
Abstract
Purpose
To determine the relationship between trunk muscle cross-sectional area (CSA) measured using trunk computed tomography at the time of injury and gait ability at discharge.
Methods
This multicenter retrospective cohort study was performed in comprehensive rehabilitation units of four hospitals in Japan. The study included 442 patients with hip fractures who underwent surgery (bipolar hip arthroplasty or open reduction and internal fixation) and were hospitalized for treatment between January 2020 and January 2023. The main outcome measure was bilateral trunk muscle CSA (multifidus, erector spinae, psoas major, lateral abdominal muscles, and rectus abdominis). Participants who met the eligibility criteria were classified into two groups based on gait ability at the time of hospital discharge: those who maintained their gait ability (the maintenance group) and those who declined (the decline group).
Results
The CSA of the multifidus muscle was 0.015 ± 0.005 (CSA/Weight/fourth lumbar vertebrae) and 0.013 ± 0.004 (CSA/Weight/fourth lumbar vertebrae) in the maintenance and decline groups, respectively, being significantly lower in the decline group (P = 0.028, effect size = 0.457). The CSA of the psoas major was 15.3 [13.1–18.0] (CSA/Weight/fourth lumbar vertebrae) and 13.4 [11.9–16.0] (CSA/Weight/fourth lumbar vertebrae) in the maintenance and decline groups, respectively, being significantly lower in the decline group (P = 0.020, effect size = 0.335).
Conclusion
Smaller CSAs of the multifidus and psoas major muscles before injury were associated with decreased gait ability after hip fractures.
Introduction
The incidence of hip fractures (including many secondary fractures such as contralateral hip fractures 1 ) is increasing in Asian countries. 2 Half of secondary fractures occur within the first year after injury; therefore, preventing repeated falls is vital during the postoperative period. 3 Although insufficient recovery of physical function (such as gait ability) may cause repeated falls in the postoperative period, 50% of patients with postoperative hip fractures do not return to their pre-injury gait ability. 4 Therefore, it is important to identify pre-injury physical impairments that affect the recovery of gait ability after hip fractures to prevent further fall-associated fractures.
Lower extremity muscles are atrophied in patients with hip fractures from the pre-injury stage5,6; these muscles are important for improving gait ability after hip fractures.7,8 Another problem associated with hip fractures is that the trunk muscles are atrophied before the injury. 9 Furthermore, atrophy of the trunk muscles affects spinal alignment. 10 Trunk muscle strength and thickness are associated with balance and gait speed in older adults.11,12 In addition, dynamic balance affects gait modality. 13 However, the relationship between pre-injury trunk muscle atrophy and the return to the pre-injury gait modality in patients with hip fractures remains unclear.
We hypothesized that patients with hip fractures with a small cross-sectional area (CSA) of the trunk muscles before injury have decreased gait ability after surgery. Therefore, this study aimed to determine the relationship between trunk muscle CSA and spinal alignment using trunk computed tomography (CT) at the time of injury and gait ability at discharge.
Methods
Study Design and Settings
This multicenter retrospective cohort study was conducted in four Japanese hospitals with comprehensive rehabilitation units and in accordance with the guidelines of the Declaration of Helsinki and the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE). The study protocol was reviewed and approved by the Ethics Committee of our institution. Informed consent was obtained in the form of opt-out on the website or notice board of each hospital included in the study.
Study Participants
The study included 442 patients with hip fractures who underwent surgery (bipolar hip arthroplasty or open reduction and internal fixation) and were hospitalized for treatment between January 2020 and January 2023. The exclusion criteria were (1) under 65 years of age, (2) discharged early without undergoing rehabilitation in a comprehensive rehabilitation unit, (3) hemiplegia due to stroke, (4) gait difficulty before surgery, (5) cut-outs after surgery, and (6) without CT imaging of the lumbar spine. Participants who met the eligibility criteria were classified into two groups based on gait ability at the time of hospital discharge: those who maintained their gait ability (the maintenance group) and those who declined (the decline group). Gait ability was defined based on gait modality (no device, T-cane, or walker). The preliminary analysis of spinal alignment involvement included only participants with CT of the thoracolumbar spine. In addition, the participants received standard physiotherapy twice a day (total, 80-120 min), including joint range of motion exercises, strength training, and gait training.
