
Abstract
Introduction
The objective of the present study is to assess the impact of the triglyceride-glucose index (TyG index) on the prognosis and explore the correlation between the TyG index and all-cause mortality in femoral neck fracture patients.
Materials and Methods
In this retrospective cohort study, we analyzed the TyG index in the follow-up of femoral neck fracture patients who underwent partial hip prosthesis. The formula of ln [fasting triglycerides (mg/dL) x fasting blood glucose concentration (mg/dL)/2] was used in the calculation of the TyG index. The patients were separated into three categories based on the TyG index.
Results
It was found that there was a significant correlation between prolonged hospital stay and elevated admission and postoperative TyG index (P = 0.011, P < 0.001, respectively). The Kaplan-Meier survival analysis curves revealed a higher risk of 30-day, 90-day and overall mortality in patients with higher postoperative TyG index levels, categorized by postoperative TyG tertiles (log-rank P < 0.001, P < 0.001 and P = 0.001, respectively). In the multivariate Cox proportional hazard models, higher postoperative TyG index was a significant risk factor for mortality (P = 0.01). The receiver operating characteristic analysis indicated that a postoperative TyG index of 9.01 and above was critical for 30-day mortality (69% sensitivity, 82% specificity and 0.78 area under curve; P < 0.001).
Conclusions
In our study demonstrate that the TyG index may be useful in identifying individuals at high risk of mortality in patients with femoral neck fractures.
Keywords
Introduction
The identification of reliable risk factors causing mortality and morbidity for osteoporotic hip fracture, which imposes a substantial economic burden as a worldwide public health issue, enables the prediction of postoperative adverse outcomes. 1 With the anticipated rise in the number of hip fractures in the years to come, it is important to acquire more information about specific death causes, whether some could be prevented and the causes of excess mortality, including comorbid conditions. 1 It is known that changing metabolic profile plays a significant role in the pathogenesis of cardiovascular disease (CVD) and causes early mortality. 2 However, the impact of metabolic parameters on mortality in hip fracture patients is yet to be fully known. 3
DM is regarded to be one of the significant risk factors of mortality for hip fracture. 4 Previous studies have reported that the risk of hip fracture increases by 1.3 to 2.1-fold in patients with type 2 DM.5,6 IR is the state of diminished sensitivity to the effects of insulin, and for several years, it has been defined as a predictor of type 2 DM development. Insulin resistance (IR) refers to the disruption in the biological response that occurs against insulin hormone. 7 The hyperinsulinemic euglycemic (HIEG clamp) test is the gold standard method for measuring IR. 8 In addition, other test tools have been employed for this purpose, including homeostasis model assessment-insulin resistance (HOMA-IR), quantitative insulin sensitivity check index (QUICKI) and triglyceride to high-density lipoprotein cholesterol (TG/HDL-C) ratio9,10. However, recently, the TyG index obtained with the help of triglyceride (TG) and fasting blood glucose levels has been proposed as a reliable IR marker, compatible with the gold standard method, due to both its cost-effectiveness and ease of use. 11
The TyG index has been increasingly investigated as a simple and reliable marker of adverse effects in some cardiovascular disorders. 7 Some recent studies have discovered that high TyG index could be an independent risk factor for all-cause mortality in patients with various cardiovascular disorders. 7 This index also serves as an IR marker associated with bone metabolism. IR is closely related to metabolic syndrome (MetS). There is also a close correlation between the TyG index and MetS and its components. 12 Hip fractures and MetS are becoming major global health problems as societies age. 13 MetS has been recently found to be significantly associated with postoperative morbidity and mortality in patients undergoing various surgeries.14,15 Despite numerous studies reporting a link between Metabolic Syndrome (MetS) and the acceleration of osteoporosis development and a simultaneous increase in the risk of fractures, the literature concentrating on the effect of MetS on postoperative outcomes after hip fracture surgery is mostly lacking.16,17
The identification of reliable perioperative risk factors enables the early prediction of adverse postoperative outcomes in hip fracture patients in clinical practice. However, in femoral neck fracture patients, the predictive value of the TyG index on the early and late mortality following partial hip replacement surgery remains uncertain. The aim of the present study is to investigate the impact of the TyG index in predicting the risk of postoperative mortality (30-day, 60-day and overall mortality).
