
Abstract
Introduction
Adherence to best practices for care of hip fracture patients is fundamental to decreasing morbidity and mortality in older adults. This includes timely transfer from the hospital to rehabilitation soon after their surgical care. Hospitals experience challenges in implementing several best practices. We examined the potential barriers associated with timely discharge for patients who underwent a hip fracture surgery in an academic hospital in Ontario, Canada.
Methods
We conducted a retrospective cross-sectional review of a local database. We used descriptive statistics to characterize individuals according to the time of discharge after surgery. Multivariable binary logistic regression was used to evaluate factors associated with delayed discharge (>6 days post-surgery).
Results
A total of 492 patients who underwent hip fracture surgery between September 2019 and August 2020 were included in the study. The odds of having a delayed discharge occurred when patients had a higher frailty score (odds ratios [OR] 1.19, 95% confidence interval [CI] 1.02;1.38), experienced an episode of delirium (OR 2.54, 95% CI 1.35;4.79), or were non-weightbearing (OR 3.00, 95% CI 1.07;8.43). Patients were less likely to have a delayed discharge when the surgery was on a weekend (OR .50, 95% CI .32;.79) compared to a weekday, patients had a total hip replacement (OR .28, 95% CI .10;.80) or dynamic hip screw fixation (OR .49, 95% CI .25;.98) compared to intramedullary nails, or patients who were discharged to long-term care (OR .05, 95% CI .02;.13), home (OR .26, 95% CI .15;.46), or transferred to another specialty in the hospital (OR .49, 95% CI .29;.84) compared to inpatient rehabilitation.
Conclusions
Clinical and organizational factors can operate as potential barriers to timely discharge after hip fracture surgery. Further research is needed to understand how to overcome these barriers and implement strategies to improve best practice for post-surgery hip fracture care.
Keywords
Introduction
Hip fractures are common injuries that can occur at any age, but the risk increases as age advances, especially affecting older people. 1 By 2050, the global number of hip fractures is projected to increase to over 4.5 million per year. 2 This increasing numbers are associated with an aging population and factors such as decreased bone density, loss of muscle mass, and deterioration of coordination and balance. Hip fractures may impact on older people’s quality of life, morbidity, long-term care needs, and risk of mortality.3,4 Hip fracture management is also costly on the healthcare system. 5
Post-hip fracture surgery care is often provided across multiple health care sectors. Cohesive follow-up care is especially important to ensure ideal recovery and following best practice guidelines for care of hip fracture patients is fundamental to decrease morbidity and mortality in this population. Early referral for rehabilitation to start within six days after surgery is recommended,6-9 with inpatient rehabilitation being the gold standard for the recovery of hip fracture patients’ post-surgery. 10 In addition, early surgery (within 48 h of patient admission), early mobilization (within 24 h of surgery), full early weight bearing, decreased polypharmacy, minimizing foley catheter usage, and several other best practices exist.6-9 However, there are still limitations in adopting these procedures in the hospital setting including the lack of availability of operating rooms to perform the surgery in the recommended time, 11 long waitlists, bed shortages and limited funding for rehabilitation. 12
Despite these limitations, studies have shown that timely access to rehabilitation following hip fracture surgery leads to better patient outcomes.13,14 Thus, the purpose of this study was to examine the potential barriers associated with discharge from acute care for older patients who underwent a hip fracture surgery between September 2019 and August 2020 in a large academic hospital in Ontario, Canada.
Method
Study Design and Population
We conducted a cross-sectional retrospective study using the Operatively Repaired Hip Fracture database (ORFD). The ORFD is a local institutional database that consists of prospectively collected data. Patients were identified via ICD codes for a hip fracture (ICD-10-CA: S72.0, S72.1, or S72.2) sequentially over the period of a year. Once identified the remaining variables were manually extracted for each patient from electronic health records, operating room information systems and discharge summaries. The Research Ethics Board reviewed and approved this study. Results are reported in accordance with the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines. 15
Data from patients (60 years of age or older) who had a unilateral hip fracture (i.e., femoral (neck or head), intertrochanteric, subtrochanteric) and underwent surgery in an academic hospital in Ontario, Canada between September 2019 and August 2020 were included. Data from patients with multiple injuries, metastatic cancer diagnosis, on dialysis, or receiving chemotherapy and/or radiation treatments were excluded. We also excluded those who died during the hospitalization or those with missing or invalid data for birth date or discharge information.