Outcomes and Measurements
The main outcomes were bilateral trunk muscle CSA (multifidus, erector spinae, psoas major, lateral abdominal muscles, and rectus abdominis), vertebral body CSA of the fourth lumbar vertebra, thoracic kyphosis angle, and lumbar kyphosis angle. Data on basic characteristics, such as age, sex, height, weight, body mass index, fracture type (femoral neck fracture/trochanteric fracture), gait ability (gait ability before injury / gait ability at time of discharge), and the duration of hospital stay, were collected from electronic medical records and from interviews of the participants or their families at the start of rehabilitation.
Measurement of the CSA of Trunk Muscles
The muscle CSA of the trunk was identified from CT axial images at the level of the fourth to fifth lumbar vertebrae based on a previously described method.
14
CT scans were performed immediately after the injury (before surgery) using SOMATOM Force VB30 (SIEMENS; tube voltage, 90 kV; tube current, 600 mA; slice thickness, 3 mm; field of view, 350 mm; matrix size, 512 × 512 pixels), SOMATOM go. Top (SIEMENS; tube voltage, 120 kV; tube current, 113 mA; slice thickness, 3 mm; field of view, 598 mm; matrix size, 512 × 512 pixels), Aquilion Prime (Canon; tube voltage, 120 kV; tube current, 113 mA; slice thickness, 3 mm; field of view, 598 mm; matrix size, 512 × 512 pixels), Aquilion Prime SP (Canon; tube voltage, 120 kV; tube current, 320 mA; slice thickness, 3 mm; field of view, 320 mm; matrix size, 512 × 512 pixels), and Aquilion Prime (Canon; tube voltage, 120 kV; tube current, 130 mA; slice thickness, 3 mm; field of view, 150 mm; matrix size, 512 × 512 pixels). Participants were assessed in the supine position, with their spine and pelvis in the neutral position. Each muscle CSA was manually measured by four authors (physiotherapists with at least 8 years' experience) at different centers using a measurement tool (RapideyeCore
1
, XTREK WebView
2
, Plissimo EX
3
, SYNAPSE Enterprise-PACS
4
) and included in the electronic medical record (Figure 1A). The CSA of the fourth vertebral body was measured from an axial image at the level of the fourth lumbar vertebra (Figure 1b).
15
Reliability of trunk muscle CSA measurement was calculated using CT data from 10 participants (three males and seven females, mean age: 86.0 ± 6.6 y, height: 151.9 ± 7.8 cm, weight: 48.1 ± 9.3 kg), with each examiner taking two measurements, and intra-examiner reliability was calculated. In addition, inter-rater reliability was calculated using the data measured once by each examiner. The intra-examiner intra-class correlation coefficient was 0.9 or higher for each muscle and vertebra, and the inter-examiner intra-class coefficient was 0.85 or higher, confirming high reliability. Measurement of the cross-sectional area (CSA) of trunk muscles and vertebral body. Axial CT images at the level of the fourth to fifth (a) and fourth (b) lumbar vertebrae. Regions of interest were set at the trunk muscles (a) and fourth lumbar vertebrae (b). CSA, cross-sectional area; CT, computed tomography; ES, erector spinae muscles; LA, lateral abdominal muscles; MF, multifidus muscles; PM, psoas major muscles; RA, rectus abdominal muscle.
Measurement of Spinal Alignment
Sagittal images were reconstructed from axial images of the thoracolumbar spine using ImageJ software version 1.53
5
. The kyphosis angle of the thoracic spine and the lordosis angle of the lumbar spine were measured according to previously described methods (Figure 2).
16
Measurement of spinal alignment. Sagittal computed tomography images at the midline. The angle between the superior endplate of T5 and the inferior endplate of T12 was used to measure thoracic kyphosis. Lumbar lordosis was measured as the angle between the superior endplates of L1 and S1. L, lumbar; LL, lumbar lordosis; S, sacrum; T, thoracic; TK, thoracic kyphosis.