Material and Methods
The study was designed as a retrospective cohort study after obtaining approval from the local ethics committee (24-KAEK-032). The follow-up period in the study was determined until the patients’ death or their last hospital contact by December 31, 2022.
Patients who were diagnosed with femoral neck fracture and underwent partial hip replacement surgery in a tertiary care teaching hospital between January 2011 and December 2020 were evaluated for inclusion.
The data used in the study were retrieved form the preoperative anesthesia records and medical files of the patients using the electronic patient record system (Enlil Hospital Information Management System, Version V2.19.46 20191118) and PACS software (Sectra Workstation Ids7, Version 21.2.11.6289; ©2019 Sectra Ab).
The patients who were treated with partial hip prosthesis for femoral neck fracture were identified from the Enlil Hospital Information Management System with the use of the ICD code. Demographic information of the patients was recorded. Date of death, gender, age, body mass index (BMI), American Society of Anesthesiologists (ASA) score, comorbidities, Charlson Comorbidity Index (CCI), intensive care unit (ICU) need, time to surgery (day), blood transfusion requirement (unit), duration of hospital stay, duration of postoperative ICU stay, blood biochemical and hematological parameters at admission and postoperative biochemical and hematological parameters were assessed. Death data were acquired from the national population management system. Inclusion criteria involved all patients aged 60 years and above with the primary diagnosis of femoral neck fracture who underwent surgical treatment with hip hemiarthroplasty.
Cases of hip fractures that were either not surgically treated or were surgically treated with osteosynthesis and total hip arthroplasty (THA), those with bilateral hip fractures, fractures extending to the subtrochanteric region or the femoral shaft and those with pathological and multi-traumatic multiple fractures, individuals who underwent hip surgery for reasons other than primary hip fracture (such as osteoarthritis, trauma, tumor metastasis, infection, or avascular necrosis of the femoral head), patients with active infections or hematological diseases, cancer patients undergoing chemotherapy, those with severe cognitive impairment and patients with incomplete clinical data or missing triglyceride and glucose data, were excluded from the study.
Since the study was conducted retrospectively, informed consent was waived. Duration of hospital stay above the 75th percentile were regarded as prolonged hospital stay.
BMI was calculated as mass (kg) divided by the square of height (m2). The patients were divided into four groups according to ASA score. After assessing the patients’ CCI scores, they were separated into three groups: in the first group, there were no comorbidities, classified as none; in the second group, there was one comorbidity, classified as low; and in the third group, there were two or more comorbidities, classified as high. Follow-up period was defined as the time from hospital admission to death or last follow-up date.
The patients included in the study continued to take drugs they use regularly for their comorbidities. In addition, after the surgery, subcutaneous enoxaparin sodium was given daily, and anti-embolism stockings were administered for deep vein thrombosis prophylaxis. The patients were followed up monthly for the first three months, then every six months and annually thereafter.
Blood samples were collected in the morning session after at least nine hours of overnight fasting. Following overnight fasting, venous samples for plasma glucose and lipid measurements were typically obtained by aseptic technique. All blood samples were analyzed on the blood analyzer device used for determining complete blood count in our laboratory.
The patients were categorized into five groups according to hemogram value at admission (group 1: ≤ 10; group 2: 10.1-10.9; group 3: 11.0-11.9; group 4: 12.0-12.9; group 5: ≥ 13.0). The TyG index was defined as TyG = ln [fasting triglycerides (mg/dL) x fasting glucose (mg/dL)/2] [11].
The admission TyG index was calculated based on the fasting glucose and triglyceride levels obtained at the latest one month before the onset of fracture. The postoperative TyG index, on the other hand, was found from the fasting glucose and triglyceride levels obtained within the first 2-5 days after the surgery.