Variables of Interest
Patient baseline characteristics included age, sex, place of residence before hospital admission (i.e., home, long-term care, retirement home), and pre-fracture health status (i.e., mobility, frailty and comorbidities).
Characteristics of the pre-surgery and surgery acute episode of care included: the type of fracture (i.e., femoral (neck (31-B) or head (31-C)), intertrochanteric (31-A), subtrochanteric), the presence of a pathological fracture, time from arrival to admission, the day of admission (i.e., weekday, weekend), time from admission to surgery, the surgery day (i.e., weekday, weekend), and the procedure type (i.e., hemiarthroplasty, total hip replacement, intramedullary nails, dynamic hip screws).
Characteristics of the post-surgery acute episode of care included: the completion of fall risk assessments and pressure ulcer examinations, the presence of post-surgery delirium, the weightbearing status, and the occurrence of complications (i.e., pneumonia, urinary tract infection, stroke, deep vein thrombosis, pulmonary embolism, surgical site infection). The number of alternative level of care (ALC) days, the discharge destination from the orthopaedic ward (i.e., long term care, home/retirement home/home with home care, other speciality in hospital, or inpatient rehabilitation), and the time from the rehabilitation consult requested to the rehabilitation consult completed were also captured.
The primary outcome was the proportion of patients who underwent surgery for a unilateral hip fracture and who experienced a delayed discharge from the acute care hospital (>6 days post-surgery). We defined day 6 at the cutoff point based on clinical expertise and published guideline. 16
Data Analysis
Potential factors associated with delayed discharge were grouped as barriers to discharge related to the patient characteristics, or the clinical team and hospital management. We used descriptive statistics to characterize individuals according to the timeliness of discharge (i.e., delayed discharge or timely discharge). Mean and standard deviation were used for continuous variables, and absolute and relative frequency for categorical variables. Multivariable binary logistic regression was used to evaluate factors associated with delayed discharge and estimates were expressed as odds ratios (OR) and 95% confidence intervals (CI). All independent variables were simultaneously included in the model. Variance inflation factor (VIF) was used to inspect multicollinearity and no issues were detected. All analyses were performed with Stata version 14.2, and only complete records were included.
Results
Of the 606 patients’ records extracted for analysis, 114 were excluded from our analysis including patients less than 60 years of age (n = 43), patients who died during hospitalization (n = 38), or patients who had missing or invalid data relevant to discharge (n = 33), leaving a final sample of 492 patients included in the study.
Patient Baseline Characteristics
Baseline Characteristics of the Patients According to Days From Surgery to Discharge.

Pre-surgery and Surgery Acute Episode of Care
Characteristics of the Acute Episode of Care According to Days From Surgery to Discharge.

aAlternate Level of Care (ALC) days are defined as days where patients occupy acute care beds when they do not require the intensity of the services provided.
bMissing values calculated based on the total number of patients discharged to inpatient rehabilitation (N = 168).
Post-surgery Acute Episode of Care
Fall risk assessments were performed on 98.4% (n = 484) and pressure ulcer examinations were recorded on 90.7% (n = 446) of patients. Post-surgery delirium was developed in 18% (n = 84) of the patients. One third of patients experienced complications, with the most prevalent being urinary tract infections (14.1%, n = 69), pneumonia (6.1%, n = 30), and falls (5.3%, n = 26). As for the discharge destination from the orthopaedic ward, 34.1% (n = 168) of patients were discharged to geriatric rehabilitation, with an average wait time of 1.5 days (±2 days) post-request of their rehabilitation consult (Table 2).
Delays in Discharge (>6 Days Post-Surgery)
A total of 58% (n = 286) of patients who underwent surgery for a unilateral hip fracture experienced a delayed discharge from the acute care hospital (>6 days post-surgery).
Potential Barriers to delayed Discharge
The odds of having a delayed discharge occurred when patients (1) had a higher frailty score (OR 1.19, 95% CI 1.02;1.38), (2) experienced an episode of delirium (OR 2.54, 95% CI 1.35;4.79), or (3) were non-weightbearing (WB) (OR 3.00, 95% CI 1.07;8.43).
Association Between Characteristics of the Patients and Delayed Discharge (Adjusted Model).