Statistical Analysis
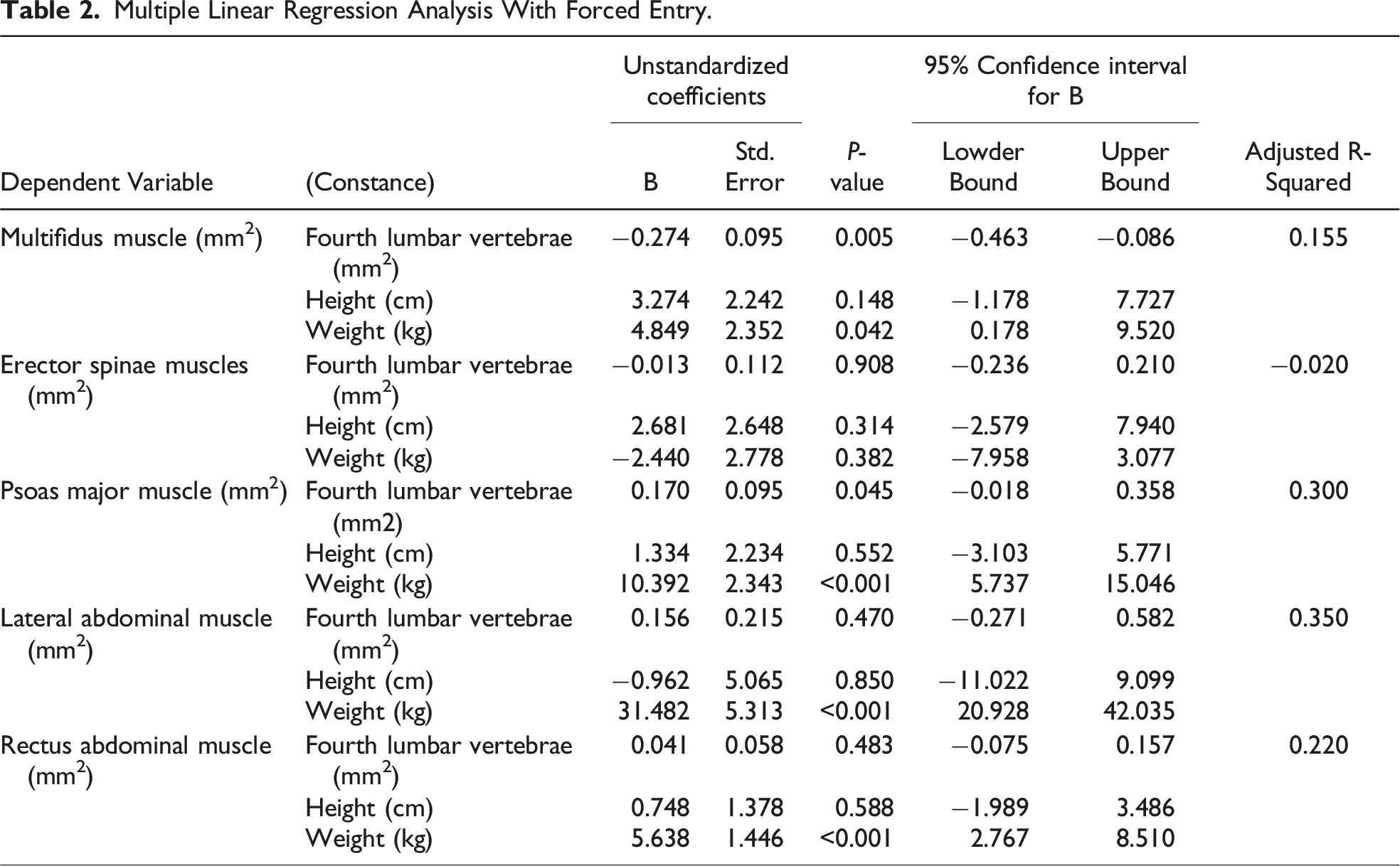
All statistical analyses were performed using SPSS Version 27.0 6 . The normality of each data point was tested using the Shapiro–Wilk normality test. To normalize the muscle CSA, multiple linear regression analysis with forced entry was performed to identify relevant factors related to the CSA of each trunk muscle divided by the associated factor. To determine the difference between the left and right trunk muscle CSAs, differences in trunk muscle CSA between the unaffected and affected sides were compared using the unpaired t test or the Mann–Whitney U test. Baseline characteristics, muscle CSA and spinal alignment of the maintenance and decline groups were compared using the unpaired t test, Mann–Whitney U test, and chi-squared test. The effect size was calculated to compare the two groups for each muscle CSA. Statistical significance was set at P < 0.05. In addition, a post hoc power analysis was conducted for each significant result for CSA using G* Power 3 Software (version 3.1.9.4) 7 to determine whether there was sufficient power to detect statistically significant effects given the available sample sizes.