The mortality of the patients was evaluated at 30-day, 90-day and final follow-ups.
The patients were divided into five groups by age (group 1: 60-74; group 2: 75-79; group 3: 80-84; group 4: 85-89; group 5: 90+).
Statistical Analysis
Continuous variables were presented as mean ± SD or median (Interquartile range) according to data distribution, whereas categorical variables were expressed as proportions.
The Kolmogorov-Smirnov test was employed to evaluate the normality of continuous parameters.
The analysis of continuous variables with nonnormal distribution was performed using Mann–Whitney U-test or Kruskal–Wallis test.
Kaplan-Meier survival analysis was employed to assess the incidence rate of endpoints among groups based on different levels of the TyG index, and their differences were assessed through log-rank tests.
Cox proportional hazards models were used to calculate the hazard ratio (HR) and 95% confidence interval (CI) between the TyG index and endpoints, and also adjusted for some models.
Confounding Variables included Variables selected based on p Value.
The receiver operating characteristic (ROC) curves were analyzed to determine the cutoff value of the TyG index.
Results
After applying Figure 1 the study’s exclusion criteria, a total of 136 patients (87 females and 49 males) with fully accessible TyG index values and follow-up records were included in the study. The median follow-up duration was 759 (195-1195) days. At the final follow-up, 41.9% of the patients had died. The mean age of the patients was 77.22 ± 7.82 years. According to the CCI, 30.1% were classified as none, 25.7% as low and 44.1% as high. Comorbidities of the patients’ are shown in Figure 2. Flowchart of femoral neck fracture identification. Comorbidities of all patients included in the study. HF: hearth failure; CRF: chronic renal failure; CVD: cardiovascular disease; CAD: coronary artery disease; COPD: Chronic obstructive pulmonary disease; DM: diabetes mellitus.

30-day mortality
Twenty-one point three percent of the patients had died within the first 30 days. The median survival time of the patients in the 30-day mortality group was 8 [Q1-Q3: [6-14] day. The first 30-day mortality was higher in males (P = 0.001), in patients requiring ICU care (P = 0.020), those necessitating blood transfusion (P < 0.001) and those with high ASA score (P < 0.001). Among the patients who died within the first 30 days, time to surgery was longer in the deceased patients (median: 5 Q1-Q3: 4-6 day) than in the survivors (median: 3 Q1-Q3:2-4 day). The patients who died within the first 30 days stayed longer (median: 1 Q1-Q3:1-3 day) in the ICU than survivors (median: 1 Q1-Q3:0-1 day) (P = 0.004).
Overall mortality
The median age was 79 [73-85] years in the deceased patients and 74 [71-83] years in the survivor group. In the final follow-up, the median survival time was 60 [8-510] days. The mortality rate was higher in males (P = 0.002), those requiring ICU care (P = 0.036), those necessitating blood transfusion (P = 0.034), those with low hemoglobin levels at admission (P = 0.007) and those with high ASA score (P < 0.001). The factors significantly affecting overall mortality were time to surgery (P < 0.001), duration of ICU stay after surgery (P = 0.003), amount of blood transfusion (P < 0.001) and age (P = 0.049).
The mean duration of hospital stay was 9.24 ± 6.19 days. Prolonged hospital stay was found in 32.4% of the patients. It was significantly influenced by the following factors: the duration of stay in ICU after surgery (P < 0.001), ASA score (P < 0.001), being in the high CCI group (P < 0.001), presence of CAD (P = 0.001), and diabetes (P = 0.001). Among those with prolonged hospital stay, the time to surgery (P < 0.001) and duration of ICU stay (P < 0.001) were longer.
It was observed that those with high admission TyG had higher weights (P < 0.001) and higher BMI values (P < 0.001).
Distribution of Qualitative Variables by Admission and Postoperative Tertiles Groups.

Pearson chi-square test was used. (abc): Common letters in the same row indicate insignificant difference.
