
Abstract
Keywords
Introduction
The prevalence of hip fracture is growing as our population ages, with global predictions of 6.3 million hip fractures/year by 2050. 1 Hip fractures, common in older adults, are associated with increased mortality risk 2 and often lead to decreased quality of life and independence. 3
Structured rehabilitation can improve outcomes after hip fracture.4-10 Evidence on rehabilitation impact is often limited due to heterogeneity of rehabilitation program content coupled with poor reporting of specific intervention parameters (e.g., intervention timing, duration, intensity, setting, etc.). These limitations make it difficult to discern which rehabilitation intervention components may produce maximal benefits for patients; understanding which intervention components maximize patient outcomes is paramount as many hip fracture patients do not return to pre-fracture functional levels.3,11
Recent systematic reviews with meta-analyses demonstrate the impact of such intervention heterogeneity on determination of rehabilitation impact; these recent reviews,4,6,7,10,12,13 which were performed at similar time points, included different trials despite having similar aims. While all meta-analyses consistently demonstrated that exercise early after hip fracture can improve patient outcomes, most provided little guidance on the types of exercise that should be offered to patients to augment recovery; this information is needed so that clinicians develop rehabilitation programs that can maximize benefits for patients.
Diong et al. and Zhang et al. included meta-regression, a statistical technique that examines associations between study level characteristics (rather than participant level) 14 and study outcomes to try to identify program components associated with better outcomes.6,7,13 Both evaluations found that including progressive resistance training programs in rehabilitation interventions improved patient outcomes after hip fracture. However, to date, there has been no attempt to systematically explore specific resistance training program characteristics associated with improved functional recovery after hip fracture, such as timing of the intervention, duration of program, and the frequency, intensity and type of resistance exercises performed, including equipment used. Understanding the impact of progressive resistance training components could improve the design and delivery of future rehabilitation programs for hip fracture patients to improve outcomes.
Therefore, the purpose of this systematic review with meta-analyses was to a) evaluate reported resistance training program parameters in randomized controlled trials that compared progressive resistance training programs after hip fracture to usual care or programs without progressive resistance training, b) perform meta-analysis to investigate if resistance training programs influenced rehabilitation outcomes (strength [primary outcome], gait and physical activity [secondary outcomes]), and c) explore if specific progressive resistance training program components were associated with improved strength, gait and physical activity using meta-regression where appropriate.
Materials and Methods
The protocol was registered in the PROSPERO database (https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42018111803).
Search Strategy and Literature Sources
Medline, EMBASE, CINAHLPLUS, and Web of Science Core Collection databases were searched for randomized controlled trials published between January 2000 and February 2021. The search combined the concepts of hip fracture, exercise programs, and outcomes of interest (strength, gait, physical activity). Within concepts, searches for synonyms were conducted using the OR operator before combining concepts using AND. (see full search strategy Supplemental File 1).
Eligibility Criteria
Trials were selected using the following inclusion criteria: 1) randomized controlled trials; 2) participants aged 50 years or older; 3) participants undergoing surgery for hip fracture; 4) compared a progressive resistance training intervention to usual care (or an intervention without progressive resistance training); 5) reported at least some details of the resistance training intervention (i.e., timing of intervention initiation, program duration, frequency of sessions, progressive resistance training intensity, setting [home vs center]; progressive resistance training equipment used [machine vs weights/bands or bodyweight]); 6) included strength, gait, and/or physical activity outcomes and 7) were published in English.
Two independent reviewers screened the titles and abstracts as well as the full texts according to standardized criteria. For disagreements during the selection process, a third reviewer was consulted to facilitate consensus. Study selection was performed using Covidence, an online-tool developed for systematic reviews by the Cochrane Collaboration that follows the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. 15
Quality Assessment
Quality assessment of included trials was performed using the validated PEDro scale.16,17 Trials were considered moderate to high quality when the final score was 5 or higher. Two independent assessors evaluated the quality of included articles with a third reviewer consulted to facilitate consensus when needed.
Data Extraction
The included trials were individually reviewed with the study details extracted (i.e., sample size, participant age, sex, outcome/outcome measures, and assessment time points) as well as reported intervention characteristics (i.e., treatment setting, intervention initiation time, equipment type, intensity, number of sessions, and duration) and outcomes (i.e., strength, gait, physical activity).
