
Abstract
Introduction
The COVID-19 pandemic has affected and is still deeply affecting all aspects of public life. World governments have been forced to enact restrictive measures to stem the contagion which have led to a decrease in the movement of people within national territory and to a redirection of health care resources with a suspension of non-urgent procedures. In Italy, a lockdown was imposed from March 9th to May 3rd, 2020. As a result, a significant reduction in the overall operative volume of orthopedic trauma was expected, but it was not possible to predict a similar trend regarding fragility fractures of the proximal femur in the elderly.
Methods
The aim of this paper was to examine the impact of COVID-19 on the operating volume for trauma surgeries and to determine how the pandemic affected the management of fragility hip fractures (FHFs) in non-COVID patients at a single Institution.
Results
The first result was a statistically significant reduction in the overall operative volume of orthopedic trauma during the period of the first lockdown and an increase in the mean age of patients undergoing surgery, as expected. As regard to the second aim, the incidence of FHFs remained almost unchanged during the periods analysed. The population examined were superimposable in terms of demographics, comorbidities, type of fracture, peri-operative complications, percentage of operations performed within 48 hours from hospitalization and 1-year outcome.
Discussion
Our results are in line with those already present in the Literature.
Conclusions
Our study revealed a significant impact of the restrictive anti-contagion measures on the overall orthopedic surgical volume, but, at the same time, we could affirm that the pandemic did not affect the management of FHFs in non-COVID patients, and their results.
Keywords
Introduction
The World Health Organization (WHO), after assessing the severity levels and global spread of the new SARS-CoV-2 infection, declared on March 11th 2020 that the COVID-19 outbreak could be considered a true pandemic. 1 Italy was the first nation to report a case of COVID-19 in Europe and in the first phase of the pandemic it was the country counting the highest number of deaths worldwide, followed by Spain and France (deaths were four times higher than in USA). 2 According to recent WHO estimates, Italy is still one of the countries hardest-hit by the pandemic, being the European country with the second highest absolute number of deaths. 3 This could be explained by the high proportion of elderly people in Italy, 4 who have accounted for most of the victims. In the attempt to contain the contagion, on January 30th, 2020 the Italian government declared a state of emergency and implemented exceptional local preventive measures. Nevertheless, given the rapid spread of the virus, a national lockdown was declared on March 9th, 2020, all over Italy. Within a few weeks, all hospitals in the country redirected health resources to the treatment of patients involved in the pandemic to cope with their growing need for intensive medical care. These numerous and sudden changes affected each hospital ward – including Orthopedics and Traumatology. 2
Orthopedic practice for non-emergent procedures – such as elective surgery and non-urgent outpatients’ consultations – was abruptly discontinued to preserve healthcare resources, whilst all procedures related to sports traumas, motor-vehicle accidents or workplace injuries were nearly eliminated due to imposed restrictions, as predictable. At the same time, domestic injuries remained constant and became the main cause of orthopedic trauma hospitalizations.
As expected, numerous papers1,5-13 reported information in terms of reduced surgical volume during the period of the first lockdown. However, it was not possible to predict a similar trend regarding domestic injuries in general, and fragility hip fractures (FHFs) in particular. The aim of our study was to examine the impact of COVID-19 pandemic on the operating volume for trauma surgeries and to evaluate how FHFs in non-COVID patients during the emergency state were affected in terms of volume, management, outcomes and mortality, compared to the same period of the previous year when COVID-19 was still unknown and to the following year when COVID-19 was still present with less restrictive preventive measures.
Materials and Methods
An observational retrospective study was held at our Institution – Azienda Ospedaliera Universitaria Senese (AOUS) Policlinico Santa Maria alle Scotte, the referral hospital for major traumas over the territory of South-East Tuscany for about 850,000 inhabitants over an area of 11,560 km2, with a population density of 72.5 persons/km2. It also serves as primary hospital for the city of Siena and the surroundings villages, that counts around 120,000 inhabitants in total. Although the number of inhabitants of this area is restricted, the hospital counts more than 30,000 admissions per year, including both ordinary and emergency hospitalizations.