ICU: intensive care unit; ASA:American Society of Anesthesiologists; CCI: Charlson Comorbidity Index.
In the overall mortality group, the median TyG index at admission was 8.95 [8.45-9.4] in the deceased patients and 8.92 [8.61-9.44] in those who survived (P = 0.353) (Table 1).
Distribution of Qualitative Variables by Admission and Postoperative Tertiles Groups.

Kruskal Wallis test was used. ICU: intensive care unit; BMI: Body mass index.
The patients with high postoperative TyG index were observed to stay longer in the hospital, have longer time to surgery (P < 0.001) and require longer postoperative ICU stay (P < 0.001) (Tables 1 and 2).
In the 30-day mortality group, the postoperative TyG index was higher in the deceased patients (9.37 [9.1-10.09]) than in those who were alive (8.72 [8.11-9.31]) (P < 0.001). Similarly, the postoperative TyG index values of the deceased patients (median: 9.4 [9.18-10.08]) was higher compared to that of the alive patients (9.06 [8.61-9.81]) in the overall mortality group (P = 0.003). The postoperative TyG index was 10.22 [9.81-10.56] in those at or above the 75th percentile of prolonged hospital stay, while it was 9.18 [8.67-9.37] in those below the 75th percentile (P = 0.011) (Tables 1 and 2).
The Kaplan-Meier survival curve estimation for the admission TyG index did not reach statistical difference between the groups (Figure 3). The patients with a higher admission TyG index did not have a higher risk of 30-day, 90-day and overall mortality. Within the 30-day, 90-day, and overall mortality groups, there was no significant difference in terms of the admission TyG index. (log-rank P = 0.97, P = 0.88, P = 0.65, respectively). Kaplan-Meier survival analysis curves for the relationship between the admission TyG index and mortality: (a): 30-day mortality (b): 90-day mortality (c): overall mortality.
The Kaplan-Meier survival analysis curves for the primary outcomes among the groups, based on the postoperative TyG index tertiles, are presented in Figure 4. The patients with a higher postoperative TyG index had a higher risk of 30-day, 90-day and overall mortality. (log-rank P < 0.001, P < 0.001, P = 0.001, respectively). Kaplan-Meier survival analysis curves for the relationship between the postoperative TyG index and mortality. (a): 30-day mortality (b): 90-day mortality (c): overall mortality.
Cox Regression Analysis.

In the 90-day mortality, a one-unit increase in the postoperative TyG index in the tertile 2 yielded 1.099 times higher mortality than in the tertile 1. The results of the unadjusted model indicated that the postoperative index was a significant risk factor for 90-day mortality (HR: 1.099; 95% CI: 1.025-1.397; P = 0.001). Again, mortality in the tertile 3 was 1.032 times higher with a one-unit increase in the postoperative TyG index compared to tertile 2. Higher tertiles of postoperative TyG index were significantly associated with higher risk of 90-day mortality in the unadjusted model of Cox proportional hazard model (HR: 1.032; 95% CI: 1.009-1.109; P < 0.001).
On examining the results obtained for the overall mortality, a one-unit increase in the postoperative TyG index in the tertile 2 resulted in 1.173 times higher mortality compared to the tertile 1, and the postoperative TyG index was a significant risk factor for overall mortality in the unadjusted model (HR: 1.173; 95% CI: 1.070- 1.425; P < 0.001). In a similar way, mortality increased 1.079 times in the tertile 3 with a one-unit increase in the postoperative TyG index compared to the tertile 2, and there was a significant association with higher tertiles of the postoperative TyG index and higher risk of overall mortality in the adjusted model of Cox proportional hazards models (HR:1.079; 95% CI: 1.032- 1.191; P < 0.001) (Table 3).
We evaluated the clinical efficacy of the TyG index using ROC analysis (Figure 5). The admission TyG index cut-off value of ≥ 8.79 predicted prolonged hospital stay with 77% sensitivity and 47% specificity, however, the area under curve (AUC) of the TyG index (0.64) was not good enough. ROC curve of admission and postoperative TyG index for prolonged hospitalization.