Statistical Analysis
Knee or leg extension strength was used as the representative strength measure as it was most commonly reported. For trials reporting both measures, knee extension was selected. Gait speed, timed up and go (TUG) test, and 6 minute walk tests (6MWT) were the gait measures. For trials with multiple gait measures, separate analyses were conducted on each measure (gait speed, TUG, and 6MWT). Further, separate analyses were performed for assessments conducted immediately after program completion and those conducted as additional follow ups subsequent to program completion.
Standardized mean difference (effect size) based on Hedges’ g method was used based on sample sizes available at post-intervention assessments. Conventional (Frequentist method) as well as Random-effects Bayesian meta-analytic methods were used to examine the immediate effects of progressive resistance training on strength and gait measures as well as longer-term impact of the programs when extended follow-up assessment was reported. For Bayesian meta-analysis, normal distribution was defined as the priors for the true pooled effect size and Half-Cauchy distribution was defined as the priors for the between-study heterogeneity. N = 5,000 was used as the total number of iterations for Markov Chain Monte Carlo (MCMC) simulation based on Gibbs sampler. Statistical analysis was performed using SAS (Version 9.4), IBM SPSS Statistics (Version 25), and R-package (Version 3.5.0) as analytic tools.
To consider variation in outcomes among studies (heterogeneity), we used random-effects approach which allows the study outcomes to vary in a normal distribution between studies. The I2 statistic with 95% confidence interval was examined to understand the variation across studies that was due to heterogeneity rather than chance.
Outcomes immediately after intervention completion were explored further using either univariate linear meta-regression (continuous variables with a continuous outcome) or subgroup analysis with Mixed-Effects Model (categorical variables with a continuous outcome) when there were a minimum of 10 trials for the outcome of interest. When reported, we explored associations between the outcomes and the following resistance training characteristics: (1) Intervention setting—analyzed as a dichotomous variable of center-based (e.g., hospital, outpatient clinic, research lab, senior gym) vs home-based setting. (2) Time between surgery and initiating the intervention—analyzed both as a continuous variable (in weeks) and a categorical variable. Interventions were categorized as early-initiating (commencing <8 weeks after surgery), mid-initiating (commencing 8–24 weeks after surgery) and late-initiating (commencing >24 weeks after surgery). (3) Type of progressive resistance equipment used—analyzed as a dichotomous variable of machine vs other equipment (i.e., resistance bands, weights, and sand bags). (4) Progressive resistance training intensity—analyzed as a continuous variable. (5) Progressive resistance training intensity prescription—analyzed as a dichotomous variable based on percentage of one-repetition maximum or other methods (i.e., constant weight, 8 or 10 repetition maximum, and perceived exertion) (6) Number of exercise sessions—analyzed as a continuous variable. (7) Duration of intervention (in weeks)—analyzed as a continuous variable.
Univariate meta-regression was performed only on strength and gait speed assessed immediately after completion of the training programs as these were the only parameters with adequate numbers of trials to perform a meta-regression. Physical activity measures were not included in the meta-analyses or meta-regression due to substantial heterogeneity and limited number of included studies assessing this outcome.
Results
Search Results
The search identified 1289 references, with 655 duplicates subsequently excluded. After duplicates were removed, 2 independent reviewers evaluated the remaining 634 abstracts, excluding 582 that did not meet the eligibility criteria. The full-text of the remaining 52 trials were then assessed with 35 trials excluded (Figure 1). Data were extracted for the remaining 17 trials followed by quality assessment. PRISMA diagram of search results.
Study Characteristics and Methodological Reporting
Characteristics of included studies.

TUG, Timed up and go test; 6MWT, 6 minute walk test; * shows the outcomes that are included in the analysis; †data obtained directly from the author.
Overall, there were 9 center-based interventions5,18-25 and 7 home-based interventions;9,26-31 (1 was undefined 32 ). Six interventions initiated before 8 weeks postoperatively,18,19,21,29-31 5 initiated between 8 and 24 weeks postoperatively5,22,24,26,27 and 6 initiated after 24 weeks postoperatively.9,20,23,25,28,32
Characteristics of the interventions.

RM: Repetition maximum.