First, the burden of restrictive measures during the first lockdown phase of the pandemic on the operating volume for trauma surgeries was analysed. We defined a “lockdown group” (LG) considering patients who (1) underwent surgery for orthopedic traumas (2) during the first state of emergency (March 9th to May 3rd, 2020). As a “control group” (CG) we considered patients who underwent surgery for orthopedic traumas in the same period of 2019, when SARS-CoV-2 virus was absent. An additional “post-lockdown group” (PLG) was also analysed, including patients who underwent same kind of surgery in the same period of 2021, when SARS-CoV-2 virus was still present but preventive measures were less restrictive. Then, we further assessed non-COVID patients who suffered from FHFs and compared them between the three groups. Inclusion criteria for the groups were: (1) patients aged 65 years or older (2) who underwent surgery for FHFs, (3) were tested COVID-19 negative at their admission to hospital, and (4) remained negative during hospitalization. The collected data of interest included demographics, such as gender distribution and age, patients’ comorbidities, type of fracture (31A and 31B according to AO/OTA classification), peri-operative complications, percentage of operations that have had been performed within 48 hours since hospitalization, and 1-year outcome.
Statistical analysis was performed with the Kruskal Wallis H test, used for continuous parameters, and the Chi-Square test, used for categorical parameters and adjusted according to Yates when the number of total observations was between 40 and 200, as recommended. The significance level was set at p < .05; p was reported as not significant (n.s.) in text and with exact values in Tables. All data were elaborated with XlsStat 2020 software (Addinsoft, New York City, NY) for MS Excel (Microsoft, Seattle, WA, USA).
At our Institution, no Ethical Committee approval is necessary for retrospective studies, and all patients gave their informed consent to data collection and their anonymous use for scientific purposes.
Results
Demographic characteristics of the three groups.

aWhen a statistically significant difference was highlighted (in bold), multiple comparisons have been made to understand which populations differed more.

