke, Düsseldorf, Germany). A PMMA-coated rod (Figure 4, D1-3) and k-wires for stabilization (COPAL® G+V (Heraeus medical, Wehrheim, Germany) 40g + 2g vancomycin) were inserted (Figure 4, C). Postoperatively, a combination of meropenem, vancomycin, penicillin G, clindamycin, and fluconazole was administered targeting potential pathogens of necrotizing fasciitis. Methicillin-resistant Staphylococcus aureus (MRSA) and Candida parapsilosis were detected in intraoperative microbiology samples. Necrotizing fasciitis was confirmed by histological examination. Antibiotic therapy was adjusted to vancomycin upon clinical improvement. K-wires and cement spacer were removed after four weeks, followed by insertion of a silver-coated nail (HyProtect®, Bio-Gate, Nürnberg, Germany) (Figure 4, E, F). Linezolid was administered for six weeks post-surgery. Radiological assessment at six-weeks post revision indicated early signs of bone consolidation with infection-free bone healing six months later (Figure 4, G1, G2) Necrotizing fasciitis of the left thigh and fracture-related infection after intramedullary nailing of an intertrochanteric femur fracture. After initial treatment with intramedullary nailing (A1/2). Necrotizing fasciitis was present after four weeks (B). (C1-4) Production of PMMA-coated wire reinforced rod. (D) Postoperative X-ray with PMMA-rod and k-wires by signs of necrotizing fasciitis (E) re-osteosynthesis with custom-made silver-coated nail (F1/2) postoperative X-rays (G1/2) six months radiological follow-up after intramedullary silver-coated nailing demonstrating consolidation.
Conclusion
Patients with FRI of the proximal femur require highly individual therapy in a multidisciplinary approach based on fracture configuration, causative pathogens, and the general physical condition of the patient. The patient’s specific factors have to be taken into account carefully during decision-making and general recommendations can only serve as orientation. For FRI treatment of the proximal femur four therapy concepts are eligible: 1. Implant removal for healed fractures; 2. DAIR procedure for stable osteosyntheses if the fracture is not healed yet and fixation performed by plate; 3. One or multiple staged implant exchange in case of insufficient fracture fixation and for intramedullary fixation devices; 4. (staged) conversion to arthroplasty, if re-osteosynthesis is not feasible. The treatment should always comprise local and systemic antimicrobial therapy. Especially, regarding antibiotic therapy shared decision-making involving infectious disease specialists is recommended.
Footnotes
Author contributions
The idea for the article came from Markus Rupp. The literature search and data analysis were performed by Josina Straub, Nike Walter, Moritz Riedl and Markus Rupp. The article was drafted by Josina Straub, Nike Walter and Moritz Riedl and critically revised by Susanne Baertl, Florian Baumann, Volker Alt and Markus Rupp.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.