Strength Meta-analysis
Of the 17 trials, two did not measure strength.29,31 Meta-analysis on strength was conducted with 10 trials (n = 728 participants) that measured knee or leg extension strength.5,9,18-23,26,30 Results from Conventional (Frequentist) meta-analysis found a significant increase in strength measures in the intervention relative to control group immediately after the intervention (Standardized Mean Difference (SMD) [95% CI] .40 [.02, .78]; Heterogeneity: I2 = 73%, τ2 = .22, P < .01) (Figure 2).5,9,18–23,26,30 Meta-analysis on 5 trials (n = 384) with follow-up assessments (Mean ± Standard Deviation (SD): 14.0 ± 5.7 weeks after completion of the intervention) suggested that the greater improvement in strength in the intervention relative to control group was not maintained (SMD [95% CI] = .47 [-.28, 1.23]; Heterogeneity: I2 = 81%, τ2 = .28, P < .01) (Figure 2).9,18,21,26,30 Bayesian meta-analysis method demonstrated similar findings (see Supplementary File 1-Figure 1). Forest plots of immediate and long-term effects of resistance training on muscle strength and gait speed (conventional [Frequentist] meta-analysis); (a) immediate effect of resistance training on muscle strength; (b) immediate effect of resistance training on gait speed; (c) long-term effect of resistance training on muscle strength; (d) long-term effect of resistance training on gait speed.
Five trials were not included in the meta-analysis.24,25,27,28,32 Mangione et al. (2005, 2010) reported on total isometric force of lower extremity using a manual grading system.27,28 Mangione et al. (2005) showed greater improvement in strength in the intervention groups compared to the control group. 27 In Mangione et al. (2010), strength improved significantly in the intervention group both immediately after completion of the training program and at 1-year follow-up. 28 Sylliaas et al. (2011, 2012) used the sit-to-stand test and maximum step high test to measure strength and reported significant improvements in intervention relative to control groups.24,25 Wu et al. (2020) did not include standard deviation, so was excluded from the meta-analysis, but they did report significant increase in knee-extensor maximum voluntary isometric contraction force after the intervention with no significant change in control group. 32
Gait Meta-analysis
Of the included 17 trials, 3 did not measure gait outcomes.9,29,31
Gait Speed
Ten trials (n = 704 participants) were included in the gait speed meta-analysis.5,18,21,23-28,30 Results from Conventional (Frequentist) meta-analysis found a significant increase in gait speed in the intervention relative to control group immediately after the intervention (SMD [95%CI] = .42 [.08, .76]; Heterogeneity: I2 = 65%, τ2 = .17, P < .01) (Figure 2).5,18,21,23–28,30 Meta-analysis on 5 trials (n = 240) with follow-up assessments (Mean ± SD: 14.4 ± 5.5 weeks after program completion) indicated that the greater change in gait speed in the intervention relative to control group was not maintained (SMD [95%CI] = .6 [-.26, .38]; Heterogeneity: I2 = 0%, τ2 = .028, P = .61) (Figure 2).18,21,26,28,30 Bayesian meta-analysis method demonstrated similar findings (Supplementary File 1-Figure 1).
Timed up and go (TUG)
7 trials (n = 500 participants) were included in the TUG meta-analysis.18-22,24,25 Results from Conventional (Frequentist) meta-analysis found no significant change in the TUG in the intervention relative to control group immediately after the intervention (SMD [95% CI] = .26 [-.32, .85]; Heterogeneity: I2 = 86%, τ2 = .33, P < .01) (Supplementary File 1-Figure 2).18–22,24,25 Meta-analysis on 2 trials (n = 68 participants) with follow-up assessments (Mean ± SD: 11.0 ± 1.4 weeks after program completion) also did not show any changes in TUG results in the intervention relative to control group (SMD [95% CI] = .13 [-.92, 1.18]; Heterogeneity: I2 = 0%, τ2 = .0008, P = .73) (Supplementary File 1-Figure 2).18,21 Bayesian meta-analysis method demonstrated similar findings (Supplementary File 1-Figure 3). Forest plots of subgroup analysis using the Mixed-Effects Model (random-effects model within subgroups, fixed-effects model between subgroups); (a) immediate effect of resistance training on muscle strength by program setting (center-based vs home-based); (b) immediate effect of resistance training on gait speed by program setting (center-based vs home-based); (c) immediate effect of resistance training on muscle strength by intensity prescription based on %RM (yes vs no); (d) immediate effect of resistance training on gait speed by intensity prescription based on %RM (yes vs no).