The postoperative TyG index cut-off value of ≥ 9.66 predicted prolonged hospital stay with the sensitivity of 82% and the specificity of 86% (AUC 0.89).
A statistically significant cut-off value for the admission TyG index could not be calculated for the 30-day mortality group in the ROC curve analysis (P = 0.745) (Figure 6). However, the cut-off value above 9.01 for the postoperative TyG index predicted prolonged hospital stay with 69% sensitivity and 82% specificity (AUC 0.78; P < 0.001). ROC analysis results of admission and postoperative TyG index ROC. (a): 30-day mortality (b): 90-day mortality c: overall mortality.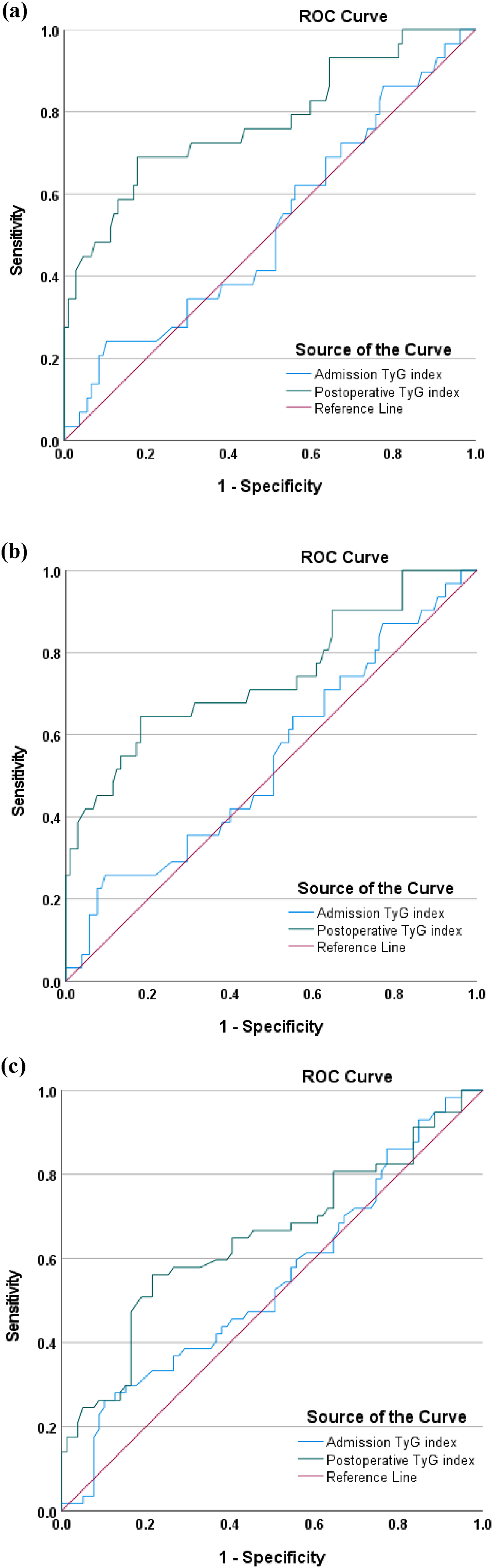
In the ROC curve analysis for the 90-day mortality group, a statistically significant cut-off value for the admission TyG index could not be determined (P = 0.49) (Figure 6). On the other hand, the cut-off value above 9.01 for the postoperative TyG index predicted prolonged hospital stay with 65% sensitivity and 82% specificity (AUC: 0.74; P < 0.001)
For the overall mortality group, a statistically significant cut-off value for the admission TyG index was not able to be established in the ROC curve analysis (P = 0.35), whereas the postoperative TyG index cut-off value above 9.12 predicted prolonged hospital stay with a sensitivity of 56% and a specificity of 78% (AUC: 0.65; P = 0.003) (Figure 6).