Graphical illustration of the progression of the number of weekly performed surgical procedures at our Institution during the 2020 lockdown period, compared to 2019 historical series and 2021 “normal pandemic” period.
Of the total surgeries performed in the three periods, considering only patients older than 65 years, those operated on for FHFs were found to be the majority, being 20.6% of the total in 2019, 33.0% in 2020 and 19.2% in 2021 (p = .0435). However, despite the abrupt reduction in the number of interventions for orthopedics traumas in general, the volume of FHFs remained almost unchanged (36 interventions in 2019 vs 28 in 2020 vs 29 in 2021, p = n. s.) (Figure 2). Graphical illustration with column chart of the overall surgical volume of the three periods (2019, 2020 and 2021). Surgical procedures for FHFs are highlighted.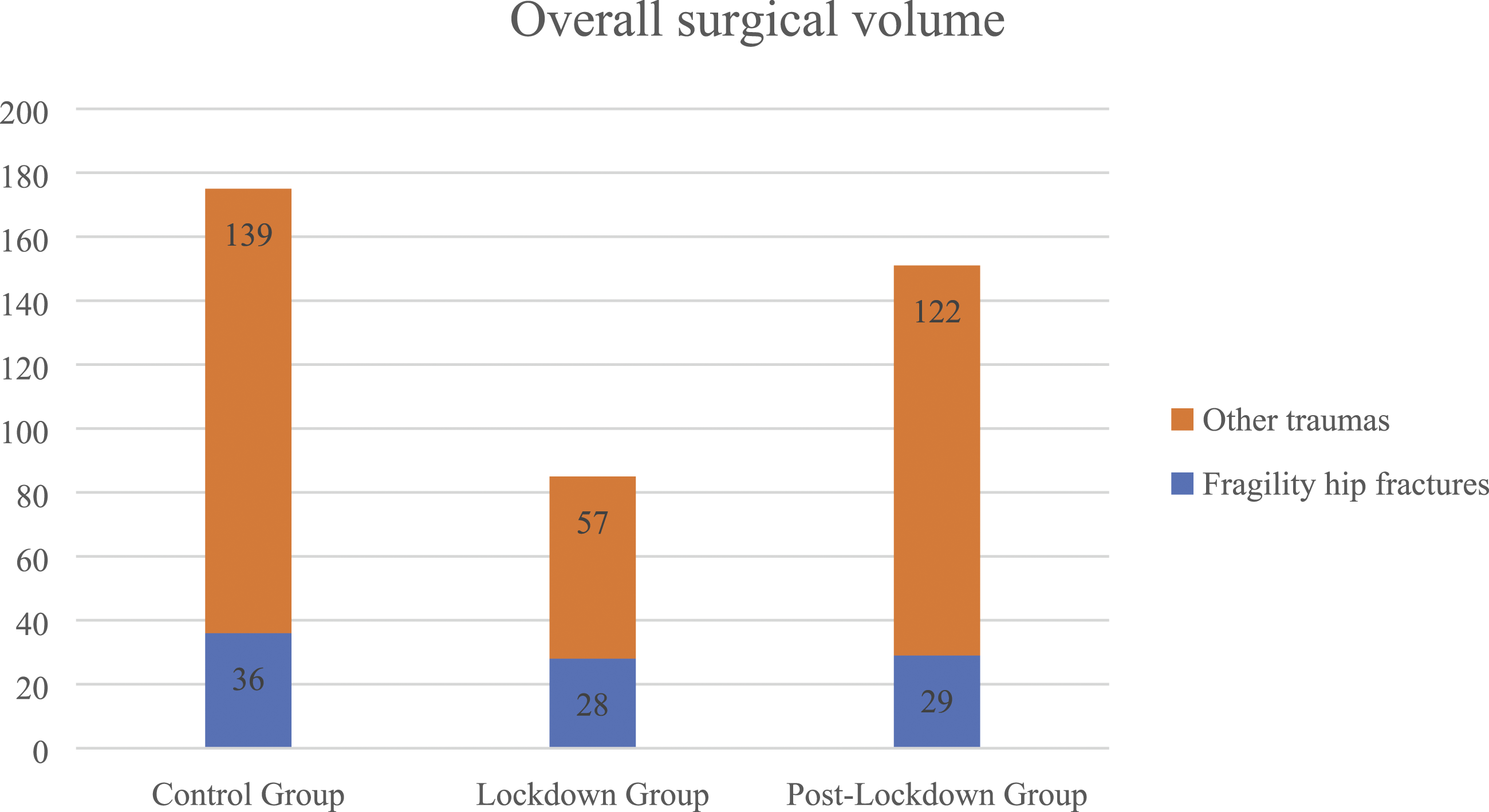
Collected data of interest of the three periods analysed: demographics (gender distribution and age), comorbidities and type of fracture, peri-operative complications, percentage of operations performed within 48 hours from hospitalization and 1-year outcome.

n°.

Comorbidities distribution among patients who underwent surgical procedure for proximal femur fracture.
Type of FHFs was then analyzed according to AO/OTA classification, dividing them into fractures of the trochanteric region (type 31A) and femoral neck fractures (type 31B). Type 31B fractures were further divided into subcapital (type 31B1), transcervical (type 31B2) and basicervical (type 31B3). The ratio of type 31A (fractures of the trochanteric region) to type 31B (femoral neck fractures) remained almost constant in the 3 considered periods. Specifically, 18 type 31A and 18 type 31B (13 subcapital, 2 transcervical and 3 basicervical) fractures were reported in 2019, 14 type 31A and 14 type 31B (8 subcapital, 4 transcervical and 2 basicervical) fractures in 2020, whilst 2021 counted 18 type 31A and 11 type 31B (6 subcapital, 3 transcervical and 2 basicervical) fractures (p = n. s.).
Surgical waiting times – defined as the percentage of patients who were brought to surgery within the 48 hours following hospital admission – recorded during the emergency status compared with those in the 2019 control period and in the 2021 post-lockdown period were superimposable and not statistically different (91.7%, 92.9% and 75.9%, respectively) even if in the post-lockdown period there was a trend to longer surgical waiting time.