Six minute walk test (6MWT)
6 trials (n = 540 participants) were included in the 6MWT meta-analysis.22,24-28 Results from Conventional (Frequentist) meta-analysis showed that there was no significant change in the 6MWT in the intervention relative to control group immediately after the intervention (SMD [95%CI] = .16 [-.34, .67]; Heterogeneity: I2 = 80%, τ2 = .16, P < .01) (Supplementary File 1-Figure 2).22,24–28 Meta-analysis on 2 trials (n = 145 participants) with follow-up assessments (Mean ± SD: 19.0 ± 7.1 weeks after program completion) also did not show any changes in 6MWT results in the intervention relative to control group (SMD [95% CI] = .15 [-3.77, 4.06]; Heterogeneity: I2 = 53%, τ2 = .11, P = .14) (Supplementary File 1-Figure 2).26,28 Bayesian meta-analysis method demonstrated similar findings (Supplementary File 1-Figure 3).
Wu et al. (2020) was excluded from the meta-analysis because they did not report means or standard deviations; they reported no significant change in 6MWT distance in either intervention or control group. 32
Physical Activity
Only 3 studies reported physical activity measures; no meta-analysis was performed due to heterogeneous data. Hauer et al. (2002) used a physical activity questionnaire to assess the efficacy of high intensity progressive resistance training after hip surgery. They found significant improvements in physical activity in the intervention group relative to control, but some of these improvements were not maintained after intervention completion. 18 In a study by Orwig et al. (2011), participants in a year-long home-based progressive resistance exercise program reported spending more time in exercise behavior and more energy over the course of the program. 29 Turunen et al. (2017) examined the effect of a year-long home-based rehabilitation program including progressive resistance training on the participants’ physical activity. Findings indicated that there was an increase in the number of patients who engaged in moderate to heavy physical activity in the intervention group compared with the control group. 31
Strength Meta-regression
In 7 of 10 trials reporting strength measures, progressive resistance training was center-based,5,18-23 with the remaining 3 conducted in home settings.9,26,30 In 4 trials, the intervention started early after surgery (<8 weeks),18,19,21,30 while intervention initiation time was 8–24 weeks after surgery in 3 trials5,22,26 and >24 weeks in 3 trials.9,20,23 6 trials used resistance machines for training18,20,22,23,26 while the remaining 4 trials used other equipment (resistance bands, weights, or sand bags).9,19,21,30 Progressive resistance intensity was prescribed based on percentage of one-repetition maximum in 6 trials5,18,20-23 with the remaining 4 using constant weight, perceived exertion, 8 or 10 repetition maximum.9,19,26,30
Associations between the progressive resistance training program characteristics and outcomes (continuous) immediately after completion of the training programs.
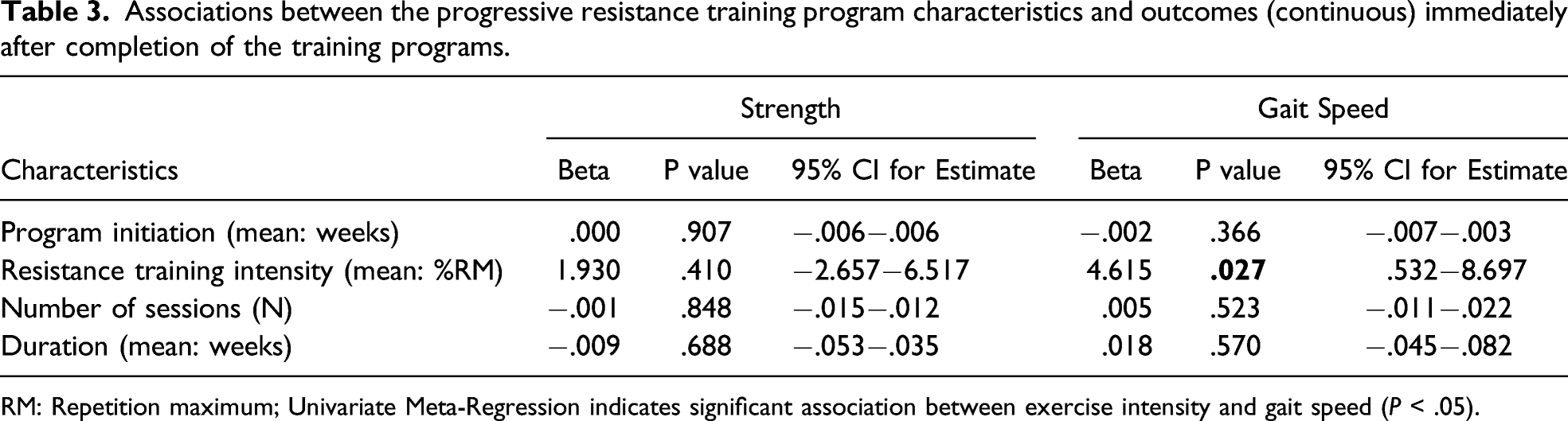
RM: Repetition maximum; Univariate Meta-Regression indicates significant association between exercise intensity and gait speed (P < .05).