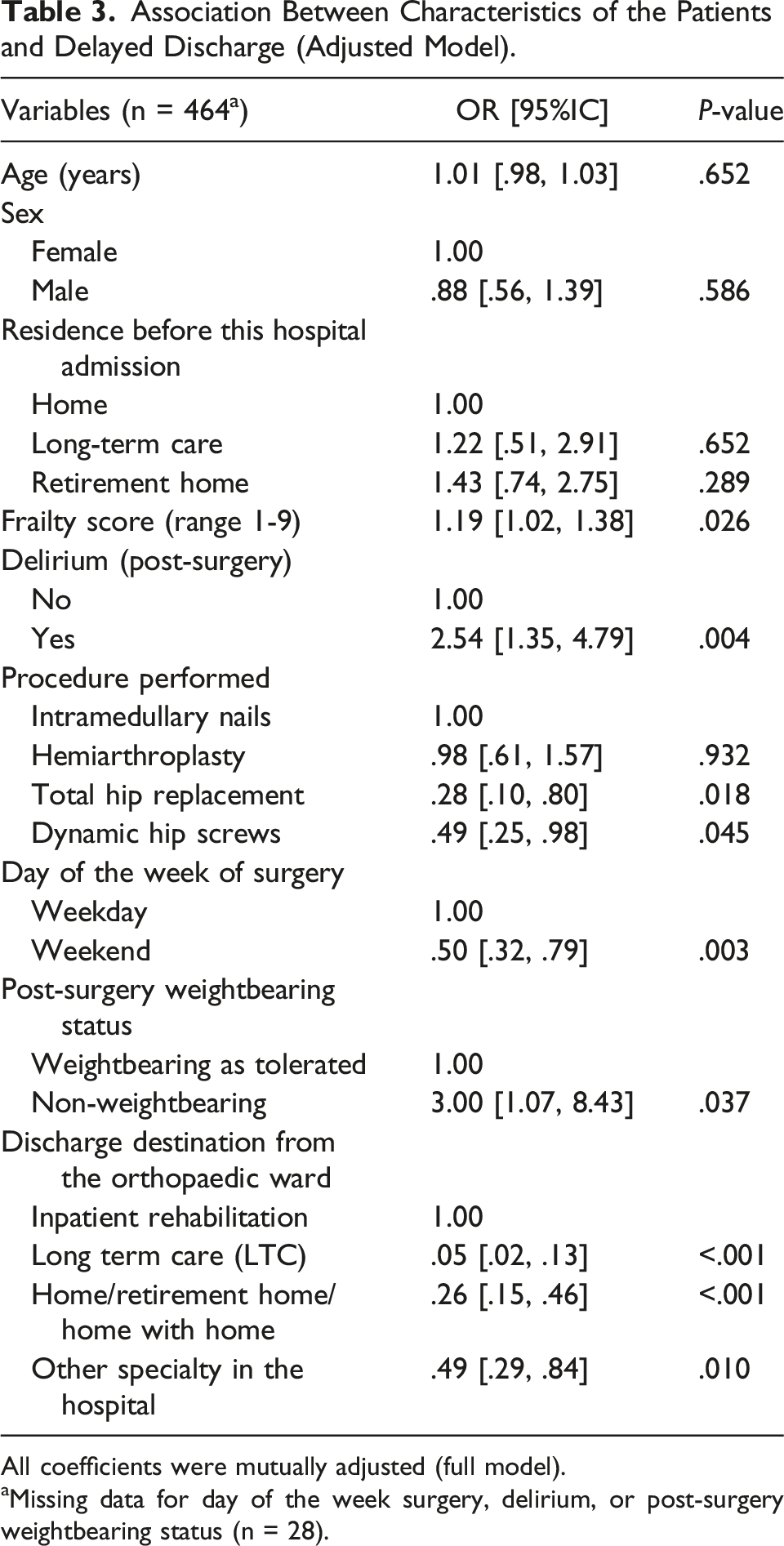
All coefficients were mutually adjusted (full model).
aMissing data for day of the week surgery, delirium, or post-surgery weightbearing status (n = 28).
Discussion
This study examined the potential barriers associated with delayed discharge to rehabilitation for patients who underwent a hip fracture surgery in a large academic hospital in Ontario, Canada. Potential barriers associated with delayed discharge included patients with higher frailty scores, the occurrence of post-surgery delirium, or having a non-weight bearing status. Factors that reduced the odds of a delayed discharge included a weekend surgery, a total hip replacement or dynamic hip screw fixation, discharge destination to long-term care, home or to another specialty in the hospital.