Peri-operative complications were analysed as well, especially the need for blood transfusions, performed in 66.7% of patients in 2019, in 64.3% of patients during the lockdown status and in 58.6% of patients in 2021 (p = n. s.). Other complications such as deep venous thromboses (DVTs), pressure ulcers or infections (surgical site infections, pulmonary infections, or urinary tract infections) were detected in 5 (13.9%) patients in the CG, in 3 (10.7%) patients in the LG and in 2 (6.9%) patients in the PLG (p = n. s.).
To evaluate the outcomes of the treatments performed, data regarding return to normal ambulation were collected during follow-up visits. Excluding the deceased subjects, it emerged that almost all the operated patients resumed walking in all the three analysed periods, with or without aids. In 2019, 66.7% of patients resumed walking with aids (axillary walker or classic walking sticks), compared to 33.3% that recovered without the need of any supports. In 2020, the percentages were very similar: 66.7% of patients required aids, 26.7% regained walking without aids and 2 patients (6.7% of the total) switched to the wheelchair after surgery, as dementia prevented adequate cooperation for the proper conduct of physiotherapy, thus affecting functional recovery. In 2021 the percentages were very similar, as well: 41.4% of patients required walking aids, 37.9% recovered without the need of any support, but 6 patients (20.7% of the total) were not able to recover from the fracture (Figure 4). One-year mortality was analysed as well. No statistically significant difference was observed between the three groups in terms of both incidence (35% vs 13% vs 31%) and patients’ mean age (87.8 ± 6.8 vs 84.6 ± 8.8 vs 88.0 ± 6.6 years) in the CG, LG and PLG, respectively. Graphical illustration with column chart of patients’ recovery of walking during the three periods analysed (2019, 2020 and 2021).
Discussion
Over the past two years, an extraordinary health emergency was faced, which has undoubtedly strained health care systems all around the world. The spread of contagion made it necessary to introduce social norms and bans that have revolutionized daily routines: for a long period of time, both recreational and working activities were limited to the essential, centering them in home environment, with a reduction of sports-related, work-related and road traffic-related traumas. At the same time, health care system was forced to redirect hospital resources to meet the increasing demand for intensive care from COVID-19 patients. This resulted in the suspension of all elective surgical activities and nonurgent procedures. In the lockdown period and in the post-lockdown period of the present study, no COVID-positive patients were admitted in our hospital with an orthopedic trauma requiring surgery. This is maybe the result of the very low population density of the surroundings, that may justify rarefied social contact in general and especially for the elderly, with a reduced risk for SARS-CoV-2 infection. The demographic rarefaction could also be the reason why the contagion spread late in our area, while in other parts of Tuscany numbers have been higher impressive since the beginning of the pandemic. Nevertheless, and comprehensibly, even local healthcare was shifted and focused on the pandemic, with a reduction of other activities. Also, post-hospital care was redirected to manage COVID-patients, and post-operative care for operated patients was slowed and somewhat suspended in the lockdown period, as for our Fracture Liaison Service, for example. 14 The aim of this study was to evaluate if this forced unexpected and abrupt re-organization of the healthcare system influenced the management and the recovery of non-COVID patients who underwent surgery for FHFs.
This study confirmed the statistically significant reduction in the overall volume of orthopedic trauma during the period of the first lockdown in Italy. Numerous articles have reported similar results in terms of reduction of operative volume during the lockdown analysed period,1,5-13 for nonsurgical procedures as well. 15 Also, an increase in the mean age of patients undergoing surgery was observed, as already highlighted by Ogazkaya et al 16 and Lv et al. 10 This trend may be explained by the fact that – due to imposed bans and restrictions on travel, sports, working and social activities – high-energy traumas have decreased and consequently the involvement of younger patients. Similar assumptions were made by Kumar et al. 8 This hypothesis seems to have confirmation in the fact that in 2021 a new increase in the overall operating volume accompanied by a statistically significant reduction in patients’ average age was witnessed. Therefore, it can be affirmed that the cause of the drastic reduction of orthopedic traumas is to be found in the restrictions imposed by the Government and not by the SARS-CoV-2 spread by itself. FHFs are mainly due to low-energy domestic traumas, and in the present study their incidence was not affected by the social restrictions associated with COVID-19 pandemic. This result appears to be confirmed by recent papers. Onizuka et al 17 reported how social distancing and travel restrictions reduced the volume of trauma patients in general, whilst the amount of osteoporotic fractures in general, and FHFs in particular, remained constant during the pandemic. These results were confirmed by other studies, as well.1,5,6,8,9,11-13,18-20 However, a significant difference in the prevalence of FHFs in the three periods analysed was observed in the present study. This should be attributed to the abrupt reduction in the number of interventions for traumas related to common injuries, eg road traffic or sports and working injuries, in contrast to the constant volume of domestic traumas.