Gait Speed Meta-regression and Mixed-Effects Model
In 6 of 10 trials reporting gait speed, progressive resistance training was center-based,5,18,21,23-25 with the remaining 4 conducted in home settings.26-28,30 In 3 trials, the intervention started early after surgery (<8 weeks)18,21,30 while the intervention initiation time was 8–24 weeks after surgery in 6 trials5,24-28 and >24 weeks in 1 trial. 23 6 trials used resistance machines for training,5,18,23,26-28 whereas 4 others used other equipment (weights or sand bags).21,24,25,30 Progressive resistance training intensity was prescribed based on percentage of one-repetition maximum in 8 trials5,18,21,23-25,27,28 while the remaining trials used constant weight or 8 repetition maximum.26,30
Univariate meta-regression analysis showed that higher progressive resistance training intensity was significantly associated with greater improvements in gait speed immediately after program completion (P < .05, Table 3). There were no significant associations between the intervention initiation time, number of exercise sessions, or duration of intervention with gait speed immediately after completion of the interventions (Table 3). Subgroup analysis with Mixed-Effects Model showed no significant difference in change in gait speed based on intervention setting (center vs home) (P = .20), progressive resistance training intensity prescription (% of one-repetition maximum vs other) (P = .74; Figure 3), intervention initiation (Early vs Mid vs Late) (P = .35), or type of equipment used (resistance machine vs others) (P = .64; Supplementary File 1-Figure 4).
Discussion
This meta-analysis found that progressive resistance training as part of a rehabilitation program is highly heterogeneous in terms of timing of initiation, setting, and duration. The frequency and intensity of these interventions and the type of resistance equipment used was also variable. Further, it is essential that rehabilitation programs define the program components being offered, so that the impact of specific components as well as their interaction can be evaluated to determine the overall impact on patients’ recovery. Despite the substantial number of systematic reviews and meta-analyses performed on rehabilitation or exercise after hip fracture,4,6,7,10,12,13 we were only able to find 17 trials that reported specifically on progressive resistance training programs and their parameters. Our findings support the use of the TIDieR guidelines in future randomized trials to facilitate improved reproducibility of interventions. 33
Despite this marked heterogeneity, similar to others,6,7,13 our meta-analysis found that progressive resistance training improved both strength and gait speed relative to usual care or comparison interventions that did not include progressive resistance training programs. Although our meta-regression was exploratory and should be interpreted with some caution, we identified progressive resistance training components worthy of further investigation to maximize improvements in strength and gait speed after a hip fracture. Specifically, progressive resistance training intensity prescription based on percentage of one-repetition maximum appears to be more effective for improvements in strength than other methods of exercise intensity prescription while higher intensity programs also improved gait speed. Superiority of higher vs lower intensity progressive resistance training to improve strength has been reported previously. 34 Center-based programs also appeared superior to those conducted in home settings in improving strength. This might be related to more intensive supervision and exercise compliance in center-based vs home-based programs. Lower levels of supervision in home-based programs may result in lower adherence to the prescribed intensity, or even completion of program components. Participants might also be apprehensive about exercising independently in their homes after a hip fracture, which might slow their progression or completion of the exercises.
The greater improvements in both strength and gait speed in the intervention relative to control group appeared to be mitigated within an average of 14 weeks after participants completed the formal rehabilitation program. This might be attributed to the small number of trials (n = 5; 384 participants) with follow-up assessments that continued beyond the intervention as the intervention groups continued to show higher mean strength values in the long term in 4 of the 5 trials with follow-up assessments on strength measures,9,18,21,30 but our findings were not statistically significant. Thus, our analysis on the long-term impact of progressive resistance training on strength is likely under-powered.
Similar findings were seen with gait speed, which improved immediately after completion of the progressive resistance training program, but the achieved gains in the intervention relative to control group were also mitigated over time. Again, our results should be interpreted with caution due to the small number of trials (n = 5; 240 participants) that performed extended follow-up evaluations. Future trials should consider longer-term follow-up to determine if the positive impact of progressive resistance training can be maintained following the intervention.