Results
Classification and Baseline Characteristics of Participant Groups
A flowchart of the study is shown in Figure 3. The study included 96 participants who met the eligibility criteria (mean age, 84.7 ± 6.9 y; height, 152.7 ± 9.7 cm; weight, 47.3 ± 9.0 kg; sex, 25 males and 71 females; fracture type, 53 femoral neck and 43 trochanteric fractures). The patients were categorized into two groups based on whether they maintained their pre-injury gait modality at the time of discharge, with 49 in the maintenance group and 47 in the decline group. Preliminary analysis of spinal alignment included 31 participants who met the eligibility criteria (mean age, 84.6 ± 6.9 y; height, 152.7 ± 9.7 cm; weight, 47.4 ± 9.0 kg; sex, 13 males and 18 females; fracture type, 19 femoral neck and 12 trochanteric fractures). Of the 31 participants, 17 were included in the maintenance group and 14 were in the decline group. In both analyses, baseline characteristics differed significantly between the groups only in gait ability (Table 1). No differences were observed in the CSA of each muscle between the left and right sides. Therefore, only the muscle CSA of the affected side was presented in the following results. Multiple regression analysis showed that body weight was the selection variable for all muscles, except for the erector spinae (Table 2). In addition, the multifidus and psoas major muscles were selected for the fourth cross-section of the lumbar vertebral body (Table 2). Study flowchart. Basic Characteristics of the Participants. *Mean ± standard deviation, median [lower quartile – upper quartile]. aIn total, 96 patients were categorized into the maintenance and decline groups for comparison. The 31 participants in the preliminary analysis were categorized into the maintenance and decline groups, and baseline characteristics and spinal alignment were compared between the two groups. Multiple Linear Regression Analysis With Forced Entry.

Comparison Between the Two groups
Comparison of the Cross-Sectional Area of the Two Groups of Trunk Muscles.
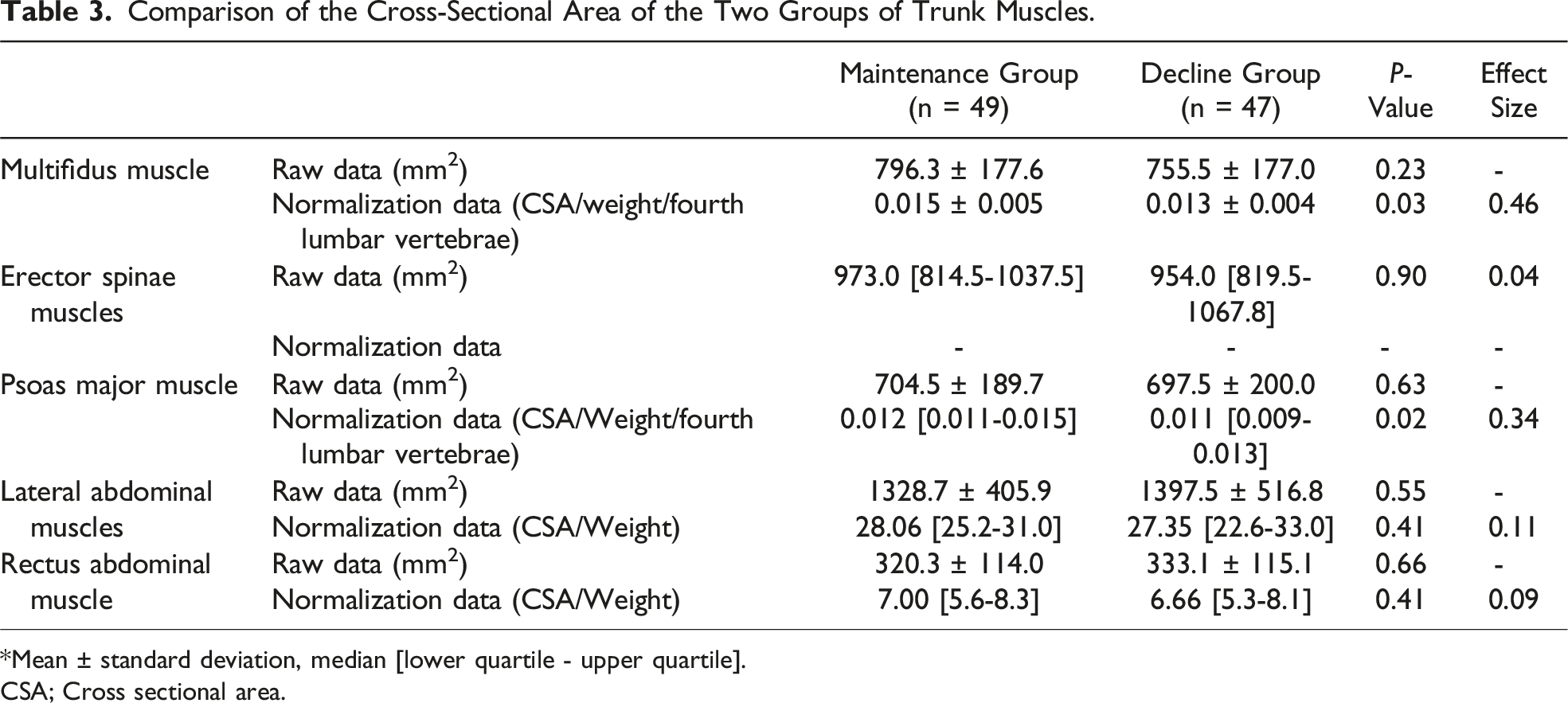
*Mean ± standard deviation, median [lower quartile - upper quartile].