As concerns surgical waiting times, a reduction was observed in the percentage of patients who were brought to surgery within the 48 hours following hospital admission, even though not statistically significant among the three periods. The greatest difference was observed between the LG and the PLG, probably because a re-normalization in other traumas has occurred at a time when COVID was still present as a major medial concern and healthcare resources (anesthesiologists and nurses, operating room hours) were still preserved to cope with the pandemic.
Regarding patients’ recovery from surgery, the three periods did not substantially differ from each other. However, it emerged that there was a statistically significant difference between non-recovery of walking in the CG and in the PLG. This result could be attributed to the fact that most deceased patients in the PLG died within the first month from surgery, when walking recovery was not yet assessable. It can also be explained by the fact that due to the presence of COVID, an abrupt reduction in postop physical therapy was observed. Rehabilitation institutions were closed or only partially accessible so that most of the patients could not benefit from intensive rehabilitation protocols. One-year mortality in the LG was slightly higher than in the CG and in the PLG, although the difference was found not to be statistically significant. Similarly, Malik-Tabassum et al 18 Onizuka et al 17 and Bilgetekin et al 21 enlightened how 30-days mortality rate after surgery in non-COVID patients was very similar between the two years. However, when comparing COVID-19 positive and negative patients during the pandemic, a significantly higher mortality rate, complications rate and length of hospitalization were observed.18,20 With regards to the statistically non-significant increase in mortality detected in the present study, although it is difficult to prove the direct cause, it is possible that it is related to the higher average age of patients who died during the period of the medical emergency, considering that information about a possible SARS-CoV-2 infection in the months following surgery could not be retrieved for a large number of patient.
Therefore, our study appears to be in line with the results offered by literature, suggesting that COVID-19 pandemic did not affect management and outcomes in non-COVID patients with FHFs during both the lockdown and the medical emergency period.
Limitations are present in this study. First, it is a retrospective study with a limited number of patients: it may be difficult to correctly generalized data obtained because of the small sample size. Secondly, an additional bias could be represented by the fact that during the first lockdown at our Institution no COVID-positive patients experienced a FHFs. This element may have influenced the absence of delay in the management of FHFs.
Conclusions
This study confirmed a significant impact of the COVID-19 pandemic on the overall orthopedic surgical volume. However, no differences between a pre-pandemic historical control group (2019), the lockdown period (2020) and a “pandemic normality” period (2021) regarding the incidence of FHFs were detected, as they were independent of the social restrictions associated with COVID-19; treatment outcomes were not affected by the health emergency either, as functional recovery remained similar in all the three analysed periods.
The sudden reorganization of the health system in the first phase of the COVID-19 pandemic did not adversely affect preoperative management and timing, as the 48-hours rate remained almost unchanged between 2019 and 2020 and 2021 in non-COVID patients. Comorbidities and perioperative complications were also superimposable in terms of need for blood transfusions, bedsores, infections and DVTs. Also, 1-year mortality and functional recovery were found to be overlapping in the three periods.
Ultimately, care-management reorganization during the first lockdown for the SARS-CoV-2 outbreak had no influence on the presentation, treatment nor outcomes of FHFs in patients tested COVID-negative at hospital admission. As lesson learned for future pandemics, at our Institution a plan to modulate medical activities (and dedicated wards) in an accordion-like fashion has been prepared.
Footnotes
Author’s Note
Elisa Troiano and Nicola Mondanelli contributed equally to the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.