The effect of progressive resistance training on TUG and 6MWT was not significant. Although muscle strength can affect mobility and gait, other factors such as balance also contribute. 20 Moreover, factors such as fear of falling might play important roles in individual’s walking performance, 23 with patients continuing to walk at lower gait speed to avoid falling or continuing habitual slow walking practices that may develop after the hip fracture.
Further, Latham et al. (2014), have previously established that to improve patient’s functional abilities, training should focus on specific tasks as opposed to general training. 9 Trials mostly commonly were focused on common strength and gait outcomes, but progressive resistance training programs may be of greater benefit to patients after hip fracture if they focus on training functional performance in activities of interest for the patient. Future trials should consider how to develop and incorporate higher intensity progressive resistance training that focuses on performance of functional tasks.
Study strengths include using meta-analysis to assess the weighted impact of the intervention on patient outcomes and also using meta-regression to try to delineate the impact of specific resistance program characteristics on outcome. We were able to identify a limited number of trials that reported the resistance training characteristics so that we could explore how intervention characteristics affected outcomes. The marked heterogeneity even amongst these trials in progressive resistance training program characteristics suggests that further work is needed to improve reporting in order to determine how to maximize the impact of resistance training for patients’ quality of life. However, we were able to identify important factors for clinicians and researchers to consider when developing and/or evaluating a resistance training program as our findings do suggest that higher progressive resistance training intensity, center-based programs may have more impact on patient outcomes.
Further, we avoided common pitfalls of meta-regression. We only explored study level characteristics to prevent ecological fallacy14,35 where average patient level characteristic (e.g., age), which may not reflect the true individual level characteristics, are evaluated in relation to study outcomes as was done in previous meta-regressions.6,7,13 In addition, we did not over-fit our meta-regression models as we only performed meta-regression when we had at least 10 trials reporting the outcome of interest. 36
However, we did not define the progressive resistance training program characteristics that we were going to explore using meta-regression a priori as the first objective of our review was to determine what program characteristics were being reported in current randomized trials.14,35 This limitation may have created potential for misleading conclusions in our meta-regression, so we encourage further evaluation of program characteristics to identify those associated with better patient outcomes. Further, despite the numerous systematic reviews that examine the impact of rehabilitation programs after hip fracture,4,6,7,10,12,13 we were constrained in our evaluation that focused on the progressive resistance training component by the limited number of trials that reported specific resistance training program characteristics. Hence, our meta-regression was limited and we were unable to perform meta-regression to determine the longer-term impact of progressive resistance training programs.
Conclusions
The current study suggests that while progressive resistance training programs are associated with at least short-term benefits in strength and gait speed, the effect of resistance training after program completion requires more evaluation as it appears that these positive benefits may reduce over time. Only a small number of trials performed assessments over time after the intervention ended, so further work is required to determine if program benefits can be maintained. Higher progressive resistance training intensity and center-based resistance training programs may also be associated with higher strength gains and improved gait speed immediately following the intervention.
While this review provides further insights into progressive resistance training program characteristics that impact strength and gait outcomes, it also demonstrates the need for larger high quality trials with carefully constructed and reported rehabilitation program parameters focused on outcomes of interest for the patient. While improvement in strength is beneficial, a focus on using progressive resistance training for functional performance and mobility may be of more importance for patients. Given the increasing number of hip fractures, it is essential to improve rehabilitative interventions to benefit patients, caregivers, and health care systems.
Supplemental Material
Supplemental Material - Progressive Resistance Training Program Characteristics in Rehabilitation Programs Following Hip Fracture: A Meta-Analysis and Meta-Regression
Supplemental Material for Progressive Resistance Training Program Characteristics in Rehabilitation Programs Following Hip Fracture: A Meta-Analysis and Meta-RegressionAilar Ramadi by Victor E Ezeugwu, Sydnie Weber, Martha Funabashi, Monica Rodrigues Perracini, Lauren A Beaupre, and Camila Astolphi Lima in Geriatric Orthopaedic Surgery & Rehabilitation.
Footnotes
Acknowledgments
We would like to acknowledge the work of SH Kang in undertaking the meta-analyses and meta-regression reported in this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Alberta Health Service Seniors Health Strategic Clinical Network grant number (RES0036510).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.