CSA; Cross sectional area.
Discussion
This study showed that the patients in the decline group who were unable to return to pre-injury gait ability had significantly smaller pre-injury CSA for the multifidus and psoas major muscles than did the patients in the maintenance group, regardless of supine spinal alignment.
Although lumbar kyphosis alignment and lumbar extensor CSA have been shown to be related in healthy people in the supine position, 17 the results for hip fractures in this study were differed. Trunk muscle atrophy has been reported after surgery for hip fractures. 14 In addition, patients with poor improvement in gait ability after a hip fracture have low scores on the Trunk Control Test, an assessment of trunk control and function. 18 Previous studies mainly focused on trunk muscle atrophy and function after hip fracture. This study revealed that the pre-injury CSA of the trunk muscles may affect the maintenance of postoperative gait modality and requires an evaluation of trunk muscle impairment after hip fracture.
The alignment of the lumbar spine in the supine and standing positions in healthy participants showed no difference. 19 The multifidus and psoas major muscles are important for maintaining lumbar lordosis in the antigravity position.12,20 Older hip fractures may have been affected by postural changes. Lumbar kyphosis alignment is associated with decreased dynamic balance. 21 Because dynamic balance is associated with different gait modalities, 13 atrophy of the multifidus and psoas muscles, as observed in this study, may be associated with a decreased gait modality at the time of discharge from the hospital. Furthermore, atrophy of the psoas muscle affects lower-limb swing and decreases foot clearance during gait. 22 These results suggest the importance of the multifidus and psoas muscles with regard to the return of the pre-injury gait modality after a hip fracture.
The multifidus and psoas major muscles are associated with decreased gait ability after hip fractures. Conventionally, after hip fractures, physical therapy for the lower extremities is a commonly used intervention23,24; however, the need for intervention for the trunk muscles has been suggested. Interventions for trunk muscles may increase the rate of return to pre-injury gait modality.
Study Limitations
This study investigated the trunk muscle CSA only once at the time of injury. Therefore, changes in the trunk muscle CSA during hospitalization remain unclear. Furthermore, the effects of the trunk muscle CSA on spinal alignment and dynamic balance in the anti-gravity position remain unclear. In addition, gait assessment was limited to examining gait modalities. Although there was a significant difference in the statistical P-values, the effect sizes were all <0.5, which may not have sufficient statistical power. Future studies should consider sample size and use multivariate analyses to examine associations between outcomes. In addition, changes in the trunk muscle CSA during hospitalization should be investigated to assess spinal alignment in the antigravity position, assess its association with dynamic balance, and quantitatively assess gait speed. The problem lies in the development of a trunk muscle training program that can be performed in older patients with hip fractures.
Conclusions
This study revealed a relationship between the trunk muscle CSA using trunk CT at the time of injury and gait ability at discharge. Smaller CSAs of the multifidus and psoas major muscles before injury were associated with a decrease in gait ability after a hip fracture. These results suggest the importance of trunk muscle intervention in addition to lower extremity intervention in postoperative hip fracture rehabilitation.
Footnotes
Author Contributions
Conceptualization, K.K. and S.K.; methodology, K.K., S.K., and M.T.; validation, K.K. and S.K.; formal analysis, K.K.; investigation, K.K., D.F., N.K., M.T., and M.Y.; resources, K.K. and S.K.; data curation, K.K.; writing—original draft preparation, K.K.; writing—review and editing, K.K.K., M.T., S.M., and S.K.; visualization, K.K. and M.T.; supervision, S.K.; project administration, K.K. and S.K.; funding acquisition, S.M. and S.K. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study was supported by the Morinomiya University President’s Research Encouragement Award (Grant Number: 2023MPA2) and the JSPS KAKENHI (grant number JP 24K20550).