Discussion
It is essential to identify mortality risk factors in hip fractures. In the present study, we evaluated the relationship between the TyG index and prolonged hospital stay as well as all-cause mortality, in patients who underwent partial hip replacement surgery due to femoral neck fracture. These findings demonstrate that the TyG index may be useful in identifying individuals at high risk of mortality in patients with femoral neck fractures. Our findings may guide clinicians in normalizing postoperative glucose or triglyceride levels within the target range. To the best of our knowledge, this is the first study to investigate the impact of the TyG index on outcomes, focusing on both short-term and long-term mortality, in patients treated with partial hip prosthesis after femoral neck fracture. Therefore, it is challenging to compare the obtained results with those of other studies. The results indicated that the rise in the TyG index is significantly associated with higher risk of 30-day, 60-day and overall mortality, independent of potential risk factors.
When survival analysis methods like Cox regression were employed, the postoperative TyG index was associated with mortality independently of whether the TyG index is considered as a continuous or categorical variable. Additionally, we identified an increase in the postoperative TyG index as a marker of prolonged hospital stay. These findings emphasize the usefulness of an increase in the postoperative TyG index, which is simple and easy to calculate, for early identification of patients at high risk of developing serious outcomes such as prolonged hospital stay and mortality after undergoing treatment for femoral neck fracture. In general, the TyG index is related to lipid and glucose metabolism disorder. 18 It has been demonstrated that the metabolic status of a hip fracture patient considerably increase metabolic demand due to the trauma suffered by the patient, 2 and surgical procedures also induce a catabolic state in patients. 3 In hip fracture patients, the impact of postoperative changes in metabolic parameters on mortality is yet to be fully known. We attribute the greater impact of the postoperative TyG index than the admission TyG index on mortality and prolonged hospital stay, which emerged in our study, to this catabolic effect induced by surgery. IR is a significant risk factor for cardiometabolic diseases and a determinant value in type 2 DM. When compared to lower TyG index, a higher TyG index has been associated with an elevated incidence of coronary artery disease, myocardial infarction and CVD. 7
One of the parameters used in the calculation of the TyG index is fasting blood glucose. Both type 1 and type 2 diabetes has been found to be linked with increased risk of bone fracture.6,19 In hyperglycemia, it has been asserted that advanced glycation end products binding to bone collagen and oxidative stress compromise bone quality, which in turn can increase the risk of hip fracture.20-22 A cohort study based on population by Tebé et al 4 showed that type 2 DM patients had a higher risk of mortality, hip fracture and mortality after hip fracture compared to matched participants without type 2 DM. Recently, there is increasing evidence suggesting that preoperative glycemic control alone is not solely responsible for adverse outcomes, and that postoperative control is also an important factor requiring further research.23-25 Monnier et al. reported that the change in glucose concentration exhibits greater oxidative stress compared to continuous hyperglycemia. 26 These results may support our finding that the postoperative TyG index, rather than the preoperative TyG index, is effective on outcomes.
Another parameter used in the calculation of the TyG index is blood triglyceride level. Chang et al. stated that the risk of non-traumatic fracture increased by 2 to 2.5 times in midlife women with fasting plasma TG levels of at least 300 mg/dl. 27 In studies in the literature, elderly hip fractures have been linked to an increased risk of falls due to decreased muscle strength associated with increased serum triglyceride concentrations. 28 Compared to individuals without vertebral fractures, vertebral fracture patients exhibited a higher average marrow fat content (lipid-water ratio), 29 with the majority consisting of TG 30 The variability in bone marrow lipid-water ratio may be partially attributed to circulating TG 31 It is reasonable that there is an association at least partially between circulating TG levels and fracture, because it denotes higher content of bone marrow fat. Norring et al detected a significant relationship between 30-day mortality and the elevated quartiles of TG/HDL-C. 32 These studies may present evidence for the impact of the postoperative TyG index on mortality, which we found in our study.