Potential Barriers Associated with Patient Characteristics
Patients with higher frailty scores may have delay in discharge for various reasons. These patients are more likely to experience complications 17 requiring a prolonged stay in the acute care setting. In fact, frail patients are likely to benefit most from early rehabilitation. 18 A clear inclusion and exclusion criteria for referral to geriatric rehabilitation post-surgery for this frail group should be explored.
Post-surgery delirium was also a potential barrier to timely discharge. Data from the UK showed that delirium has significant detrimental effect on more medium-term rates of returning home and returning to mobility – underlining the seriousness of this complication and importance of avoiding it. 19 A proactive approach to avoid delirium in the perioperative period may help decrease the incidence in these patients. 20 In addition, patients with delirium often do not need to be delayed from discharge to a rehabilitation centre. Nurses and physicians at most rehabilitation facilities are often very experienced at dealing with this issue that almost always resolves with appropriate treatment. 21 We also note that the delirium rates in our study population was low (only 18%) compared to the general hip fracture population (estimated to usually be 40-60%). This suggests the likelihood that milder cases of delirium were not identified. Thus, this could be overestimating the impact of delirium on the transfer – as the most agitated patients were likely identified. Nonetheless, delirium is frequently identified as a reason for delays in starting rehabilitation. A clear criterion is needed to ensure appropriate support are in place to manage delirium-related behaviours in rehabilitation facilities.
Potential Barriers Associated with The Clinical Team and Hospital Management
“Day of week delays” may suggest that although hip fracture patients arrive to the emergency department seven days a week, the expedient transfer to the geriatric rehabilitation facility may not flow as smoothly throughout the week. Charge nurses, discharge planning coordinators and social workers often only work on a hospital ward five days a week (Monday to Friday). Another issue could potentially be the tendency for rehabilitation discharges to occur later in the week. Further analysis of contributing factors to increased length of stay for these patients would be helpful and could introduce savings by improving the utilization of surgical beds.
In addition, patients who went to rehabilitation experienced more delays than those who went home or to long-term care. This supports the implementation of an evidence-based pathway such as PATH FOR timely transfer of geriatric HIP fracture patients from hospital to rehabilitation to home (PATH4HIP) 22 that facilitates the earlier identification and transfer of patients to rehabilitation. The national care model for hip fracture surgery’s goal is to refer 65% of patients to rehabilitation, 10% to home discharge and 20% to LTC. 16 In this study, 34.1% of patients were referred to rehabilitation, 24.8% to home discharge, and 10.8% to LTC. The in-hospital mortality rate was 7.72% (n = 38), higher than the expected 5%.
Delayed discharge of hip fracture patients has significant implications for both patient care and the healthcare system. This can lead to increased mortality 23 and increased financial burden on the healthcare infrastructure, ranging from CAD $21 000 for individuals discharged home to CAD $47 000 for those discharged to LTC. 16
Strengths and Limitations
Data collection during the COVID lockdown, may have altered the composition of types of falls and the types of patients who were falling. Particularly, since exercise classes and activities were cancelled, and the well older adults were confined indoors, and less likely to fall unlike frail older adults who often fall in their living environment. This is a relatively small study from a single academic hospital and may have been under powered to detect some associations studied. In addition, this was a retrospective study, therefore, the recall of the patients’ pre-existing function and frailty status may not be as accurately captured.
Despite these limitations, this study has allowed us to identify some potential barriers to discharge with a large sample size of post-surgery hip fracture patients. The results of this study do not provide information on causality, but rather on the potential factors associated with delayed discharge.
Conclusion
The goal of care of hip fracture patients includes timely transfer to rehabilitation after successful surgery for most patients. Our results provide insights on the potential barriers to timely patient discharge after hip fracture surgery. Clinical and organizational factors can operate as barriers to timely discharge after hip fracture surgery. Further research is needed to understand how to address those barriers, involve patients and their families to better understand the importance of early rehabilitation, and implement strategies to improve best practice for post-surgery hip fracture care.
Footnotes
Author Contributions
Concept and design were done by C.B., C.W., A.H., P.T., and S.P.. Data acquisition and analysis were performed by C.B., F.D.E., A.L.S.F.M., G.M.M.L., and C.W.. Drafting of the manuscript was done by C.B. and F.D.E.. All authors critically revised the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.