Mortality risk due to heart disease and complications related to comorbidities typically increases in MetS patients.33,34 IR is closely associated with MetS . 12 MetS has been shown to have a significant impact on outcomes and mortality of trauma patients. Tracy et al. reported that there were increased rates of cardiovascular morbidity associated with MetS, and that MetS patients had significantly longer duration of hospital and ICU stay and spent more time on mechanical ventilation. In addition, MetS has been linked to higher rates of out-of-home discharge and mortality. 16 Many population-based studies published recently have indicated that the presence of MetS was related to low bone mineral density13,15 and simultaneously to a higher risk of fragility fractures.14,17 MetS has been also associated with higher adverse hospital outcomes, elevated expenses, prolonged hospital stay and non-standard discharge risks.35-37 Gandhi et al determined elevated incidence of complications in patients with MetS undergoing THA compared to those without MetS. 38 Edelstein et al reported that MetS was associated with prolonged hospital stay after THA. Menendez et al. found that MetS had a significant relationship with higher rates of postoperative complications and out-of-home discharge following ankle fractures. 39 Li et al. indicated that in hip fracture patients, overweight and obese ones had a significantly lower risk of mortality compared to those with normal body weight. They also noted that there existed an “obesity paradox” in hip fracture patients, and the abundant amount of adipose tissue serves as a reservoir for surplus calories in the form of triglycerides released during the highly catabolic state following injury. 40 On the other hand, Amin et al 41 stated that the obesity paradox in hip fracture patients does not universally hold and that the presence of the obesity paradox is observed only in hip fracture patients aged 75 years and older. They pointed out that in patients under the age of 75 years, those with class I (BMI: 30-34.9 kg/m2) and class II obesity (BMI: 35-39.9 kg/m2) did not exhibit a higher mortality risk as compared to those with normal BMI; however, there was a significant association between class III obesity (BMI: 30-39.9 kg/m2) and a higher mortality risk.
The findings of our study indicating that the postoperative TyG index is more effective on mortality than the admission TyG index may provide an explanation for this paradox. A greater amount of triglyceride is released into circulation as a result of increased catabolic effect after surgery and our current data suggest that postoperative measurements are more important than preoperative measurements.
The present study had certain limitations. First, it was conducted retrospectively in a single center. Due to its retrospective nature, it is not possible to establish an exact relationship between the change in blood parameters and outcomes. The size of the sample included in the study was small. This is because triglyceride measurement is not routinely performed. The patients with no data of TyG index excluded from the study, which may limit the generalizability of our findings. However, it should be noted that the completeness of the data is more important than the sample size being small. Another limitation is that drugs that may affect glucose and lipid metabolism were not taken into account. Another limitation is that lacks the data of nutritional assessment, 25-(OH) vitamin D and bone mineral density (BMD).The generalizability of the research findings to other races needs to be additionally evaluated. Finally, in our study, the manner of death of the patients was not listed.
In conclusion,ıt has been shown that the triglyceride-glucose index (TyG), a reliable marker of insulin resistance, is associated with adverse clinical outcomes in patients such as those with acute coronary syndrome, heart failure and ischemic stroke. However, the relationship between the TyG index and mortality in hip fracture patients is yet to be known. Our study highlights that the postoperative TyG index is positively correlated with hip fracture mortality and it may be used as an independent predictor for mortality. We identified a specific TyG index cut-off value related to increased mortality with TyG index. It is imperative to conduct future prospective studies in order to validate and expand our findings. Determining whether the improvement in the TyG index can reduce long-term mortality risk in future studies will help confirm the significance and practical implications of our findings.
Footnotes
Acknowledgements
We would like to thank the multidisciplinary team at Tokat Gaziosmanpasa Medical University Hospital, including our orthopedic colleagues, who took part in the preparation of this article and in the treatment planning and implementation.
Author Contributions
Data collection and/or processing: S.A, O.B.; Analysis and/or interpretation: S.A, O.B.; Literature search: S.A, O.B.; Writing: S.A, O.B.; Critical review: S.A, O.B.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The datasets provided in this study are available upon request by the corresponding author.